

When people are diagnosed with Type 2 Diabetes they are often sent for Diabetes education which teaches them, among other things to “choose starchy foods such as whole grain breads and cereals, rice, noodles, or potatoes at every meal” and that “good management of diabetes includes healthy eating, staying active and taking required medication [1]”. There is certainly a need for medication when blood sugar levels are not being controlled but what if in other cases, as Hippocrates has said food could be our medicine?
Food As Medicine
A therapeutic diet is involved in the management and treatment of many diseases and conditions. When someone is diagnosed with Celiac disease, for instance they are taught by a Dietitian to avoid gluten-containing foods because these cause damage to their intestines. A therapeutic diet for someone with Celiac disease involves them avoiding gluten-containing foods and beverages because eating them causes damage to their body.
A therapeutic diet for someone that is diagnosed with a food allergy often involves them avoiding eating that food and related foods that may also cause an adverse reaction. If a person is allergic to banana, for instance they may also react to pineapple, papaya or chestnuts. Except in the case of serious (anaphylactic) allergies, after a person has avoided those foods for a long time, a “food challenge” may be done to determine whether the person is later able to tolerate the foods in question, or not. Sometimes foods are able to be reintroduced later and other times, such as the case of Celiac disease, they cannot because to do so will result in damage to their body.
A therapeutic diet in someone diagnosed with Type 2 Diabetes involves limiting foods that result in too much insulin being released and/or that results in their blood sugar rising too high and too often. This may be for a period of time – after which something that can be likened to a ‘food challenge’ can be performed to determine whether there has been significant improvement or not and if so, which kinds of carbohydrate may be able to be re-introduced, in what quantities and with what frequency. More on that below.
Evidence Base for Using Dietary Carbohydrate Restriction in Diabetes Management
A Critical Review Article written by 26 authors and researchers appeared in the Journal of Nutrition in 2015 provided 12 points of evidence to support the use of low-carbohydrate diets as the first approach to treating Type 2 Diabetes. The summary of these points include that;
- Hyperglycemia is the most salient feature of Diabetes and that dietary carbohydrate restriction has the greatest effect on decreasing blood glucose levels.
- During the epidemics of obesity and Type 2 Diabetes, caloric increases have been due almost entirely to increased carbohydrates.
- Benefits of dietary carbohydrate restriction do not require weight loss.
- Although weight loss is not required for benefit, no dietary intervention is better than carbohydrate restriction for weight loss.
- Adherence to low-carbohydrate diets in people with Type 2 Diabetes is at least as good as adherence to any other dietary interventions and is frequently significantly better.
- Replacement of carbohydrate with protein is generally beneficial.
- Dietary total and saturated fat do not correlate with risk for cardiovascular disease.
- Plasma saturated fatty acids are controlled by dietary carbohydrate more than by dietary lipids.
- The best predictor of microvascular and, to a lesser extent, macrovascular complications in patients with Type 2 Diabetes, is glycemic control (HbA1c).
- Dietary carbohydrate restriction is the most effective method (other than starvation) of reducing serum TGs and increasing high-density lipoprotein.
- Patients with Type 2 Diabetes on carbohydrate-restricted diets reduce and frequently eliminate medication (and people with Type 1 usually require lower insulin).
- Intensive glucose lowering by dietary carbohydrate restriction has no side effects comparable to the effects of intensive pharmacologic treatment.
The authors provided strong support of the 12 points, concluding that there is a need for “reappraisal of dietary recommendations” which stems from;
1. The general failure to halt the epidemic of Diabetes under current
guidelines,
2. The specific failure of low-fat diets to improve obesity, cardiovascular
risk, or general health (points 1 and 4),
3. Constant reports of side effects of commonly prescribed
Diabetes medications, some quite serious (points 12),
4. Most importantly, the continued success of low carbohydrate
diets to meet the challenges of improvement in the features of Diabetes and metabolic syndrome in the absence of side effects.
The authors underscore that
“the benefits of carbohydrate restriction are immediate and well-documented.”
and that
“Concerns about the efficacy and safety of carbohydrate restriction are long term and conjectural rather than data driven. Most objections stem from the proposed dangers of total or saturated fat embodied in the so-called diet—heart hypothesis. At this point, the diet—heart hypothesis has had a record of very limited clinical or experimental success to support its position.”
As I’ve mentioned in past articles, a low carbohydrate diet is not new, but may in fact represent the diet followed by humans for much of our evolutionary history, prior to the rise of agriculture. Given the very positive outcomes of carbohydrate restricted diets, the authors conclude that people with Type 2 Diabetes should not be discouraged from following such a diet as is often the case, but rather that the strength of the evidence is that;
“current knowledge dictates that carbohydrate restriction should be a default treatment for Type 2 Diabetes and a default adjunct therapy for Type 1.”
The authors state that the insistent by those that object to the use of low carbohydrate diets on the basis that long-term randomized controlled trials are the only kind of data that will be accepted “is without precedent in science.”
“The seriousness of diabetes requires that we evaluate all of the evidence that is available. The 12 points are sufficiently compelling that we feel that the burden of proof rests with those who are opposed.’
Authors of this Review included:
- Richard D. Feinman Ph.D, Department of Cell Biology, State University of New York
- Wendy K. Pogozelski Ph.D, Department of Chemistry, State University of New York
- Arne Astrup M.D., Department of Nutrition, Exercise and Sports, Copenhagen University
- Richard K. Bernstein M.D., New York Diabetes Center, Mamaroneck, NY
- Eugene J. Fine M.S., M.D., Department of Radiology (Nuclear Medicine), Albert Einstein College of Medicine, Bronx, New York
- Eric C. Westman M.D., M.H.S., Duke University Medical Center, Durham, NC
- Anthony Accurso M.D., Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore, MD
- Lynda Frassetto M.D. Department of Medicine, University of California San Francisco, San Francisco, CA
- Barbara A. Gower Ph.D. Department of Nutrition Sciences, University of Alabama at Birmingham, Birmingham, Alabama
- Samy I. McFarlane M.D., Departments of Medicine and Endocrinology, State University of New York Downstate Medical Center, Brooklyn, NY
- Jí¶rgen Vesti Nielsen M.D., Karlshamn, Sweden
- Thure Krarup M.D. Department of Endocrinology I, Bispebjerg University Hospital, Copenhagen, Denmark
- Laura Saslow Ph.D. University of California San Francisco, San Francisco, CA
- Karl S. Roth M.D. Department of Pediatrics, Creighton University, Omaha, NE
- Mary C. Vernon M.D. Private Practice, Lawrence, KS
- Jeff S. Volek R.D., Ph.D. Department of Human Sciences (Kinesiology Program) Ohio State University, Columbus, OH
- Gilbert B. Wilshire M.D. Mid-Missouri Reproductive Medicine and Surgery, Columbia, MO
- Annika Dahlqvist M.D. Hí¤lsocentralen Centrum, Sundsvall, Sweden
- Ralf Sundberg M.D., Ph.D. Private Practice, Malmí¶, Sweden
- Ann Childers M.D. Private Practice, Lake Oswego, OR
- Katharine Morrison M.R.C.G.P., Ballochmyle Medical Group, Mauchline, East Ayrshire, Scotland
- Anssi H. Manninen M.H.S. Metabolia Oulu, Oulu, Finland
- Hussain M. Dashti M.D., Ph.D., F.A.C.S., F.I.C.S., Faculty of Medicine, Department of Surgery, Kuwait university, Kuwait
- Richard J. Wood Ph.D. Springfield College, Springfield, MA
- Jay Wortman M.D. First Nations Division, Vancouver, BC, Canada
- Nicolai Worm Ph.D. German University for Prevention and Health Care Management, Saarbrí¼cken, Germany
Blood Sugar Response in Healthy People vs Actual Responses in Individual Diabetics
We have the Glycemic Index (GI) which tells us how easily specific foods raise blood sugar in healthy people; specifically how much blood sugar will rise when a healthy person eats 50 g of that food and Glycemic Load (GL) tells us how healthy people respond to the carbohydrate in one serving of that food.
As outlined in the previous two articles titled “Not All Carbs Are Created Equal“, while brown rice and whole grain spaghetti may have a lower GI or GL than their white counterparts, they still result in a rapid rise in blood sugar even in healthy people. Would we expect brown rice or whole grain spaghetti to have any better a response in those with Type 2 Diabetes? Of course not, yet the recommendations are for those with Type 2 Diabetes to eat “starchy foods such as whole grain breads and cereals, rice, noodles, or potatoes at every meal“.
Given that the symptom of Type 2 Diabetes is that body can’t properly use the insulin that is released and as a result “sugar builds up in the blood instead of being used as energy” [1] – how does it make sense to recommend to someone with Type 2 Diabetes to “eat starchy foods such as whole grain breads and cereals, rice, noodles, or potatoes at every meal” because these “starchy foods are broken down into glucose, which your body needs for energy”[1]? Either the body can’t use the food as energy because of the dysfunction in insulin or it can.
In Type 2 Diabetes, the mechanism in which the body effectively uses carbohydrates for energy is ‘broken’ and body keeps making and releasing more and more insulin to try and bring glucose into the cells. Common sense would indicate that a therapeutic diet for someone with an intolerance to more than very small amounts of carbohydrate would be to limit foods that are high in carbohydrate, particularly those that cause a rapid spike in blood glucose even in healthy people.
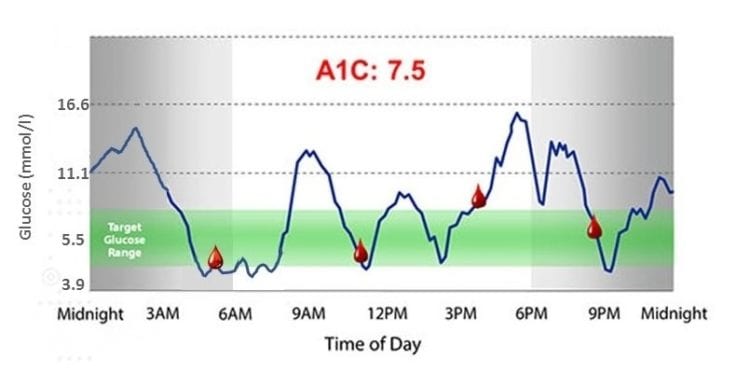
We don’t need to guess how much a person with Type 2 Diabetes’ blood sugar is going to rise when they eat a food based on the GI or GL (which is based on healthy people) because we can test it in THEM!
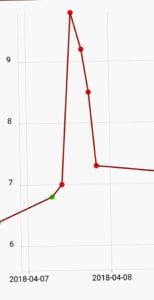 As mentioned in the previous article, without spending any additional money on testing equipment, someone with Type 2 Diabetes can eat 25 g or 50 g of a carbohydrate-based food, test their blood sugar every half hour and know exactly how their body responds to it! They can see their blood sugar rise to 11 mmol/L (200 mg/dl) or 14 mmol/L (250 mg/dl) or 16.5 mmol/L (297 mg/dl) or higher in the first hour and KNOW. No guess work is required!
As mentioned in the previous article, without spending any additional money on testing equipment, someone with Type 2 Diabetes can eat 25 g or 50 g of a carbohydrate-based food, test their blood sugar every half hour and know exactly how their body responds to it! They can see their blood sugar rise to 11 mmol/L (200 mg/dl) or 14 mmol/L (250 mg/dl) or 16.5 mmol/L (297 mg/dl) or higher in the first hour and KNOW. No guess work is required!
With the availability of relatively inexpensive Continuous Glucose Monitors (CGM) such as the FreeStyle Libre ($50 CDN) and one sensor worn for 2 weeks ($90), someone with Type 2 Diabetes can test 25 g or 50 g of specific carbohydrate-based food and KNOW exactly how their body responds!
People with Type 2 Diabetes can KNOW that 1/2 cup of whole grain rice or 1/2 of a baked potato (or some other food) resulted in their blood sugar spiking to 16.5 mmol/L (297 mg/dl) and know that this is not a food they tolerate even when eaten with a mixed meal that includes protein-based foods and non-starchy vegetables.
Guess work based on Glycemic Index or Glycemic Load – the blood sugar response of healthy people is no longer needed.
Role for a Therapeutic Low Carb Diet
Just as there is a role for a therapeutic diet in other food-related conditions such as food intolerance and Celiac disease, there is a role for a therapeutic diet in Type 2 Diabetes.
A person diagnosed with Type 2 Diabetes has (1) the inability to handle more than a very small carbohydrate load and (2) has cells which are insulin resistant, therefore it makes good clinical sense to design a therapeutic diet which enables them to lower their overall blood glucose response in order to enable the pancreatic beta cells that remain to begin to recover (these are the cells that produce insulin) and to allow their body cells which have become insulin resistant to become insulin sensitive again.
A Dietitian is knowledgeable to design such an therapeutic diet in such a ways as to include a wide variety of foods that supplies all the essential amino acids, fatty acids, vitamins and minerals that a person requires while containing only small amounts of carbohydrate at any given time.
Lab test results such as fasting insulin and fasting blood glucose (to calculate HOMA-IR) and tests of insulin response to a known glucose load (3 hour challenge) could be performed in time to monitor the degree of improvement in insulin sensitivity and pancreatic function or simply use existing routine lab tests such as TG:HDL ratio as a proxy, along with HbA1C and fasting blood glucose. This way, once a person’s body has begin to heal and restore some beta-cell function, a Dietitian can then design a customized therapeutic diet around each individual’s actual tolerance or intolerance to specific carbohydrates! We don’t need to rely on glycemic response data such as the GI or GL (which are based on healthy people) but can use an individual’s own blood sugar response!
We do this in other types of food intolerance by means of a “food challenge” and it is time we do this in Type 2 Diabetes as well.
With the advent of relatively inexpensive Continuous Glucose Monitors, we have the technology for individuals to do this easily with the help of a Dietitian, such as myself. It is more labour-intensive, but it can certainly be done using the standard blood glucose monitor that Diabetics already own and use by standardizing the size of the test food and testing blood sugar every 1/2 an hour for 3 hours.
It is long overdue for those with Type 2 Diabetes to be able to have therapeutic diets which are designed to improve their symptoms, rather than to expect them to eat carbohydrate loads they can’t handle, getting worse in time, then turning to medication to manage the disease. Type 2 Diabetes does not have to be “a chronic, progressive disease”.
Do you have questions how a low carb diet may be able to help you manage and improve the symptoms of Type 2 Diabetes?
Please send me a note using the ”Contact Me” form on this web page and I will respond shortly.
To our good health!
Joy
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
You can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
References
- Diabetes Canada, Diabetes and You, Basic Meal Planning, https://www.diabetes.ca/diabetes-and-you/healthy-living-resources/diet-nutrition/basic-meal-planning
- Richard D. Feinman, Wendy K. Pogozelski, Arne Astrup, Richard K. Bernstein, Eugene J. Fine, Eric C. Westman, Anthony Accurso, Lynda Frassetto, Barbara A. Gower, Samy I. McFarlane, Jí¶rgen Vesti Nielsen, Thure Krarup, Laura Saslow, Karl S. Roth, Mary C. Vernon, Jeff S. Volek, Gilbert B. Wilshire, Annika Dahlqvist, Ralf Sundberg, Ann Childers, Katharine Morrison, Anssi H. Manninen, Hussain M. Dashti, Richard J. Wood, Jay Wortman, Nicolai Worm,
Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base,
Nutrition,
Volume 31, Issue 1,
2015,
Pages 1-13,
Copyright ©2018 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.