I am not one for popular remedies for health issues. I don’t believe in “cleanses” and I don’t “eat clean” – or do I? If not eating any dairy is “clean” then I eat “dirty” because I use cream in my coffee, but if not eating gluten or grains is “clean”, then my eating is pristine.
The problem with popular beliefs around food and eating and word-of-mouth remedies is there is no standardized means to define them or evaluate their effectiveness.
Folk Remedies
Folk remedies, on the other hand, are in a different category. These practices, on which many nutraceuticals and even pharmaceuticals are based have GRAS standing (“Generally Recognized As Safe”) and have been used by cultures around the world for hundreds, if not thousands of years.
Here’s are two examples of folk-remedies in this category;
Swallow’s Nest
The Chinese have made soup out of the nest of a particular swallow which builds its home on high cliffs. This “bird’s nest soup” is highly prized and very expensive to make, but considered to have restorative properties for those with breathing difficulties. As it turns out, this particular swallow’s nest is high in theophilline, a compound that has come to be used in Western medicine as therapy for respiratory diseases such as chronic obstructive pulmonary disease (COPD) and asthma. Bird’s nest from this swallow has a GRAS standing and can legally be purchased in traditional Chinese medicine stores. One can take medication or food containing the same active substance, and in both cases one’s symptoms improve.
Bitter Melon
Bitter melon or bitter gourd / karela is widely grown in Asia, Africa and the Caribbean – both for food (prized for its bitter taste) and for its medicinal properties. In both Ayurveda, the traditional medicine (Hindu) of India and in Traditional Chinese Medicine (TCM) different parts of the bitter melon plant are brewed as a beverage and taken as a treatment for Diabetes. As it turns out, bitter melon, which has GRAS standing, contains polypeptide-p which is an insulin analogue.
Apple Cider Vinegar
I’ve been hearing about the use of apple cider vinegar (ACV) since I first started reading about low carb high fat diets in early 2015, from Dr. Jason Fung, a nephrologist (kidney specialist) from Toronto. He recommended that 1 Tbsp. of unpasteurized ACV be taken in a glass of water prior to meals and that it be add it to broths, soups and marinades. He’d said that it inactivates the production of digestive enzymes and slows down the rate of digestion, stabilizing blood sugar levels. Since the recommendation to use ACV at the time did not come with any scientific evidence, I summarily dismissed the idea of using it.
Persistently High Fasting Blood Glucose
For those who have been following my own progress following a Low Carb High Fat style of eating over the past 6 months (posted on the tab “A Dietitian’s Journey”) you know that despite losing weight, significantly lowering both my triglycerides and LDL cholesterol and my overall blood sugar levels coming down significantly, I had two ongoing problems;
(1) my morning fasting blood glucose (FBG) remained high, and
(2) my blood glucose would only drop into the 5-point-something mmol/ L range (~94 mg/dl) or to the 4-point-something mmol/ L range (76 mg/dl) range after an entire day of intermittent fasting.
Since there are physiological risks associated with high blood glucose, I was very motivated to find out why they were high in the morning and to do something about them.
I decided to keep detailed food records for 3 weeks to see if there was a patter, and ruled out diet.
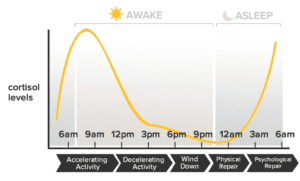
Then, I decided to take my blood sugar several times each night, from midnight until 8 am, over several days, to see when it rose. As it turned out, it would drop nicely after supper (as it would after eating at any other time of the day), to 7-point-something mmol/l (~130 mg/dl) after an hour or so, and then to 6-point-something mmol/L (121 mg/dl) around midnight, and then it would gradually begin to rise from ~2 am, reaching its highest point around 8 am, following the circadian rhythm of cortisol.
Since it seemed that my high morning blood sugar was due to cortisol rising after went to bed until 8 am, and since cortisol can be affected by many things including stress, I took up going for a walk after supper. It did help! My morning blood sugars were in the mid-6-point-something mmol/L (~117 mg/dl), which was a far-cry from the 8.0 mmol/L (144 mg/dl) level it had been!
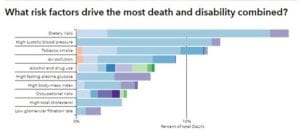
The evening walks, however, were short lived due to a shift in the winds and the raging forest fires in and around the Lower Mainland which caused the skies to fill with Fine Particulate Matter, know as PM2.5 (as the are 2.5 micrometers or less, in size). Since these can enter the lungs and the blood stream resulting in ill-effects, my walks stopped. In fact, if I did have to go out, it was with a vented N-95 mask. The smoke briefly cleared being replaced by stifling heat in the mid- to high-30 Celsius (100 F) for 10 days, followed by more smoke, so I began to look for something- anything that might lower my morning blood sugars, which at this point were hovering in the 7.6 mmol/L mmol/L (137 mg/dl) range!
At first I tried doing a short workout on my Nordic-track or using my “step” before bed, but it didn’t do much for my blood sugars and made me far too awake to fall asleep.
Having some unpasteurized, unfiltered ACV in the house, I decided to try it. It tasted terrible!! I tried adding it to water and it was still awful! I couldn’t bring myself to drink it!!
From Masking the Taste to Food as Medicine

A few years ago, in an effort to drink more water each day, I began drinking Club Soda / Selzer and then purchased a Sodastream machine, to carbonate my own (filtered) water.
I usually drink it plain, but have been known to put a twist of fresh lemon or lime in it.

I tried adding 1 Tbsp of unpasteurized ACV to 1 litre (quart) of carbonated water but I still couldn’t drink it! All I tasted was sour!
Needing to mask the taste, I decided to grate a bit of fresh ginger root into it and “ACV Gingeraid” was born!
The first time, I drank a litre (~ quart) of “ACV Gingeraid” mid-morning, and my blood sugar dropped from 7.3 mmol/L (132 mg/dl) to 6.6 mmol/L (119 mg/dl) in an hour. I thought to myself that maybe it would have dropped the same amount if I had done nothing.

I hadn’t had anything to eat or drink (except a coffee with only cream in the morning) but presumably under the effect of cortisol and my body’s own making of glucose from fat stores, my blood sugar continued to rise from 6.6 mmol/L (119 mg/dl) at 5:30 AM, to 7.7 mmol/L (139 mg/dl) just before 10 AM.
That was just too high – and I hadn’t eaten!
So, I made and drank a second bottle of ACV Ginger-aid and in 1.5 hrs, my blood sugar had dropped to 6.3 mmol/L (114 mg/dl). Then by 4:00 PM, and drinking no additional ACV Ginger-aid, it was 4.8 mmol/L (86 mg/dl).
I would previously only get to those kinds of numbers just before dinner, when I was on an intermittent fast day. This was 2-2.5 hours earlier.

That couldn’t be, I thought…
Several days in a row, the same thing would happen, with only slightly different numbers, some of them lower.
My blood sugar would be around 7.3 mmol/L (137 mg/dl) 2 hours after dinner and I would drink most of a bottle of ACV Ginger-aid before bed, and in the morning my FBG would be in the 6’s mmol/L (~119 mg/dl). Could it be because of the drink?

One day, quite by chance, I had some fresh turmeric root in the house (because I use it in cooking and because I like the taste). As well, is a potent antioxidant and the curcumin (the active compound in turmeric) has been demonstrated to have anti-carcinogenic properties).
I decided to add a little bit of grated turmeric root because I thought the turmeric would taste good with the ginger (it did!).
I also added a bit of freshly ground black pepper to the Turmeric-ACV Ginger-aid, because I had read that black pepper makes the curcumin in the fresh turmeric root 2000 times more bio-available.

The drink tasted delicious!
But what happened to my blood sugars was quite surprising.
It became evident that for me, using “food as medicine” has had some very impressive results!
Just 3 days earlier, I was impressed because by 4:00 PM my blood glucose was 4.8 mmol/L (86 mg/dl) – which was a good 2.5 hours earlier than usual.
Since adding the turmeric to the ACV Ginger-aid, I was getting numbers in the mid-4 mmol/L (i.e. 4.6 mmol/L / 84 mg/dl) by 2:30 in the afternoon!
By drinking the Turmeric-ACV Ginger-aid before bed, my morning FBG is consistently in the low 6’s mmol/L (~110 mg/dl) and on a few occasions, ”ve been getting numbers in the high-5s mmol/L (103 mg/dl). I was considering Metformin to get these kinds of results!
This is by consuming ordinary food found in my kitchen!
I continue to eat LCHF and I usually intermittent fast breakfast, as I’ve never been much of a “breakfast person”. I occasionally don’t eat until mid-day as that is when I usually first feel hungry.
My blood sugars are the best they’ve been since I started measuring them.
Now, 2 hours after meals my blood sugar is usually in the low 6’s mmol/l (~110 mg/dl) and the ONLY change has been adding this beverage before bed and occasionally one plain ACV Ginger-aid through the day.
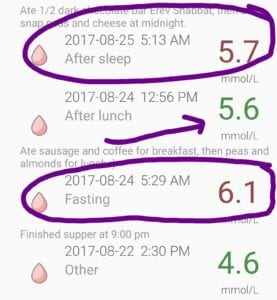
Just to be a ‘good scientist’, last night I deliberately ate 1/2 a dark chocolate bar (72% cocoa) and drank 3/4 of a bottle of plain AVC Ginger-aid (no turmeric) and tested my blood glucose this morning. It was 6.6 mmol/L (119 mg/dl). That’s crazy! I was expecting 10 or 11 mmol/L. That’s what it used to be just a few weeks ago, when I’d eat a little bit of dark chocolate!
NOTE: I wanted to see what would happen if I ate the same way but discontinued the beverage. My blood sugar went up to 8.8 mmol/L the first morning after not having any the previous day and was 8.6 mmol/L the following morning. The third day, I drank only one bottle in the afternoon and on at night before bed and the following morning, my fbg was 7.2 mmol/L (still way too high, but much lower). I anticipate it will continue to drop as I have 2-3 bottles of the mixture per day.
Even thought I am NOT exercising (first because of the smokey conditions outside and because I fell back into old “bad-habits” of getting up early and working at my desk with my coffee), my blood glucose is what I would have anticipated would have occurred if I had taken Metformin.
Keep in mind, I am “a sample-set of one”. There’s no saying that others will have the same, or even similar results. In addition, I do NOT encourage people to make any changes in the amount of medication that a doctor prescribed without being told by that doctor. This drink is NOT a substitute for medication that has been prescribed! That being said, for those who are not taking medication but have persistently high blood sugar readings does it not make good sense to consider trying such food as medicine?
NOTE: I decided to find out if there was any scientific evidence for the anti-glycemic properties of ACV and did find a 2015 study, suggesting that it increases insulin-stimulated glucose uptake in those with Type 2 Diabetes (T2D), which I have. I then decided to look and see if ginger had anti-glycemic properties and found a 2015 study that reported that ginger significantly reduced FBG as well as HbA1c, along with Apo B, Apo B/Apo A-I, MDA and increased the level of Apo A-I in T2D patients. Naturally, I looked to see if turmeric was known to have anti-glycemic properties and sure enough, it did! I found a 2013 publication that indicated it is well-known that turmeric has a stimulatory action on pancreatic β-cells, and that this may be the mechanism by which it lowers blood sugar in those with T2D. Whether these substances used together have a far greater effect on blood sugar than any of them used separately would certainly make for an interesting study!
WARNING: Given the possibility of these ordinary foods resulting in a dramatic drop in blood sugar, if you have Type 2 Diabetes or pre-diabetes, first discuss incorporating these foods into your diet with your doctor. As well, be sure to monitor your high blood sugar often if you drink these.
ACV Gingeraid Recipe
Click on the link under “Recipes” for ACV Gingeraid with Variations – food as medicine. Enjoy!
you can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
References
Mitrou P, Petsiou E, Papakonstantinou E, et al. Vinegar Consumption Increases Insulin-Stimulated Glucose Uptake by the Forearm Muscle in Humans with Type 2 Diabetes. Journal of Diabetes Research. 2015;2015:175204. doi:10.1155/2015/175204.
Khandouzi N, Shidfar F, Rajab A, Rahideh T, Hosseini P, Mir Taheri M. The Effects of Ginger on Fasting Blood Sugar, Hemoglobin A1c, Apolipoprotein B, Apolipoprotein A-I and Malondialdehyde in Type 2 Diabetic Patients. Iranian Journal of Pharmaceutical Research”¯: IJPR. 2015;14(1):131-140.
Zhang D, Fu M, Gao S-H, Liu J-L. Curcumin and Diabetes: A Systematic Review. Evidence-based Complementary and Alternative Medicine”¯: eCAM. 2013;2013:636053. doi:10.1155/2013/636053.
![]() https://twitter.com/joykiddieRD
https://twitter.com/joykiddieRD
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
Note: Everyone's results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody's nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
Copyright ©2017 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.


 The chia seeds are ground a little bit with the previously ground flax seed, and then the two ground seeds are placed in a small bowl.
The chia seeds are ground a little bit with the previously ground flax seed, and then the two ground seeds are placed in a small bowl.




 Last night, for the first time since I was diagnosed with Type 2 Diabetes (T2D) ten years ago, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl).
Last night, for the first time since I was diagnosed with Type 2 Diabetes (T2D) ten years ago, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl). My cells aren’t yet ‘healed’. They and my liver are still insulin resistant which is evidenced by the fact that even though I haven’t eaten anything since dinner last night, my blood glucose is high.
My cells aren’t yet ‘healed’. They and my liver are still insulin resistant which is evidenced by the fact that even though I haven’t eaten anything since dinner last night, my blood glucose is high.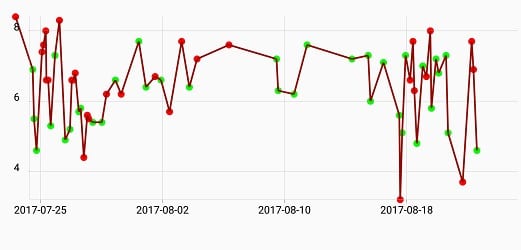
 Monday, my blood glucose was 3.7 mmol/L (67 mg/dl) at 4:00 PM and yes, I ate something immediately.
Monday, my blood glucose was 3.7 mmol/L (67 mg/dl) at 4:00 PM and yes, I ate something immediately.









 ). As with the eighteen-hour fast, one can have unsweetened coffee or tea with a drop of cream, club soda (seltzer) with a twist of lime or lemon, or “bone broth”. “Bone broth” can be made from any kind of meat, fish or poultry bones, but for me, when I think of “bone broth”, I think of a wonderful, rich broth made from beef marrow bones, that is gently simmered overnight on the stove, ready to be sipped as desired, on a fast day.
). As with the eighteen-hour fast, one can have unsweetened coffee or tea with a drop of cream, club soda (seltzer) with a twist of lime or lemon, or “bone broth”. “Bone broth” can be made from any kind of meat, fish or poultry bones, but for me, when I think of “bone broth”, I think of a wonderful, rich broth made from beef marrow bones, that is gently simmered overnight on the stove, ready to be sipped as desired, on a fast day.

 For the last 2 weeks, the Lower Mainland has been covered in smoke due to hundreds of wildfires in the area. The very poor air quality had made going for a walk impossible.
For the last 2 weeks, the Lower Mainland has been covered in smoke due to hundreds of wildfires in the area. The very poor air quality had made going for a walk impossible.


 Even wearing an N95 mask outside which is designed to filter out the small smoke particles, I have found my breathing very laboured.
Even wearing an N95 mask outside which is designed to filter out the small smoke particles, I have found my breathing very laboured.

 Taking the blood pressure medication is a temporary measure that I decided on in order to offer some protection against heart attack, stroke and kidney damage until I lose more weight, and my blood pressure stays down on its own.
Taking the blood pressure medication is a temporary measure that I decided on in order to offer some protection against heart attack, stroke and kidney damage until I lose more weight, and my blood pressure stays down on its own.








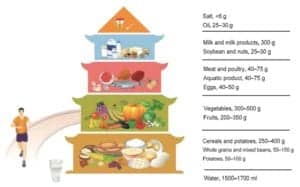
 The Chinese Dietary Guidelines, known as the ‘Food Guide Pagoda’ was first published in 1989 and revised in 1997. The 2007 revision was developed in conjunction with a committee from the Chinese Nutrition Society, in association with the Ministry of Health. A new revision came out in 2016.
The Chinese Dietary Guidelines, known as the ‘Food Guide Pagoda’ was first published in 1989 and revised in 1997. The 2007 revision was developed in conjunction with a committee from the Chinese Nutrition Society, in association with the Ministry of Health. A new revision came out in 2016.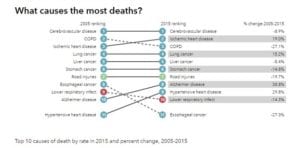 In 2015, heart disease overtook Chronic Obstructive Pulmonary Disease (COPD) as the second leading cause of death, followed by stroke.
In 2015, heart disease overtook Chronic Obstructive Pulmonary Disease (COPD) as the second leading cause of death, followed by stroke. In 2015 as in 2005, stroke was the leading cause of death, followed by heart disease.
In 2015 as in 2005, stroke was the leading cause of death, followed by heart disease.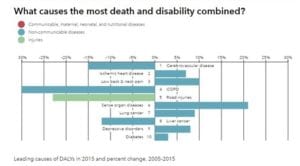 In 2015, stroke was leading cause of death in China, followed by heart disease.
In 2015, stroke was leading cause of death in China, followed by heart disease.