
An analysis was published last week in the British Medical Journal which raised several important concerns about the World Health Organization (WHO)’s draft guidelines on fatty acids; including saturated fat.
The international group of 16 nutrition experts who wrote the paper are concerned as “many governments consider the WHO dietary guidelines to be state of the art evidence, translating them into regional and national dietary guidelines” [1].
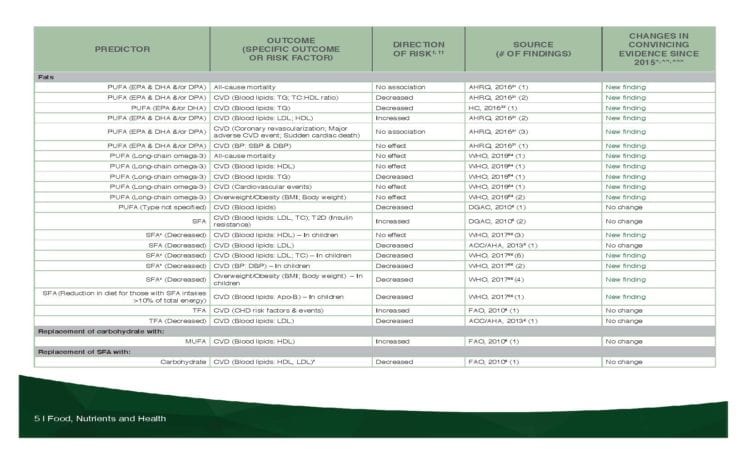
In fact, this is exactly the case in Canada. The new Canada Food Guide that was just released on January 22, 2019 relied extensively on the WHO’s 2017 Guidelines for it’s policy regarding decreasing dietary saturated fatty acids (SFA), as indicated by the table below from pg. 5 of Health Canada’s Interim Evidence Update 2018 [2].
“These guidelines have potential health implications for billions of people, so the consistency of the science behind such recommendations and the validity of the conclusions are crucial”.
The authors state that the WHO, in their draft guidelines released in May 2018 “excluded some important aspects and studies” concerning evidence linking saturated fat intake and cardiovascular (CVD) risk.
“They [WHO] recommend reducing intake of total saturated fatty acids to less than 10% of total energy consumption and replacing with polyunsaturated fat and monounsaturated fat to reduce incidence of cardiovascular disease and related mortality. But this fails to take into account considerable evidence that the health effects vary for different saturated fatty acids and that the composition of the food in which they are found is crucially important.”[1]
The authors point out that the composition of the food in which the fatty acid is found has a substantial effect on lipid digestion, absorption, as well as the amount of emulsified fat that is found in the blood after a meal (postprandial lipemia), which “is an independent risk factor for cardiovascular disease.”[1]
The authors point out that recently there have been several meta-analyses of observational studies and randomized controlled trials (RCTs) that found that total saturated fat is NOT associated with coronary heart disease, cardiovascular disease, and all cause mortality (i.e. deaths). In addition they report that a Cochrane analysis found no significant association between reducing saturated fatty acids and total mortality, cardiovascular disease deaths, fatal and non-fatal myocardial infarction (MIs), stroke, coronary heart disease events, and coronary heart disease deaths.
Continued Reliance on Surrogate Endpoints
The authors note that the WHO draft guidelines continue, as they have in the past, to (1) rely heavily on “surrogate endpoints” of the effect of dietary saturated fat intake on the level of lipid and lipoproteins in the blood — and (2) ignores the food source of the saturated fat.
They raise three key points;
1. Not all saturated fatty acids are equal; the amount and even the direction of the effects (raises or lowers) both surrogate and long term endpoints vary, depending on which fatty acid is involved.
2. Influence of the food source that the fatty acid is found in; the authors note that it has still not been determined whether any changes in blood lipoproteins translates into a lowering of cardiovascular risk and death, regardless of food source.
“Most trials included in the meta-analysis did not investigate whole food sources of saturated fat.”[1]
That is, the studies that WHO considered compared the effect of diets supplemented with fats rich in saturated fatty acids — not the effect of saturated fats in a specific food matrix.
One example of saturated fat in a whole food matrix cited in the paper is one of eggs; where there is “no association with coronary heart disease, and there is a reduced risk of stroke, and that randomized control trial data show that two eggs a day has beneficial effects on cardiovascular disease biomarkers“. (table 1, [1]).
3. Using LDL cholesterol concentration as a marker for cardiovascular disease risk. As I’ve written about in several previous articles, the authors note that the degree to which LDL particles are atherosclerotic is determined by, among other things, their size.
“Small and medium LDL particles show the strongest association with risk of cardiovascular disease, whereas large particles show no association.” [1]
in fact, the authors point out as I did in a recent article about red meat and white meat “raising cholesterol”, that a rise in serum LDL cholesterol concentration from total saturated fat consumption has been linked to a parallel increase in particle size “so it might not translate into an
increased risk of cardiovascular disease.”[1]
Excluding Observational Studies and Prospective Cohort Studies
The authors point out that the WHO draft guidelines exclude two types of studies from consideration; observational studies and prospective cohort studies because they argue that the quality of the evidence is lower than from
analyses of RCTs, and that it was not possible to assess the potential differential effects of replacing saturated fatty acids with different nutrients.
The problem with this is that (1) observational studies enable assessing the association between saturated fat and cardiovascular disease rather than simply looking at the association between surrogate endpoints” (i.e. saturated fat and LDL-c) and (2) observational studies enable examining of the actual foods that people eat, rather than just individual nutrients, as
“Longstanding evidence indicates that the food matrix is more important than its fatty acid content for predicting the effect of a food on risk of coronary heart disease.”
The authors concluded;
“A recommendation to reduce intake of total saturated fat
without considering specific fatty acids and food sources is not
evidence based; will distract from other more effective food-
based recommendations; and might cause a reduction in the
intake of nutrient dense foods that decrease the risk of
cardiovascular disease, type 2 diabetes, other serious
non-communicable diseases, malnutrition, and deficiency
diseases and could further increase vulnerability to nutrient
deficiencies in groups already at risk.
Final thoughts
This analysis adds a critical academic “voice” to the concern of limited saturated fat intake which may translate a reduction in the intake of nutrient-dense whole foods.
In fact, this was precisely the concern that I raised in my recent article about the Canada Food Guide “Snapshot” which came out at the end of June and which linked an image of ultra-processed foods with the message “limit foods high in sodium, sugars or saturated fat”. After all, meat is high in saturated fat and cheese is high in saturated fat and sodium, but are these really the types of whole, real foods that Canadians should be advised to limit?
More Info?
If you would like more information about choosing whole, real food and limiting ultra-processed foods, I can help.
You can learn more about my services under the Services tab or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchf-rd/
Instagram: https://www.instagram.com/lchf_rd
Fipboard: http://flip.it/ynX-aq
Copyright ©2019 The Low Carb Healthy Fat Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
- Astrup A, Bertram HCS, Bonjour J-P et al, WHO draft guidelines on dietary saturated and trans fatty acids: time for a new approach? BMJ 2019; 366: l4137 doi: 10.1136/bmj.l4137
- Health Canada. Food, Nutrients and Health: Interim Evidence Update 2018. Ottawa: Health Canada; 2019.
Share to Flipboard:
