INTRODUCTION: In response to numerous inquiries from individuals, healthcare professionals and the general public, Diabetes Australia has just released a new Position Statement titled Low Carbohydrate Eating for People with Diabetes[1] said to be based on the latest evidence on the subject. Diabetes Australia is the national body responsible for making treatment and dietary recommendations for the 1.7 million people in that country living with Diabetes. The publication is designed to provide practical advice and information for people diagnosed with Diabetes who are considering adopting a low carbohydrate eating plan. Since I don’t provide dietary to support to those with Type 1 Diabetes (but defer instead to someone with CDE credentials), I have limited my discussion to recommendations pertaining only to Type 2 Diabetes.
Diabetes Australia defines low carbohydrate (“low carb”) eating patterns as those that restrict carbohydrate intake — especially processed and packaged foods and beverages including cakes, candies, chocolate, chips, ice cream and sugary drinks as well as breads, cereals, grains, potatoes, fruit and sugar. They elaborate that when people are limiting carbohydrates they eat a higher proportion of protein and fats such as those found in meat, chicken, eggs, oily fish, avocados, nuts, oils and butter and eat plenty of low carb vegetables, such as cauliflower and zucchini. In this publication, they specify that a low carbohydrate diet provides “less than 130g of carbohydrate daily/ less than 26% of total daily energy intake”[1].
“When it comes to low carb eating, there is no particular diet or standard approach.”
Diabetes Australia reinforces that the (Australian) “Dietary Guidelines provide general healthy eating advice and are a good starting point for people wanting to improve their eating habits”, but that
“there is no one-size-fits-all approach to living well with Diabetes. Everybody is different.”
The publication makes clear that Diabetes Australia “does not promote or encourage any single diet or eating plan or any particular ‘diabetes diet'” and that “every person with Diabetes needs a personalized approach and support to have the healthiest eating plan and this may change over their lifetime with Diabetes“. They mention that in recent years, low carb eating has gained popularity with the general population and has also gained interest for people with Diabetes as “an option to help lose weight and to assist in managing blood glucose levels” — because “low carb diets are relatively easy to follow”.
In formulating their Position Statement, the organization states that they rely on “strong scientific evidence before making specific health and nutrition recommendations for people with diabetes or those at risk” and that “evidence is usually based on the National Health and Medical Research Council (NHMRC) hierarchy of evidence”[2] whose components are; 1. The evidence base, in terms of the number of studies, level of evidence and quality of studies (risk of bias), 2. The consistency of the study results, 3. The potential clinical impact of the proposed recommendation, 4. The generalisability of the body of evidence to the target population for the guideline, and 5. The applicability of the body of evidence to the Australian healthcare context. This hierarchy of evidence is said to also need to take into account “the quality of the study and the likelihood that the results have been affected by bias during its conduct; the consistency of its findings to those from other studies; the clinical impact of its results; the generalisability of the results to the population for whom the guideline is intended; and the applicability of the results to the Australian (and/or local) health care setting”.
The position statement stresses that Diabetes Australia believes that
“People with Diabetes should make their own, informed choices about their Diabetes management (including eating plans) in consultation with their diabetes healthcare team”.
They recognize that “long-term studies can take years to be designed, conducted and published” and underscore that they will continue to review and update their advice in relation to low carb eating for people with Diabetes based on new evidence as it becomes available.
Key Points
[1] Based on two studies [3,4] the report states that “recent evidence has shown that in the short term (up to 6 months), lower carb eating can help with the management of Type 2 Diabetes but that this benefit is no longer evident after 12 months”.
NOTE:
(a) Both of the studies quoted [3,4] were not low carb studies but moderate carb studies of <45% (225g carbohydrate) per day. Low carbohydrate diets as defined by this paper are diets which provide “less than 130 g of carbohydrate daily/ less than 26% of total daily energy intake” and the paper defines a moderate carbohydrate diet as one that provides “130g—225g of carbohydrate daily/ 26%—45% of total daily energy intake”. The two quoted studies provided dietary intake of carbohydrate that were moderate carbohydrate. Neither was a low carbohydrate study.
(b) Interestingly, despite neither study being a low carb study, one of the quoted studies [3] found “greater weight loss at 12 months on moderate carb diets than high carb diets” — which contradicts that there was no benefit after 6 months. Even a moderate-high carb diet had benefit beyond 6 months when compared with a high carb diet!
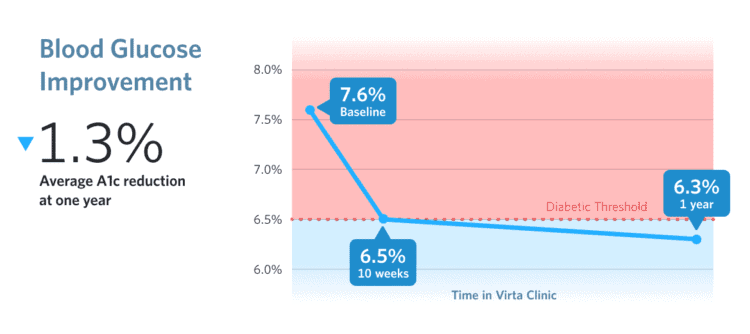
(c) In addition, the position statement did not consider the recent publication of the 1-year study results from Virta Health [5] outlined in detail in this article.
[2] In addition to promoting weight-loss, reducing carbohydrate intake can provide health benefits that include lowered average blood glucose levels and reduced risk of heart disease such as raised cholesterol and raised blood pressure and that some benefits can be achieved independent of the amount of weight-loss achieved.
[3] All people with Diabetes who wish to follow a low carb diet should
do so in consultation with their Diabetes healthcare team.
[4] People with Diabetes who begin low carb eating should monitor their
blood glucose levels and, if necessary, talk to their doctor about the need to
adjust their Diabetes medication to reduce the risk of hypoglycaemia (low
blood glucose).
[5] People with Diabetes considering low carb eating are encouraged to seek
personalized advice from an Dietitian experienced in Diabetes management as there are some practical considerations that need to be taken into account to ensure the eating plan is safe and enjoyable, provides adequate nutrition for general health, is culturally appropriate and fits into the person’s lifestyle.
[6] People with Diabetes considering low carb eating should be aware of
possible side effects (such as tiredness, headaches and nausea) and seek
advice from their health care team if concerned.
[NOTE: I’ve never heard or read about people experiencing nausea following low carb eating, and even at the beginning of following a low carb style of eating symptoms such as tiredness and headache are easily addressed with adequate fluid and electrolytes.]
[7] Low carb eating may not be safe and is not recommended for children,
pregnant or breastfeeding women, people at risk of malnutrition, people
with kidney or liver failure, or those with a history of disordered eating or some rare metabolic conditions.
[8] All people who choose to follow a low carb eating plan should be encouraged to eat foods proven to be beneficial to good health, including whole fruit and vegetables, whole-grains*, dairy foods, nuts, legumes*, seafood, fresh meat and eggs.
[*NOTE: Depending on the amount of insulin resistance and hyperinsulinemia that someone with Type 2 Diabetes has they may or may not be able to maintain glycemic (blood sugar) control eating whole-grains and legumes. In their minimally processed forms, these may be able to be re-introduced in small quantities on an individual basis after reversal of Type 2 Diabetes symptoms and lower circulating insulin levels / reduced insulin resistance.]
[9] All people should be encouraged to limit their intake of foods that are high in energy*, carbohydrate or salt*, including processed foods such as sugary drinks, chips, cakes, biscuits, pastries and candies.
[NOTE: Unfortunately, foods that are ‘high in energy’ or ‘high in salt’ are inadequately defined in this publication. “High in energy” would be better framed as “low nutrient density foods” — which are foods high in energy relative to the amount of nutrients they contain. Cheese for example may be energy-dense per 100 g but is also very nutrient-dense. What does “high in salt” means — high in salt for whom?
Perhaps you have questions as to how I could help you get started on eating low carb to lower your blood sugars, reverse symptoms of Type 2 Diabetes, reduce your risk of heart disease including raised cholesterol and blood pressure and lose weight?
Since I provide services both in-person in my Coquitlam (British Columbia) office as well as via Distance Consultation (Skype or phone), I am available to help.
Please send me a note using the Contact Me form above and I will reply as soon as I am able.
To our good health!
Joy
you can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
Copyright ©2018 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
- Diabetes Australia, Low Carbohydrate Eating for People with Diabetes – Position Statement, August 2018, https://static.diabetesaustralia.com.au/s/fileassets/diabetes-australia/ee67e929-5ffc-411f-b286-1ca69e181d1a.pdf
- National Health and Medical Research Council (2009), NHMRC additional levels of evidence and grades for recommendations for developers of guidelines, https://www.nhmrc.gov.au/_files_nhmrc/file/guidelines/developers/nhmrc_levels_grades_evidence_120423.pdf
- Sainsbury E et al. Effect of dietary carbohydrate restriction
on glycaemic control in adults with diabetes: a systematic
review and meta-analysis. Diabetes Research and Clinical
Practice, 2018; 139: 239-252. - Snorgaard O et al. Systematic review and meta-analysis
of dietary carbohydrate restriction in patients with type 2
diabetes. BMJ Open Diabetes Research & Care, 2017;
5(1). - Hallberg, S.J., McKenzie, A.L., Williams, P.T. et al. Diabetes Ther (2018). Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. https://doi.org/10.1007/s13300-018-0373-9



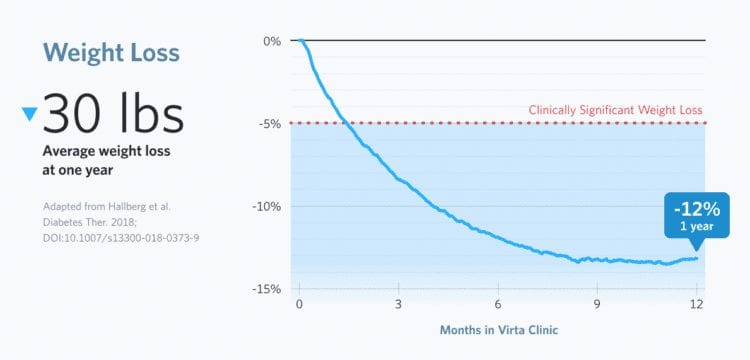
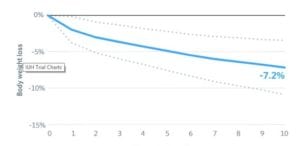 Mean body mass reduction was 7.2% from a baseline average of 117 kg (257.4 pounds) ±26 kg / 57 lbs.
Mean body mass reduction was 7.2% from a baseline average of 117 kg (257.4 pounds) ±26 kg / 57 lbs.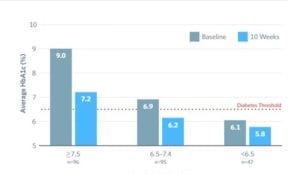 At 6 months, HbA1C was reduced to 6.1% ±0.7% from 7.5% ±1.3% in a sample of 108 participants who elected to test HbA1c at 6 months.
At 6 months, HbA1C was reduced to 6.1% ±0.7% from 7.5% ±1.3% in a sample of 108 participants who elected to test HbA1c at 6 months.