

INTRODUCTION: A low carbohydrate, high fat diet is not new, in fact eating this way was the standard recommendation for treating Diabetes prior to the discovery of insulin.
More than 150 years ago, the first weight-loss diet book, written by William Banting, ironically a distant relative of Sir Frederick Banting, the co-discoverer of insulin focused on the limiting the intake of carbohydrates, especially those of a starchy or sugary nature. The book was titled Letter on Corpulence — Addressed to the Public (1864) and summarized the advice of the author’s physician, Dr. William Harvey that had enabled Banting to shed his ‘portly stature’.
In clinical practice, a ketogenic diet (very low carbohydrate, high fat, adequate protein) was successfully used in the Mayo Clinic nearly 100 years ago by Dr. R. Wilder as a treatment for epilepsy and continues to be used at Johns Hopkins University and other centers for this purpose.
In 1963, Dr. Robert Atkins in his own search for a weight loss plan came across an article in the Journal of the American Medical Association titled A New Concept in the Treatment of Obesity [1]. After he successfully lost weight by following its recommendations, he decided to enroll 20 overweight business executives in a 20 week trial. All lost weight and follow up records indicated that they continued to keep it off for at least a year. After establishing his medical practice in New York City, Dr. Atkins made some adjustments to the plan and incorporated it into his practice, helping his own patients successfully lose weight. In 1972, Atkins published his book Diet Revolution which was immediately successful but very controversial. Criticism of Atkins and his diet continues to this day.
Anecdotal evidence which relies on personal testimony is fine as encouragement (hence my blog A Dietitian’s Journey) and the clinical experience of physicians such as Dr. Jason Fung, a nephrologist from Toronto is excellent, but clinical use of a low carbohydrate diet to target the reversal of symptoms of Type 2 Diabetes requires scientific studies.
Enter Phinney and Volek.
Stephen Phinney, MD, PhD is a medical doctor and scientist with 40 years experience and is Professor of Medicine Emeritus at University of California, Davis. Dr. Phinney is an internationally recognized expert on obesity, carbohydrate-restricted diets, diet and performance and essential fatty acid metabolism and has held clinical faculty appointments at MIT, the Universities of Vermont, Minnesota and California at Davis. He has designed, conducted and published data from more than 20 clinical protocols involving diets, exercise, oxidative stress and inflammation and his design of clinical nutrition trials has led to more than 87 peer-reviewed papers and book chapters on clinical nutrition and biochemistry.
Jeff Volek, PhD, RD is a Registered Dietitian with a Doctorate degree and is professor in the Department of Human Sciences at The Ohio State University. Dr. Volek’s work has contributed to the existing science of ketones and ketogenic diets, their use as a therapeutic tool to manage insulin resistance. For the past 20 years, Dr. Volek has researched how humans adapt to diets restricted in carbohydrates, with a focus on both the clinical and performance application of nutritional ketosis. He has published more than 300 peer-reviewed scientific manuscripts and five books.
In 2011, Phinney and Volek published their fully referenced expert guide titled The Art and Science of Low Carbohydrate Living documenting the clinical benefits of carbohydrate restriction and its practicality as both a sustainable and enjoyable lifestyle. While primarily a book directed towards healthcare professionals and those with a science background, it provides ample scientific evidence behind the use of a low carbohydrate diet to target the reversal of symptoms of Type 2 Diabetes.
In the January-June issue of JMIR Diabetes, Phinney and Volek along with a host of other physicians, Registered Dietitians and nurses published initial 10 week results of a nonrandomized, parallel arm, outpatient intervention using a very low carb diet which induced nutritional ketosis*. Each participant was provided with intensive nutrition and behavioral counseling, digital coaching and education platform and physician-guided medication management.
Nutritional ketosis was defined as a dietary regimen resulting in serum ketone levels of β-hydroxybutyrate between 0.5 and 3.0 mmol·L−1
There were 238 participants in the intervention, all participants had a diagnosis of Type 2 Diabetes (T2D), mean age was 54 years old (with participants ranging in age from 46 – 62 years). The majority were women 67% with 33% men. Average weight was 257 pounds (117 kg) with participants ranging from 200 pounds to 314 pounds (117±26 kg). Average Body Mass Index (BMI) was 41 kg·m-2 (class III obesity) ±9 kg·m-2. Average HbA1c was 7.6% ±1.5%. The majority of participants (89%) were taking at least 1 glycemic control medication.
Each participant received an Individualized Meal Plan for nutritional ketosis, behavioral and social support, biomarker tracking tools, and ongoing care from a health coach with medication management by a physician.
Subjects typically required <30 g·day−1 total dietary carbohydrates. Daily protein intake was targeted to a level of 1.5 g·kg−1 based on ideal body weight and participants were coached to incorporate dietary fats until they were no longer hungry. Other aspects of the diet were individually tailored to ensure safety, effectiveness and satisfaction, including consumption of 3-5 servings of non-starchy vegetables and enough mineral and fluid intake. The blood ketone level of β-hydroxybutyrate was monitored, using a portable, handheld device.
Ten Week Outcomes
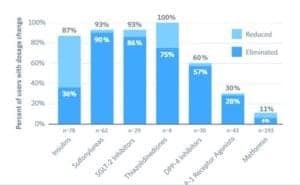
Medication Use
At baseline, 89% of participants were taking at least one medication for Diabetes.
At 10 weeks almost 57% had one or more Diabetes medications reduced or eliminated.
64% of insulin, sulfonylurea, SGLT-2 inhibitor, DPP-4 inhibitor and thiazolidinedione prescriptions were eliminated in 10 weeks.
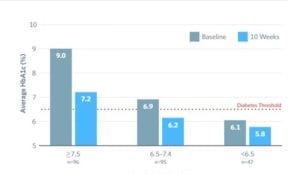
Glycosylated Hemoglobin (HbA1C)
At baseline, the average HbA1c level was 7.6% ±1.5%, with less than 20% having a HbA1c level of <6.5% (with medication usage).
After 10 weeks, HbA1c level was reduced by 1.0% and the percentage of individuals with an HbA1c level of <6.5% increased to more than 56%.
Note: 48% achieved this level while taking only Metformin (n=86) or no Diabetes medications (n=39). That is, >15% achieved this level by diet alone.
Weight Loss
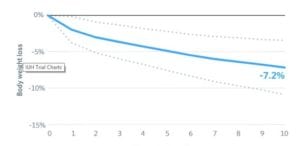 Mean body mass reduction was 7.2% from a baseline average of 117 kg (257.4 pounds) ±26 kg / 57 lbs.
Mean body mass reduction was 7.2% from a baseline average of 117 kg (257.4 pounds) ±26 kg / 57 lbs.
Six month outcomes
After 6 months, 89% of participants were still enrolled in the study. Results indicate that nutritional ketosis was quite effective in improving blood sugar control and weight loss in adults with Type 2 Diabetes, while significantly decreasing medication use.
Glycosylated hemoglobin (HbA1C)
 At 6 months, HbA1C was reduced to 6.1% ±0.7% from 7.5% ±1.3% in a sample of 108 participants who elected to test HbA1c at 6 months.
At 6 months, HbA1C was reduced to 6.1% ±0.7% from 7.5% ±1.3% in a sample of 108 participants who elected to test HbA1c at 6 months.
Twenty-two of the 108 started with a HbA1c <6.5%, and at 6 months, 76% reduced their HbA1c below the threshold for diabetes diagnosis (6.5%).
Weight Loss
Patients lost 11.5% (±8.8%) of their body weight with 81% having attained a clinically signiï¬cant weight loss (more than 5% of their body weight).
Medication Reduction
Most medication eliminations were maintained through 6 months along with reduced HbA1c and weight.
Participants also experienced a 20% reduction in triglycerides with an average value at follow-up in the healthy range below 1.69 mmol/L (150 mg/dL) [3].
Discussion
Improvements in blood sugar control in adults with Type 2 Diabetes (T2D) have been associated with weight loss of greater than 5% [4], which is why a weight loss component is part of many treatment plans.
As noted by the researchers, it is often assumed that it is the weight loss that leads to the improvements in blood sugar control, but it is possible that improvements in blood sugar control occur simultaneously with- or before signiï¬cant weight loss is achieved.
In their 10-week outcomes, weight and HbA1c reduction seemed to occur simultaneously, but the researchers noted that there were signiï¬cant reductions in HbA1c occurring even before the full life cycle of red blood cells (approximately 100 days), in which HbA1C is measured.
The researchers referred to other research which demonstrated that improvements in blood sugar control occur prior to signiï¬cant weight loss [5]. In that study, patients with Type 2 Diabetes who consumed a very low carbohydrate (ketogenic) diet of 21g of carbohydrate per day had signiï¬cantly improved insulin sensitivity concurrent with signiï¬cantly lower plasma glucose and HbA1c, but had only a 5 lb (2kg) weight loss after two weeks ( 1.8%) [5]. This suggests that it is not only the weight loss that was resulting in better insulin sensitivity.
The researchers also referred to other studies which reported that early improvement in blood sugar control is also highlighted by how quickly insulin and some oral anti-diabetic medications must be reduced or eliminated when a very low carbohydrate diet is begun, with most reductions and eliminations occurring in the ï¬rst 3 weeks [5,6] when there is only a modest reduction in weight.
The researchers noted;
“this suggests that weight loss may not be the driver of improved blood sugar control, but may be a positive side effect that is achieved concurrently with a well-formulated, very low carbohydrate diet.”
Medical Involvement
People with Type 2 Diabetes who take medication to lower blood sugar require the involvement of their physician as they follow a low carb- or ketogenic diet, as an adjustment in medication is often needed soon after beginning, due to blood sugar levels coming down. I would consider it prudent that regular daily glucose monitoring take place for (a) fasting blood sugar, at least once (b) just before a meal, and at least once (c) 2 hrs after a meal and again (d) at bedtime.
For those taking medication to lower blood pressure, the involvement of one’s physician is also needed, as blood pressure often drops with– or soon after blood sugar levels come down. The doctor may need to adjust medication dosages several times before attempting to trial eliminating them.
If you are taking medications to lower blood sugar or blood pressure, please speak to your doctor before beginning to eat low carb.
For those with Type 2 Diabetes but not taking any medication to lower blood sugar, regular daily glucose monitoring is still necessary, with (a) daily fasting blood sugar and (b) at bedtime and a few times per week (c) just before a meal, and (d) 2 hrs after a meal. This is to be sure that blood sugar levels do not drop too low.
For those whose clinical condition requires use of a very low carbohydrate diet / use of nutritional ketosis, monitoring of ketone levels using urine sticks at first and then blood levels of β-hydroxybutyrate occurs is highly recommended to make sure that steady levels are maintained.
Note: It is not recommended for people with any health or medical conditions to seek to achieve the levels of nutritional ketosis described in the above study, with levels of β-hydroxybutyrate between 0.5 and 3.0 mmol·L−1 without regular medical supervision.
Some final thoughts…
As demonstrated by this intervention study, it is entirely possible for the symptoms of Type 2 Diabetes to go into remission by following a low-carbohydrate lifestyle. After 6 months, >75% of people had HbA1c that was no longer in the Diabetic range (6.5%). This does not mean, however that their Diabetes was “cured”. If those people revert back to eating a high carb intake, they will experience the return of high blood sugar, blood pressure and abnormal lipid profile.
For those wanting to manage and aim to achieve remission of Type 2 Diabetes symptoms, I recommend that people first speak with their doctor about following a low carbohydrate diet with the support of an Registered Dietitian who is experienced using a wide range of low carb diets.
Have questions?
Why not send me a note using the Contact Me form located on the tab above?
You can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
References
1. Gordon ES, Goldberg M, Chosy GJ. A New Concept in the Treatment of Obesity, JAMA. 1963;186(1):50—60. doi:10.1001/jama.1963.63710010013014
2. Volek JS, Phinney SD, The Art and Science of Low Carbohydrate Living: An Expert Guide, Beyond Obesity, 2011
3. McKenzie AL, Hallberg SJ, Creighton BC, Volk BM, Link TM, Abner MK, Glon RM, McCarter JP, Volek JS, Phinney SD
A Novel Intervention Including Individualized Nutritional Recommendations Reduces Hemoglobin A1c Level, Medication Use, and Weight in Type 2 Diabetes, JMIR Diabetes 2017;2(1):e5
URL: http://diabetes.jmir.org/2017/1/e5
DOI: 10.2196/diabetes.6981
4. Franz MJ, Boucher JL, Rutten-Ramos S, VanWormer JJ. Lifestyle Weight-Loss Intervention Outcomes in Overweight and Obese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Journal of the Academy of Nutrition and Dietetics. 2015;115(9). doi:10.1016/
5. Boden G, Sargrad K, Homko C, Mozzoli M, Stein PT. Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. 2005;142(6): 403-411.
6. Bistrian BR, Blackburn GL, Flatt JP, Sizer J, Scrimshaw NS, Sherman M. Nitrogen metabolism and insulin requirements in obese diabetic adults on a protein-sparing modiï¬ed fast. 1976;25(6):494-504.
Note: Everyone's results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody's nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
Copyright ©2017 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.