

What all low carb diets have in common is that they are low in carbohydrates and high in healthy fats, but they vary with respect to the amount of protein and fat. This is part 1 in a new series titled The Role of Protein in the Diet, and outlines the problem with current carbohydrate intake in terms of the recommended dietary requirements.
This article is based largely on a lecture given by Dr. Donald Layman, PhD – Professor Emeritus from the University of Illinois (Nutrition Forum, June 23, 2013, Vancouver, British Columbia, Canada)
Sometimes, when people debate what is, or isn’t a “high protein diet” they define it in terms of the percentage of calories in the diet but this is really meaningless.
For example, someone may be eating only 56 gm of protein which was 28% of the 800 calories per day they ate and someone else may be eating 160 gm of protein which is 34% of the 2000 calories they are eating per day.
Both are eating ~30% of calories as protein but there is a big difference between 56 gm of protein and 160 gm of protein.
According to Dr. Donald Layman PhD [1], when we speak of a “high protein diet”, we need to discuss the absolute amount of protein in grams, not as a percentage of calories, because adequacy in determined on the basis of absolute intake.
The Recommended Daily Allowance (RDA) for Protein
The Recommended Daily Allowance (RDA) for any nutrient is the average daily dietary intake level that is sufficient to meet the requirements of 97 – 98 % of healthy people. This is not the optimum requirement, but the absolute minimum. The RDA for Protein, Carbohydrate and Fat are as follows;
Protein: 56 g (224 kcals)
Carbohydrate: 130 g* (520 kcals)
Fat: 30 g (270 kcals)
The RDAs for Carbohydrate[2] is set at 130 g / day, but as established in an earlier article, How Much Carbohydrate is Essential in the Diet, we know that even in the absence of dietary carbohydrate (not recommended!), the minimum amount of glucose needed by the brain of 130 g / day can be made from protein and fat, provided they are eaten in adequate amounts.
The RDA for Protein is set at 56 gm per day, so whether a person is eating 800 calories a day or 2000 calories per day, their body has an absolute requirement for 56 gm of protein per day.

This range from 56 g to 200 g of protein per day is referred to as the range of safe intake[2].
According to Dr. Layman, a high protein diet doesn’t start “until well above 170 g / day“.
There are low carb diets that are higher in protein than others, and to distinguish between the two, the one that is higher in fat than protein (in grams) is referred to as a low carb high fat (LCHF) diet and the one that is higher in protein (in grams) is referred to as a low carb high protein (LCHP) diet – but it really isn’t “high protein”, but higher protein.
Current Dietary Intakes – the problem with carbs
Protein Intake in the US and in Canada is ~70 g of protein per day in women and in men about 90 g of protein per day (~15-16% of calories). Given the range of safe intake of protein from 56 g to 200 g of protein per day, dietary intake of protein in the US and Canada is very low.
The RDAs of macronutrients, which is the minimum amount required per day is just over 1000 calories per day, as follows;
Protein: 56 g (224 kcals)
Carbohydrate: 130 g (520 kcals)
Fat: 30 g (270 kcals)*
1017 calories*
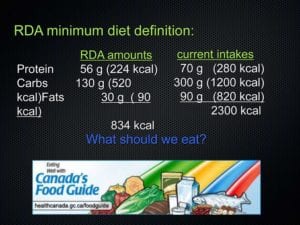
Current Intake of macronutrients is as follows;
Protein: 70 g (280 kcals)
Carbohydrate: 300 g (1200 kcals)
Fat: 90 g (820 kcals)
2300 calories
***That means there are between 1000 calories and 1300 calories per day of ‘discretionary calories’ – calories above and beyond the minimum requirements of 97-98% of healthy individuals.***
How should we eat to make the most of these calories?
What is going to give us the best health?
Currently, we are eating 3 times the RDA for carbohydrate (300 g carbohydrate per day!) and very close to the minimum for protein. Is this the right balance?
What evidence is there for this being the ‘right balance’?
Eating Well with Canada’s Food Guide, as with the US Dietary Recommendations emphasizes lots of whole grains and high carb intakes and very low protein intake. For a long time in both countries, we’ve highlighted that the issue is fat. But is this correct?
It was thought that since fat has a high caloric density, reducing fat intake would reduce calorie intake and that’s where the US Food Pyramid and Eating Well with Canada’s Food Guide comes from.
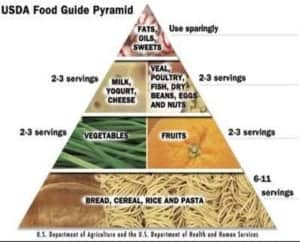
In both cases, the message is ‘stay away from fats‘, ‘stay away from proteins‘, ‘eat lots of cereal grains‘.
So how did that work out for us?
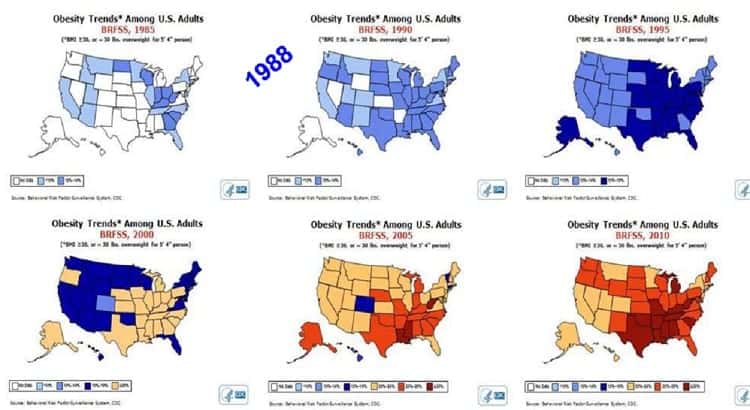
The Food Guide Pyramid first appeared in the US in 1988- exactly when obesity rates exploded. It tracks back almost to the date…obesity, Diabetes.
This occurred as we started consuming more and more cereal grains and this, according to Dr. Layman “is the origin of the problem”.
Let’s first look at children;
- In 1978, only 15% of children and adolescents were overweight or obese.
- By 2007, that rate had doubled to 29% of children and adolescents being overweight or obese.
- By 2011, obesity prevalence alone for boys was 15.1% and for girls was at 8.0% in 5 to 17 year olds.
What about adults?
- The prevalence of obesity [body mass index (BMI) ≥30 kg/m2] in Canadian adults increased from 10% in 1970-72 to 26% in 2009-11
- Based on waist circumference 37% of adults and 13% of youth are abdominally obese.
- Looking at these numbers slightly differently, as of 2013, there were approximately 7 million obese adults and 600 000 obese school-aged children in Canada.
What exactly changed in the Dietary Guidelines that caused us to get fat?
For one, Dr. Layman points out, caloric intake was increased by 300 calories per day and according to the Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010 these extra 300 calories per day came from these 6 categories:
- grain based desserts and snacks
- yeast bread
- pasta
- pizza
- chicken and chicken products
- soda and sports drinks
These are all grain-derived products in excess of our caloric needs. See the pattern? The fifth category includes breaded chicken products, such as chicken fingers and chicken nuggets and even soda and sports drinks, sweetened with high fructose corn syrup are grain derived.
All of these grain-derived products are in excess of our caloric needs. This is only part of the problem with current dietary intake of carbohydrates.
In the next article in this series, I’m going to take a look at our current high intake of dietary carbohydrates in terms of the history of man’s diet and the length of time that we’ve had to adapt to eating them.
You can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
References
1 – Layman, Donald, The Evolving Role of Dietary Protein in Adult Health, Nutrition Forum, British Columbia, Canada, June 23, 2013 https://youtu.be/4KlLmxPDTuQ
2 – Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids (2005), pg 275
3 – Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010
Copyright ©2018 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.