A new consensus report from an expert panel made up of representatives from the American Diabetes Association (ADA), European Association for the Study of Diabetes (EASD) and Diabetes UK [1,2,3] have proposes a standard definition for remission of type 2 diabetes. This new article outlines the different factors involved in that definition, as well as the proposed cut-offs.
As outlined in a previous article, in 2009 the American Diabetes Association defined partial remission, complete remission and prolonged remission of type 2 diabetes as follows [4];
Partial remission is having blood sugar that does not meet the classification for Type 2 Diabetes; i.e. either HbA1C < 6.5% and/or fasting blood glucose 5.5 — 6.9 mmol/l (100—125 mg/dl) for at least 1 year while not taking any medications to lower blood glucose.*
Complete remission is a return to normal glucose values i.e. HbA1C <6.0%, and/or fasting blood glucose < 5.6 mmol/L (100 mg/dl) for at least 1 year while not taking any medications to lower blood glucose.
Prolonged remission is a return to normal glucose values (i.e.
HbA1C <6.0%, and/or fasting blood glucose < 5.6 mmol/L (100 mg/dl) for at least 5 years while not taking any medications to lower blood glucose.
In 2019, the Association of British Clinical Diabetologists and the Primary Care Diabetes Society [5] defined remission of type 2 diabetes as follows;
“Remission of type 2 diabetes can be diagnosed when a person with confirmed type 2 diabetes has achieved all three of the following criteria: (1) weight loss; (2) fasting plasma glucose or HbA1c below the WHO diagnostic threshold (<7 mmol/L or <48 mmol/mol, respectively) on two occasions separated by at least 6 months; (3) the attainment of these glycaemic parameters following the complete cessation of all glucose-lowering therapies.”
I am by no means an expert in diabetes, but in clinical practice I’ve defined remission of type 2 diabetes as blood sugar levels “at or below the cut-offs for diagnosis” (HbA1C & FBG) without the use of medication.
Choice of the Term “Remission”
The consensus report’s expert panel outlined that while several terms have been proposed to describe those who have become free of a previously diagnosed disease state, including ‘resolution‘, ‘reversal‘, ‘remission‘, and ‘cure‘, that with respect to type 2 diabetes ‘remission‘ is the most appropriate term [1,2,3]. They chose the term remission as it is used widely used in the field of cancer treatment (oncology) as defined as a decrease in or disappearance of signs and symptoms of cancer [6].
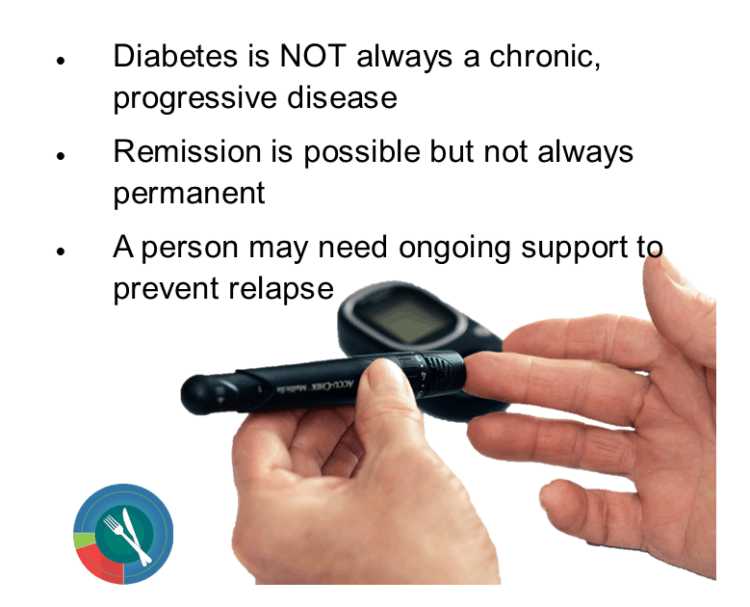
The expert panel believes that the term remission captures that (1) “diabetes may not always be active and progressive“, while also implying that (2) “notable improvement may not be permanent“, and (3) is consistent with the view that a person may need ongoing support and regular monitoring to prevent relapse [1,2,3].
“Remission” Not Equivalent to No Evidence of Disease
The panel highlighted that the tendency to equate remission with “no evidence of disease” is not appropriate with respect to type 2 diabetes because diabetes is defined by hyperglycemia, which exists on a continuum [1,2,3], and noted that any criterion chosen to define remission is somewhat arbitrary, as it represents a point on a continuum of glycemic levels. They also highlighted that remission is not equivalent to “no evidence of disease” because the underlying cause of type 2 diabetes is rarely resolved by dietary or lifestyle changes, or by bariatric surgery — including insufficient release of insulin from βeta-cells and insulin resistance.
Different Levels of Remission
The panel decided against dividing diabetes remission into partial remission and complete remission using different blood glucose thresholds as this could result in challenges with respect to policy decisions related to insurance premiums, and coding for medical visits and that the 5-year threshold previously used by the ADA for defining prolonged remission “did not have an
objective basis”.
Use of Glucose-Lowering Medication in Defining Remission
The issue of whether remission could be diagnosed while a person was receiving ongoing medication support, was also addressed. This is an important consideration, as some studies such as those from Virta Health [7,8] define remission of type 2 diabetes as a HbA1C < 6.5% and fasting blood glucose ≤ 5.5 (100 mg/dl) while taking no other medication except metformin / glucophage.
The panel concluded that since it is not possible to tell if a person has achieved remission due to dietary and lifestyle changes or due to medication that lowers glucose, “a diagnosis of remission can only be made after all glucose-lowering agents have been withheld for an interval that is sufficient both to allow waning of the drug’s effects and to assess the effect of the absence of drugs on HbA1c values“.
The panel concluded the absence of medication includes the use of metformin for weight maintenance, to improve markers of risk for cardiovascular disease or cancer, or prescribed for polycystic ovarian syndrome (PCOS), GLP-1 receptor agonists (such as Ozempic, Victoza / Saxenda and others) which may be used for weight management or to reduce the risk of cardiovascular events, and sodium glucose cotransporter inhibitors (such as Invokana, Jardiance, Synjardy and others) which may be prescribed for heart failure or renal protection.
The panel concludes that if it is not possible to discontinue these drugs for 3 months or longer, then remission cannot be diagnosed even though
normal or near normal blood sugar values are maintained — and that without doing so “whether true remission has been attained remains unknown”.
Timeline for Determining Remission
Whether the changes made are dietary, lifestyle or surgical (such as gastric bypass), varying amounts of time are required to determine whether remission has been achieved.
Medication Intervention (Pharmacotherapy)
The expert panel determined that when the intervention has been through medication (pharmacotherapy), there needs to be a period of at least 3 months after the medication has been completely stopped before tests of HbA1C can reliably evaluate whether remission has been achieved.
Surgical Intervention
In the event of surgical intervention, the panel determined that there needs to be a period of at least 3 months after the surgical procedure and 3 months after the medication has been completely stopped before tests of HbA1C can reliably evaluate whether remission has been achieved.
Lifestyle Changes
When lifestyle changes, including diet and exercise are made, the panel determined that there needs to be a period of at least 6 months after beginning this intervention and 3 months after the medication has been completely stopped before tests of HbA1C can reliably evaluate whether remission has been achieved.
Need for Ongoing Monitoring
As outlined above, since the improvements in blood glucose may not be permanent, a person who has achieved remission from type 2 diabetes as defined above will likely need ongoing support and regular monitoring to prevent relapse as weight gain, stress resulting from other illnesses, and the continued decline of βeta-cell function can all result in recurrence of type 2 diabetes. The panel recommends regular laboratory testing of HbA1c or another measure of blood sugar control should be performed at least once a year.
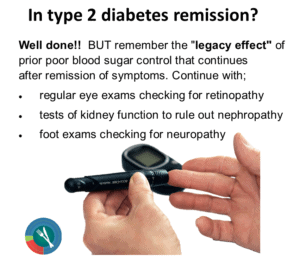 The panel cautions that since there can still be the “legacy effect” of prior poor blood sugar control in various body tissues that continues after remission of symptoms, there is a need not only for ongoing monitoring of HbA1C, but also regular retinal screening for retinopathy, tests of renal function to rule out nephropathy, foot evaluation to rule out neuropathy, as well as measurement of blood pressure and weight to reduce the risk of cardiovascular disease.
The panel cautions that since there can still be the “legacy effect” of prior poor blood sugar control in various body tissues that continues after remission of symptoms, there is a need not only for ongoing monitoring of HbA1C, but also regular retinal screening for retinopathy, tests of renal function to rule out nephropathy, foot evaluation to rule out neuropathy, as well as measurement of blood pressure and weight to reduce the risk of cardiovascular disease.
HbA1c as the Defining Measurement of Remission
The expert panel set the cut-off point for defining remission as HbA1c to < 6.5% (<48 mmol/mol) while stating that “the relative effectiveness of using HbA1C of 6.0% (42 mmol/mol), HbA1c of 5.7% (39 mmol/mol), or some other
level in predicting risk of relapse or microvascular or cardiovascular complications should be evaluated“. As noted above, the panel believes that any criterion chosen to define remission is somewhat arbitrary, as it represents a point on a continuum of glycemic levels.
Conclusions of the Expert Panel
The expert panel concluded that the term “remission” should be used to describe a sustained metabolic improvement in type 2 diabetes to nearly normal levels defined as a return of HbA1c to < 6.5% (<48 mmol/mol) that occurs spontaneously, or following an intervention and that persists for at least 3 months in the absence of usual glucose-lowering medication (pharmacotherapy).
When HbA1c is determined to be an unreliable marker of chronic glycemic control, the panel concluded that a fasting blood glucose (FBG) / fasting plasma glucose (FPG) <126 mg/dL (<7.0 mmol/L) or eA1C <6.5% calculated from continuous glucose monitoring (CGM) values can be used as an alternative.
Final Thoughts…
In addition to the new proposed cut-offs, there are three very important points made in this new consensus report:
NOTE: Be sure to read the following post about why it is time to stop calling type 2 diabetes ”a chronic, progressive disease”.
More Info?
If you would like more information about how I can support you in seeking remission of type 2 diabetes as defined above, please have a look around my web page, or send me a note through the Contact Me form.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchfRD/
Instagram: https://www.instagram.com/lchf_rd
Note: A consensus report is not an American Diabetes Association (ADA) position statement but represents expert opinion of this international expert panel’s collective analysis, evaluation, and opinion.
References
- Riddle MC, Cefalu WT, Evans PH. et al. Consensus Report: Definition and Interpretation of Remission in Type 2 Diabetes, The Journal of Clinical Endocrinology & Metabolism, 2021, dgab585, https://doi.org/10.1210/clinem/dgab585
- Riddle MC, Cefalu WT, Evans PH. et al. Consensus report: definition and interpretation of remission in type 2 diabetes.
- Riddle MC, Cefalu WT, Evans PH. et al. Consensus report: definition and interpretation of remission in type 2 diabetes. Diabetologia (2021). https://doi.org/10.1007/s00125-021-05542-z
- Buse JB, Caprio S, Cefalu WT, et al. How do we define cure of diabetes?
- Nagi D, Hambling C, Taylor R. Remission of type 2 diabetes: a position statement from the Association of British Clinical Diabetologists (ABCD) and the Primary Care Diabetes Society (PCDS). Br J Diabetes 2019, June 2019; 19 (1):73—76. https://doi.org/10.15277/bjd.2019.221
- Barnes E. Between remission and cure: patients, practitioners and the transformation of leukaemia in the late twentieth century. Chronic Illness 2008, Jan 2008;3(4):253—264.https://doi.org/10.1177/1742395307085333
- McKenzie AL, Hallberg SJ, Creighton BC, Volk BM, Link TM, Abner MK, Glon RM, McCarter JP, Volek JS, Phinney SD, A Novel Intervention Including Individualized Nutritional Recommendations Reduces Hemoglobin A1c Level, Medication Use, and Weight in Type 2 Diabetes, JMIR Diabetes 2017;2(1):e5, URL: http://diabetes.jmir.org/2017/1/e5, DOI: 10.2196/diabetes.6981
- Hallberg, S.J., McKenzie, A.L., Williams, P.T. et al. Diabetes Ther (2018). Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. https://doi.org/10.1007/s13300-018-0373-9
Copyright ©2021 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.