
This article is the fourth entry in A Dietitian’s Journey Part II, which began with my recent diagnosis of hypothyroidism. This post is about how I will measure success as I recover from hypothyroidism.
NOTE: Articles posted under A Dietitian’s Journey are separate from referenced clinical articles (categorized as Science Made Simple articles) because these are about what happened to me (i.e., anecdotal) and based on my personal observation.
A Dietitian’s Journey – Part I

“A Dietitian’s Journey” (Part I) was my personal weight-loss and health-recovery journey that began on March 5, 2017 when I decided to make dietary and lifestyle changes so that I could reclaim my health. At that time, I was obese, had type 2 diabetes for the previous 8 years, and extremely high blood pressure.
Two years later, on March 5, 2019, I accomplished all but one of my goals, and the last one I achieved three months later. In all, I lost 55 pounds and more than a foot off my waist, and met the criteria for partial remission of type 2 diabetes, and remission of hypertension (high blood pressure).
To get an idea of what I looked like at the beginning and the end of that journey, there are two short videos on my Two Year Anniversary post that tell the story well. The first video was taken when I started and it is very apparent how obese I was, and how difficult it was for me to walk and talk at the same time. The second clip was taken when I completed my journey, and the difference is unmistakable.
A Dietitian’s Journey – Part II
Without much difficulty I maintained my health and my weight-loss from March 2019 until August 2020 but then I came down with Covid. This was at the very beginning of the pandemic and no one really knew what to expect in terms of symptoms. As you can read about in the first post in what has become A Dietitian’s Journey Part II, (When a New Diagnosis is a Long Time Coming ) I had symptoms that both my doctor and I assumed were related to the virus, including muscle aches and joint pain, being exhausted, having ‘brain fog,’ headaches, and having the shivers.
Afterwards, I had to work very hard to regain my mobility. No one knew this wasn’t ‘normal.’
At first, I could barely walk up a flight of stairs. At the time, “success” was being able to walk around the block. Then I began taking several dietary supplements to help strengthen my immune system and in retrospect, the reason I felt better was likely due to the fact that these were all supplements involved in thyroid support. Success at the time was being able to walk around the man-made lake at the local park, but over the weeks and months of supplementing my diet and walking every weekend, success was being able to complete several medium difficulty hikes in the local mountains.
Unfortunately, in March of 2022, I came down with what my doctor assumed was Covid again. At first the symptoms were similar to what I experienced in August 2020, including muscle aches, joint pain, being exhausted, feeling cold all the time, with the only difference being that I didn’t have headaches. The symptoms persisted for several months and I was beginning to think that I had “long-Covid.” As most people did over the pandemic, I put on 20 pounds, but from March to May, I began to look as though I was putting on significant weight, but every time I got on the scale it indicated only a few pounds of difference. I had no idea what was going on.
 The next symptom that I became aware of was swelling in my ankles. It wasn’t just a little bit of swelling, but significant enough that I needed to wear compression stockings all day.
The next symptom that I became aware of was swelling in my ankles. It wasn’t just a little bit of swelling, but significant enough that I needed to wear compression stockings all day.
At my youngest son’s wedding at the beginning of June, I looked like I did when I was 55 pounds heavier, but I wasn’t.

About three weeks after the wedding, I was diagnosed with hypothyroidism, and started taking desiccated thyroid. At first, I felt significantly better, and within several weeks, the edema in my legs began to subside.

There is still a fair amount of mucin accumulation in my legs, but as of this weekend, I can begin to grab a very small amount of flesh between my fingers. From what I have read it will take at least 6 months for this to resolve. You can read a referenced article about the skin symptoms associated with hypothyroidism here.
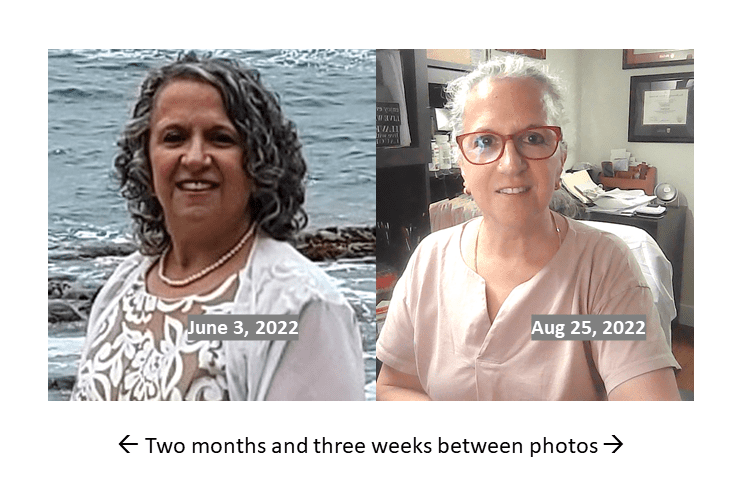
It is easy to see from the above photo that in less than 3 months on thyroid medication treatment, my face has lost its puffy, “inflated” look yet amidst the positive improvements of decreased edema and looking more like myself in some respects is the reality that I have lost ~1/2 of my hair due to telogen effluvium that often occurs with sustained hypothyroidism. You can read more different causes for hair loss here.

Even though I have already been on thyroid replacement hormones for several months, it usually takes ~3-6 months for hair loss to stop and another 3-6 months for regrowth to be seen and 12-18 months to complete regrowth [3]. For someone like my who has lost half their hair, six months to a year to begin to see hair growth can seem like an eternity.
I recently changed medication forms from desiccated thyroid to a mixture of T4 medication (Synthroid®) and T3 medication (Cytomel®). The overall distribution of T4:T3 is about the same, but it is hoped that this mixture will result in more stable thyroid hormones day-to-day.
In six weeks I will have new blood tests to re-evaluate whether my levels have improved. At last check, my TSH was still high-normal (3.47 mU/L) when in most patients on thyroid hormone replacement the goal TSH level is between 0.5 to 2.5 mU/L [7]. My Free T4 = 14.0 pmol/L which is still in the lower end of the range (10.6-19.7 pmol/L) when it is considered optimal to be in the higher end of the range.
Metabolic Changes due to Hypothyroidism
It’s well known that people with hypothyroidism experience several clinical changes including different type of anemia, changes in how their heart functions, changes in blood pressure, blood sugar and cholesterol and weight gain due to a slower metabolism. My recent medical work up indicates that I was no different in this regard.
Different Types of Anemia
People with hypothyroidism have a decrease in red blood cells and experience different types of anemia, including the anemia of chronic disease. In addition, 10% of people with hypothyroidism develop pernicious anemia, which is associated with vitamin B12 and folate (folic acid). Iron deficient anemia is also common due to decreased stomach acid that results in decreased absorption of iron.
I was supplementing with B12 and folate and as a result have no signs of pernicious anemia, however my hematology panel indicates that I may have iron deficient anemia. An iron panel would be able to quantify this, however I am already taking heme iron supplements, along with vitamin C to support absorption.
Heart Changes
The slowing of metabolism associated with hypothyroidism also results in a decrease in cardiac (heart) output, which results in both slower heart rate and less ability for the heart to pump blood. This is what results in the unbearable fatigue.
High Blood Pressure
The decreased ability of the heart to pump leads to increased resistance in the blood vessels, which results in increased blood pressure (hypertension).
In those who had normal blood pressure previous to developing hypothyroidism, blood pressure can rise as high as 150/100 mmHg. Hypothyroidism may increase it further for those previously diagnosed with high blood pressure. While my blood pressure had been normal for more than a year, it gradually started increasing the last year, which in retrospect is the period of time over which I was exhibiting more and more symptoms of hypothyroidism. I have since been put back on medication for hypertension to protect my kidneys, which I hope to be able to get off of again within the next six month to a year, as my thyroid hormones normalize.
Weight Gain
Thyroid hormones act on every organ system in the body, but the thyroid is well-known for its role in energy metabolism. When someone has overt hypothyroidism, there is a slowing of metabolic processes, which results in symptoms such as fatigue, cold intolerance, constipation, and weight gain.
Weight gain is not only about diet or how much someone eats versus how much they burn off. It is also about the person’s metabolic rate, which can be impacted by several things, including decreased thyroid hormones. I gained 20 pounds over the pandemic (much of which overlaps with the period of time over which I was exhibiting more and more symptoms of hypothyroidism. I also gained 10 pounds from March to June which is mostly water weight, due to the mucin accumulation.
High Cholesterol
It has long been known that those with hypothyroidism have high total cholesterol, high low-density lipoproteins (LDL) [4], and high triglycerides (TG) [5], which results from a decrease in the rate of cholesterol metabolism. My doctor deliberately did not want to check these last time, because he knew they would be abnormal only as a result of the hypothyroidism. He plans to evaluate them once I have been stable on hormone replacement for several months.
So, What Does Success Look Like Now?
Over the next year, this is what I want to accomplish;
-
- weight same as March 5, 2019 (end of A Dietitian’s Journey, part I)
- waist circumference same as March 5, 2019 (end of A Dietitian’s Journey, part I)
- regrowth of my hair to same thickness as before clinical symptoms of hypothyroidism
- restoration of iron deficient anemia:
(a) normal ferritin 11-307 ug/L
(b) iron 10.6-33.8 umol/L
(c) TIBC 45–81 µmol/L
(d) transferrin 2.00-4.00 g/L - Blood pressure ≤ 130/80 mmHg
- Blood sugar:
(a) non-diabetic range fasting blood glucose ≤ 5.5 mmol/L
(b) non-diabetic range HbA1C ≤ 5.9 % - Thyroid Hormones:
(a) optimal TSH= 0.5 to 2.5 mU/L
(b) optimal Free T4 = 15-18 pmol/L (10.6-19.7 pmol/L) - Cholesterol:
(a) LDL ≤ 1.5 mmol/L
(b) TG ≤ 2.21 mmol/L
Final Thoughts…
While I don’t know if it will be possible to achieve all of these within the time frame or within adjustments to medication that my doctor will be willing to make, these are my goals. I believe that most of these are possible, and as far as they are within my control, this is what I would like to accomplish.
I have achieved a lot the last 3 months, but I am not “done.” I want the rest of my life back!
I want to be able to do the things that I enjoy, and to have the freedom to make plans in the evening knowing I will have the energy to follow through.
I think this is reasonable to ask and I will do everything I can to make this a reality.
A Dietitian’s Journey Part II continues…
To your good health,
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchfRD/
Instagram: https://www.instagram.com/lchf_rd
References
- Rotondi M et al. Serum negative autoimmune thyroiditis displays a milder clinical picture compared with classic Hashimoto’s thyroiditis. Eur J Endocrinol 2014;171:31-6. Epub April 17 2014
- Croce, L., De Martinis, L., Pinto, S. et al. Compared with classic Hashimoto’s thyroiditis, chronic autoimmune serum-negative thyroiditis requires a lower substitution dose of L-thyroxine to correct hypothyroidism. J Endocrinol Invest 43, 1631–1636 (2020). https://doi.org/10.1007/s40618-020-01249-x
- Malkud S. Telogen Effluvium: A Review. J Clin Diagn Res. 2015;9(9):WE01-WE3. doi:10.7860/JCDR/2015/15219.6492
-
Lithell, H., Boberg, J., Hellsing, K., Ljunghall, S., Lundqvist, G., Vessby, B., & Wide, L. (1981). Serum lipoprotein and apolipoprotein concentrations and tissue lipoprotein-lipase activity in overt and subclinical hypothyroidism: the effect of substitution therapy. European journal of clinical investigation, 11(1), 3–10. https://doi.org/10.1111/j.1365-2362.1981.tb01758.x
- Nikkila E, Kekki M, Plasma triglyceride metabolism in thyroid disease, J Clin Invest. 1973;51:203.
- Iron Disorders Institute, Iron Deficiency, Understanding Iron Deficiency Anemia, http://irondisorders.org/iron-deficiency-anemia/
- American Thyroid Association, Is the TSH (thyroid stimulating hormone) a good way to titrate my thyroid hormone therapy? https://www.thyroid.org/patient-thyroid-information/what-are-thyroid-problems/q-and-a-tsh-thyroid-stimulating-hormone/
DISCLAIMER: The information in this post should not be taken as a recommendation to self-diagnose, self-interpret diagnostic tests, or self-treat any suspected disorder. It is essential that people who suspect they may have symptoms of any condition consult with their doctor, as only a medical doctor can diagnose and treat.
Copyright ©2022 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.