Three years ago, my theory about the roots of the current obesity and Diabetes epidemic was simple. I believed that it was largely a matter of us eating too many carbs while having reduced the amount of healthy fat we ate. I now think it is a little more subtle than that, and that it is specifically the combination of a diet too high in refined carbs while high in industrial seed oils (such as soybean and canola oil) that underlies the issue.
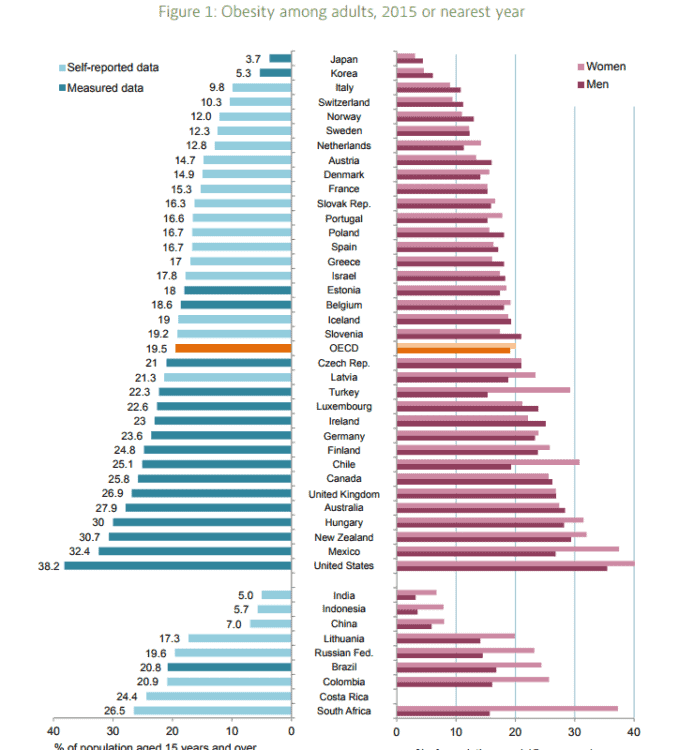
When I first started reading and writing about the current obesity and Diabetes epidemic, my thoughts were summarized in two articles written in May and June of 2015. In the first article, I documented how in 1970-72 only 6% of men and 11.7% of women were considered obese (Body Mass Index > 30) in Canada, but by 2013 obesity in men had tripled to 20.1% in men and to 17.4% in women. In the second article, I explained how the changes in the obesity rates coincided with the changes in the Dietary Recommendations that began in 1977 and continued in 1982, 1992 and 2005 and which encouraged people to eat considerably more carbs and a lot less fat coincided with the increased obesity rates, and that the increasing rates of Type 2 Diabetes (9.4% in 2014 in Canada) was just a natural outworking of the higher obesity rates.
The problem was, I really didn’t know of any specific mechanisms that related one to the other.
Now I know of several.
This article summarizes my current theory of obesity, as it relates to previous articles and a brand new study published last week.
Correlation is not Causation
There’s an expression in science is that “correlation is not causation”.
That is, the fact that a dramatic increase in obesity rates correlates (or coincides) with the changes in the Dietary Recommendations doesn’t mean that the Dietary Recommendations ’caused’ the obesity epidemic or the Diabetes epidemic.
One can hypothesize that there is a relationship between these two things, but without some understanding of the mechanism and more data, we don’t know what this relationship might be.
From the reading I have been doing the last number of years, I have some ideas of some of what may be involved.
Evolution of the Theory
A presentation at a conference at the beginning of March (documented in two previous articles) got me thinking that the picture was bigger than just “too many carbs” and a “decrease in the satiety effect of saturated fat” from full fat milk, cheese and butter. I was challenged by the fact that in the late 1960s and early 1970s, people in the US and Canada were generally slim, despite eating carbohydrates at just about every meal;
“They ate cereal or toast for breakfast and just about every household had a toaster. Lunch was often sandwiches, as there were no microwaves to heat food up in. Potatoes were a mainstay at dinner, sometimes pasta — yet the majority of young adults and adults were slim. Of course there were always some people that were overweight. Most elementary school classes had one chubby’ kid, but when one looks around the classes of today or on public transit or in stores and supermarkets, most people are considerably heavier than people in the 1950’s and 1960’s”
The question was raised ‘what resulted in overweight and obesity all of a sudden exploding in the 1970’s and just keep rising?’
What changed?
We knew that (based on US data) people began eating ~240 calories a day more as carbohydrate but what was causing them to do this? Was it just because the Dietary Recommendations were encouraging us to eat more carbohydrate or was there something else going on?
Not More Fat but the Type of Fat
While people were eating more carbohydrate, neither people in Canada nor the US were eating more fat, but the type of fat we’ve been eating since the 1970s has changed substantially. This tweaked my interest.
We’d reduced our intake of saturated fat (because the “Diet-Heart Hypothesis” had told us they were the “cause of cardiovascular disease”) and we dutifully ate more and more of ‘polyunsaturated fats’ / vegetable oils which as I wrote about previously are more appropriately called “industrial seed oils”. These oils, including soybean, corn oil and canola oil contain high amounts of linoleic acid which is at the very top of the omega 6 (n-6) pathway and these fats which elongate to arachidonic acid are pro-inflammatory products in nature.
There is nothing inherently ‘bad’ about linoleic acid which is found naturally in nuts and seed oils, including walnut, macadamia and sesame oil, but it is the sheer amount of these industrial seed oils which suddenly became excessive in our diet, which I think may be a significant factor. These fats are in our bread, pastries, salad dressing, margarine and even our peanut butter. Canned fish is packed in it, our mayonnaise is made from it and everything we eat that is fried from a restaurant is bathed in these industrial seed oils. On top of that, many of us use it our own homes to cook with.
So many of the foods we now eat are prepared with soybean or canola oil and as a result, we consume a much greater amount of linoleic acid than our body ever evolved to handle.
As outline in previous articles, these oils are much more unstable than the saturated fats they were created to replace. What I mean by ‘unstable’ is that they are more easily oxidized – that is, when industrial seed oils are heated in the making of commercial foods using them or in cooking, they react with oxygen in the air to form toxic substances including aldehydes and lipid peroxides. When these oils are heated, they produce oxidized metabolites which have been also been implicated in the development of a variety of conditions, including non-alcoholic fatty liver disease (NAFLD), cardiovascular disease and cancer and it has been proposed that inflammation is involved in the development of Type 2 Diabetes and metabolic syndrome, as well.
Also as written about previously, cardiolipin is an important component of the inner membrane of the mitochondria (the so-called “powerhouse of the cell”) and the fats that make up cardiolepin change, depending on the types of fats in the diet. That is, the fatty acid composition of cardiolepin is altered by us eating a diet high in linoleic acid, such as soybean and canola oil. This past week a study about cardiolepin was published that added a very interesting piece to my evolving theory of the obesity and Type 2 Diabetes epidemic.
In this new study, researchers at the University of Copenhagen found that when large amounts of cardiolipin are produced in ‘brown fat’ cell mitochondria, there is much stronger calorie-burning. Conversely, when there are low amounts of cardiolepin in brown fat, there is much less calorie-burning. Low amounts of cardiolepin and less calorie-burning in brown fat was reported to be associated with obesity and Type 2 Diabetes [1].
Note: “Brown fat” is a specialized type of fat that burns fat, rather than stores it and cardiolepin acts like a kind of on-off switch for the activity in our brown fat.
This study got me thinking that since it is known that the fatty acid composition of cardiolepin changes according to the fatty acid composition of the diet (covered in previous blogs), what effect has the massive increase in linoleic acid intake in the diet in both Canada and the US had on the function of the cardiolipin?
Could it be that a shift in the types of fats that make up cardiolepin in brown fat stemming from a very high linoleic acid intake from industrial seed oils has had a similar effect as an absolute decrease in cardiolepin – and that this is somehow related to the increase in obesity and Type 2 Diabetes?
Type of Fats and Refined Carbohydrates
My theory of obesity has evolved and will likely continue to evolve. I don’t think that increased carbohydrate consumption based on changes in the Dietary Recommendations in the late 1970s / early 1980s in and by itself resulted in the obesity epidemic and huge increase in Type 2 Diabetes we see now.
I currently believe that the introduction of these manufactured industrial seed oils (soybean, canola, corn) that were created in the 1970s and meant to replace saturated fat in the diet (presumably to protect people from heart disease!) may be part of the initiation of the disease process.
As documented in earlier articles, we know that these fats are easily oxidized, have a direct impact on increasing inflammation and triggering the disease generation process in several health conditions and on acting on the endo-cannibinoid receptors in the body, in much the same way as cannabis (marijuana). Could it be that these created oils that are very high in the average Western diet actually lead people to consuming more and more carbohydrate-based foods; foods that often comes liberally bathed in more industrial seed oils?
The mechanism of how the above might work was presented in an earlier article and had to do with how energy is generated in the electron transport chain of the mitochondria being different for saturated fats and unsaturated fats.
There are several possible mechanisms that may link consumption of these novel fats to obesity and development of Type 2 Diabetes (oxidation, inflammation, food cravings) and now based on this new study, the possibility of an increase in linoleic acid content in cardiolepin and it’s effect on fat burning.
It will take years more research before we have a fuller picture, so what do we do in the meantime?
Sensible Recommendations based on the Current Knowledge
For someone who is metabolically healthy (i.e. does not have Type 2 Diabetes or Insulin Resistance, hypertension or high cholesterol), it would seem that a whole-foods approach combined with avoiding omega – 6 industrial seed oils such as soybean, canola and corn oil combined with being mindful of the amount and type of carbohydrate in the diet may be sufficient to avoid developing these chronic diseases. Such a scenario would not be unlike the diet of the average American or Canadian in the 1950s and 60s. Not that that diet was that healthy, when compared with a classic Mediterranean diet, Japanese or Okinawan-style diet, or a whole food low-carbohydrate diet. These, it would seem offer a much healthier alternative.
For those who are already are insulin resistant or been diagnosed with Type 2 Diabetes, avoiding industrial seed oils would prudent and eating naturally-obtained vegetable fats such as olive oil or avocado oil instead. Since it does not seem that studies clearly support that saturated fat causes heart disease and not simply increase in surrogate markers of heart disease such as higher LDL (which LDL subfraction?), it would seem that using modest quantities of real butter is preferable to eating margarine made from industrial seed oils. It would also seem that at least initially, eating a diet where the amount and type of carbohydrate is kept to a quantity that does not trigger large amounts of insulin release or spike blood glucose makes good sense. As I wrote about recently, with the availability of Continuous Glucose Monitoring (CGM), this approach can be tailored to each individual person’s response to specific foods. We are no longer reliant on Glycemic Index or Glycemic Load, which are derived from healthy people’s response to foods, not those with Type 2 Diabetes. A suitable diet could be expressed as a variety of different lifestyles (just as for the healthy individual) including a Mediterranean diet, Okinawan-style diet, or whole food low-carbohydrate diet – with carbohydrate levels tailored on an individual basis, based on glycemic response and insulin levels.
Whether a person is healthy or metabolically unwell, based on the studies I have read and some of the mechanisms that have come to light, I can see no benefit in people eating either industrial seed oils or refined, processed carbohydrates. There is every reason to believe that both of these may have been part of the underlying cause of the current obesity and Type 2 Diabetes epidemic.
Unrefined Carbohydrates and Healthy Fats
If someone is metabolically healthy, I recommend eating minimally processed carbohydrates as they reduce the ‘incretin effect’ of hormones such as GIP, GLP-1 and GLP-2 that are released in the intestine and trigger the release of insulin from the pancreas beta-cells. Eating minimally processed carbs would result in less triggering of the release of insulin, thus reducing the likelihood of developing either insulin resistance or Type 2 Diabetes.
If someone is already insulin resistant or has Type 2 Diabetes, it seems from recent studies that minimizing carbohydrate initially, along with weight loss and some forms of activity may be at least as good if not more beneficial than a low-fat calorie-restricted diet. Certainly, many people find they are a lot less hungry eating a low carbohydrate whole foods diet and are easily able to stick with it long term (a year or two in studies), allowing for a period of improving insulin sensitivity and lower overall blood sugar levels. It certainly has been demonstrated to be safe and effective in periods up to two years.
For both those that are metabolically healthy or insulin resistant or have Type 2 Diabetes, avoiding industrial seed oils makes good sense, for all the reasons outlined above.
What about your specific situation?
Do you have questions about the type and amount of carbohydrates that are most suitable for you based on your health and family history? What about which fats are are the best choices given your lifestyle?
I can help.
Please feel free to send me a note using the “Contact Me” form located on the tab above to find out how I can support your needs and I will reply as soon as possible. Remember, I provide both in-person services and am experienced providing services via Distance Consultation (telephone or Skype).
To your good health!
Joy
You can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
Reference
Sustarsic EG, Ma T, Lynes MD et al, Cardiolipin Synthesis in Brown and Beige Fat Mitochondria Is Essential for Systemic Energy Homeostasis,
Cell Metabolism (2018), https://doi.org/10.1016/j.cmet.2018.05.003
Copyright ©2018 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.











 In August 1967 the New England Journal of Medicine published the first review article written by Drs. Stare, Hegsted and McGandy titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which stated;
In August 1967 the New England Journal of Medicine published the first review article written by Drs. Stare, Hegsted and McGandy titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which stated;