

It occurred to me that the time frame for an epidemic to occur is absolutely critical in determining public response. If rates of a disease went from 1 in 10 people to 1 in 3 people in only 10 years, there would be public outcry for scientists to determine the cause and to find a cure quickly. If the disease caused debilitating metabolic effects such as very high blood pressure that resulted in heart attacks or strokes and people of all ages were getting this disease, with many dying – the outcry would be even more urgent.
But what if rates of the same disease went from 1 in 10 people to 1 in 3 people over a period of 40 or 50 years? The current generation would have no recollection of what it was like ‘before’ because things had always been this way since they were kids. The older generation would remember what it was like ‘before’ and concluding that for whatever reason, that is the way it is now. Doctors and scientists of the older generation that might be able to apply their knowledge and skill to find the cause and a cure would be at the end of their working lives.
The disease is obesity.
Debilitating metabolic side effects of obesity include very high blood pressure that can lead to heart attacks and strokes and Type 2 Diabetes which can result in blindness, amputations and organ failure.
Once a rare disease, obesity has now reached epidemic proportions and the metabolic side effects are not just for the old, but are rampant among youth and young adults.
This disease epidemic has taken place over 50 years but few are noticing because it has fallen between the cracks of time.
Obesity Rates Then and Now
Photographs and videos of what people looked like fifty years ago are widely available, and a simple Google search will provide an abundance of them. Movies, documentaries and TV shows from the mid-1960s also provide a glimpse of what the average American and average Canadian looked like then.
In the 1960s only 10.7% of the US population and 10.2% of the Canadian population were obese; that’s approximately 1 in 10 people.
Below is a US sorority photo of a Sigma Iota Chi chapter from West Virginia from 1967. Look how slim most of the women are compared to today’s young adults.

West Virginia now has one of the highest adult obesity rate in the US.
To the left is another photo from a 1967 Fraternity party at Cornell University. For the most part, the young men and their girlfriends are slim and lean – certainly much slimmer than university students today.
Below is what the average city-dwelling Canadian looked like in 1967, riding the subway in Toronto. Young adults, middle aged adults and older people were very slim compared to today’s standards – especially when compared to what the average public transit rider looks like today.

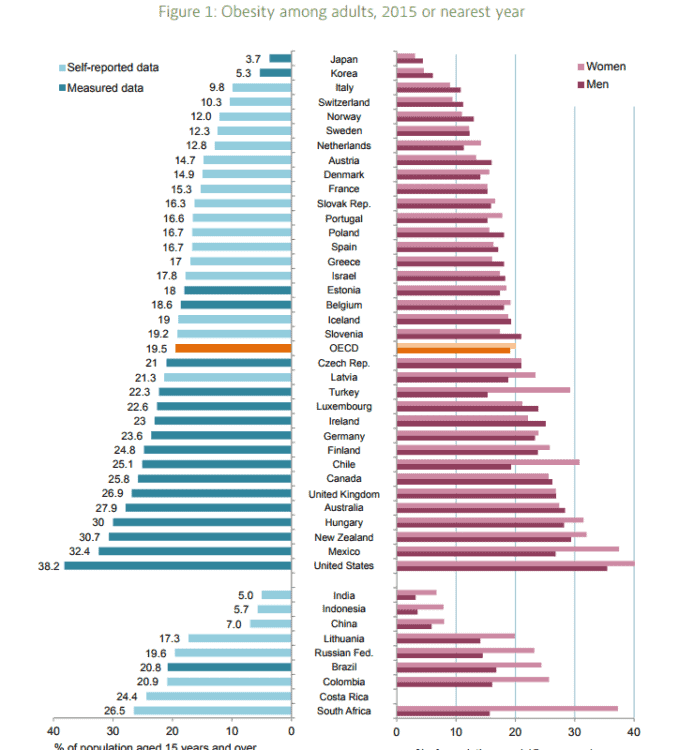
Most recent international data from 2015 found that 38.2% of the US population and 25.8% of the Canadian population are obese; that’s more than 1 in 3 people in the US and more than 1 in 4 people in Canada [1].
People in both countries are now some of the most obese in the world;
When one compares what university students looked above to what they look like now in a current photo of Fraternities and Sororities below, the difference in average body weight of the students from 50 years ago to today is quite apparent – despite the fact that university students come from families where the average family income is significantly higher than the national average.
Given this, their higher body weights cannot be dismissed due to low income, socioeconomic status or lack of education. So what is going on?

What changed in the last 50 years that contributed to this obesity epidemic?
As written about in a previous article, in 1967 (fifty years ago) the sugar industry paid three Harvard researchers (Stare, Hegsted and McGandy) very handsomely to critique studies that vindicated sugar as contributing to abnormal fat metabolism and heart disease, and who instead laid the blame on dietary fat, and in particular saturated fat and dietary cholesterol [2,3].
They concluded;
”Since diets low in fat and high in sugar are rarely taken, we conclude that the practical significance of differences in dietary carbohydrate is minimal in comparison to those related to dietary fat and cholesterol…the major evidence today suggests only one avenue by which diet may affect the development and progression of atherosclerosis. This is by influencing the levels of serum lipids [fats], especially serum cholesterol.” [4]
These researchers who were sponsored by the sugar industry concluded that there was “major evidence” which suggested that there was only ONE avenue for diet to contribute to hardening of the arteries and the development of heart disease – and that was dietary fat and cholesterol…yet only a year later in 1968, the Diet-Heart Review Panel of the National Heart Institute recommended that a major study be conducted to determine whether changes in dietary fat intake prevented heart disease – because such a study had not yet been done [5].
No major study had yet been done to find out whether changing the types of fat we ate prevented heart disease, yet these researchers were SO certain that there was “only one avenue” for diet to contribute to hardening of the arteries and the development of heart disease. How much was their certainly impacted by their sponsors?
Their influence didn’t end there.
Only ten years later, one of the three Harvard researchers (Hegsted) was directly involved with developing and editing the 1977 US Dietary Guidelines [6] which recommended a decrease in saturated fat and cholesterol consumption, and an increase in dietary carbohydrate. While Canadian Dietary Guidelines are distinct from the US ones, much of the research on which they are based is the same.
Comparing the US to Canadian dietary recommendations with respect to the consumption of fat in general, as well as the consumption of saturated fat in particular, one finds the recommendations mirror each other.
We are told to limit saturated fat ostensibly because of its negative impact on blood cholesterol and heart disease. We are told to increase consumption of vegetable oils, and to substitute polyunsaturated fats for saturated fat in cooking and baking and to eat 45-65% of our daily calories as carbohydrate.
It is increasingly my conviction that the simultaneous (1) marketing of polyunsaturated vegetable oil – more accurately called industrially-created seed oils, such as soybean oil and canola oil, along with (2) changes in the Dietary Recommendations in both Canada and the US for people to (a) limit calories from fat and especially to (b) limit saturated fat, combined with the recommendations for people to (c) eat 45-65% of calories as carbohydrate created the “perfect storm” that when viewed together, explains the obesity epidemic we now have and the associated increase in metabolic health problems that we now see 50 years later.
I will be writing more in the days ahead on what is thought to be the role of these industrially-created seed oils in the process of obesity and inflammation that underlies many metabolic conditions, including Type 2 Diabetes.
Why isn’t the public alarmed by this massive increase in obesity?
I believe it’s because it took place over such a long period of time that those old enough to remember what things were like before have either died or are approaching retirement age and have left its solution to the next generation, and those young enough to do something about it have never known it any other way.
I think that looking at the magnitude of the epidemic without the time frame is helpful.
What if only 10 years ago, only 1 in 10 people were obese and now 1 in 3 people were obese? Would there not be a public outcry for scientists to determine what caused this and to research to find a cure quickly?
Obesity underlies debilitating metabolic effects such as very high blood pressure that can lead to heart attacks and strokes and people of all ages are getting this disease – including children and teenagers. Obesity underlies the huge increase in Type 2 Diabetes and when poorly managed can result in blindness, limb amputation and organ failure. People of all ages are dying from these metabolic effects of these disease, which at present are mainly being managed through medication and advising people to “eat less and move more”.
Is that the best we can do to curb this epidemic?
As covered in previous articles, there are peer-reviewed published studies – some a year or two long, that demonstrate that these metabolic effects can be put into remission by eating a diet with less carbohydrates – yet government-funded research into use of this is not a priority.
Why?
What role does the sugar industry and the corn-producers (that manufacturer high fructose corn syrup found in much of our packaged food) play?
What role do the grain boards (that market wheat and other grains for baked goods) play?
What about the soybean and canola growers – multi-billion dollar a year industries in both countries that grows the soybeans and canola seed that are processed into fats sold to consumers for cooking and baking?
These industries and their respective lobby groups play an influential role in the economies of both Canada and the United States and in that way (and others) influence what types of research should be funded.
There is an epidemic going on and people are living with terrible metabolic consequences of them or dying from them.
Before the Dietary Guidelines are updated in both countries, the governments of Canada and the US must approve external, independent scientific review of the evidence-base for the existing dietary recommendation as well as examine the evidence-base for use of a well- designed low carbohydrate diet in reducing obesity and managing the debilitating metabolic effects.
The length of time since the obesity epidemic began does not make this any less urgent.
Do you have questions about how I can help you in tackling obesity and lowering or putting metabolic side effects into remission?
Please send me a note using the “Contact Me” form located on the tab above.
To our good health,
Joy
You can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
References
- OECD Health Statistics 2017, June 2017, http://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf
- Kearns C, Schmidt LA, Glantz SA, et al. Sugar Industry and Coronary Heart Disease Research: A Historical Analysis of Internal Industry Documents. JAMA Intern Med. 2016 Nov 01; 176(11):1680-1685.
- Husten, L, How Sweet: Sugar Industry Made Fat the Villain, Cardio|Brief, 2016 Sept 13.
- McGandy, RB, Hegsted DM, Stare,FJ. Dietary fats, carbohydrates and atherosclerotic vascular disease. New England Journal of Medicine. 1967 Aug 03; 277(5):242—47
- The National Diet-Heart Study Final Report.” Circulation, 1968; 37(3 suppl): I1-I26. Report of the Diet-Heart Review Panel of the National Heart Institute. Mass Field Trials and the Diet-Heart Question: Their Significance, Timeliness, Feasibility and Applicability. Dallas, Tex: American Heart Association; 1969, AHA Monograph no. 28.
- Introduction to the Dietary Goals for the United States — by Dr D.M. Hegsted. Professor of Nutrition, Harvard School of Public Health, Boston, MASS., page 17 of 130, https://naldc.nal.usda.gov/naldc/download.xhtml?id=1759572&content=PDF
Copyright ©2018 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.