NOTICE: This my personal experience as a private consumer of lab services, and is not related to my profession as a Dietitian. This article is posted in a separate section of the web page titled “A Dietitian’s Journey” which is about my personal health journeys.
“A Dietitian’s Journey – Part I” was about my two year journey recovering from obesity, and poor metabolic health and “A Dietitian’s Journey-Part II” is my current personal journey recovering from hypothyroidism.
This article is written as a private consumer, which is why it is categorized as a personal account, and an editorial.
 This past Monday, I went to the lab to have blood tests to measure my thyroid hormones, anti-thyroid antibodies, and an iron panel. When I had met with my doctor last week, I learned that I would need to pay for the free T3 test because the British Columbia guidelines and protocols for ordering thyroid tests state that a free T3 test is only covered to rule out suspected cases of hyperthyroidism [1]. As I wrote last Thursday, I was “more than willing to pay for a $9.35 test to have all the data.”
This past Monday, I went to the lab to have blood tests to measure my thyroid hormones, anti-thyroid antibodies, and an iron panel. When I had met with my doctor last week, I learned that I would need to pay for the free T3 test because the British Columbia guidelines and protocols for ordering thyroid tests state that a free T3 test is only covered to rule out suspected cases of hyperthyroidism [1]. As I wrote last Thursday, I was “more than willing to pay for a $9.35 test to have all the data.”
I think most people are aware that the healthcare system is economically stretched, and I certainly understand and accept the need to reduce costs. One way to do that is to restrict the ordering of laboratory tests to only medically justifiable circumstances, which makes good sense.
While I recognize that I am not objective in this situation, it would seem to me that when someone is on thyroid hormone replacement medication that includes both synthetic T4 and T3 hormones, that the expense of both a free T4 test and free T3 test should be covered by the provincial healthcare system as the cost is justifiable because the prescribing doctor needs to determine if the dosage of both synthetic hormones is adequate, but not too high.
As I said above, I knew last week that I would be paying for the free T3 test and was fine with that, but what I wasn’t prepared for was that I would be expected to pay three times the cost the government pays for the same test, and that there would no patient-price list available.
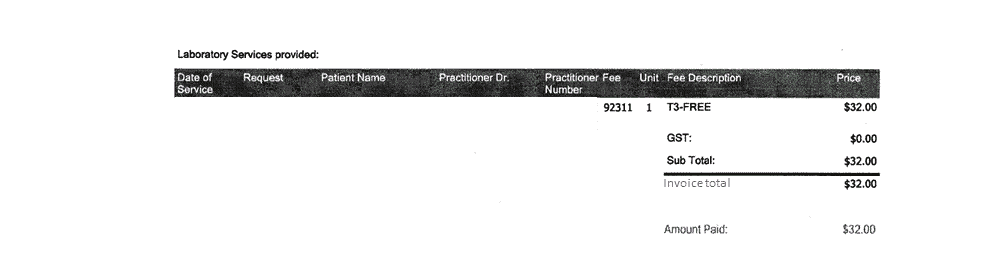
When I arrived at the lab on Monday, I was told that the free T3 test would cost $32.00. I replied that there must be a mistake, because the cost of the test is $9.35. I was informed that the government pays $9.35 for the free T3 test, but the patient-pay cost for the same test is $32.00. I explained to the person at the desk that I could understand the test costing more if there was a set-up fee for a stand-alone test, or for a separate blood draw, but this test was going to be run with others using the same blood draw. I was informed that $32.00 is the patient-pay cost of the free T3 test regardless of whether it is done with other tests, or by itself.
I asked if I could please see the price list with the patient-pay costs, and was told that there isn’t one. I was asked if I wanted to have the free T3 test period formed, and if I did that I would need to pay $32.00. What choice did I have? It was not as though I could go to one of the lab’s competitors, as this private lab company is the only one providing laboratory services in this city.
[NOTE (October 28, 2022: I have spoken to people in other provinces, and it appears from what people have said that the practice of diagnostic laboratories not disclosing patient-pay prices occurs in Manitoba, Ontario, and British Columbia. This practice may also occur in others provinces as well, but I don’t know. This article written as private consumer is about the practice of diagnostic labs not disclosing patient-pay prices to consumers, irrespective of which province the practice occurs in, or by what company.]
I paid the $32.00 for the test because I needed this information to know the effect of the medication on my thyroid hormones, and for my doctor to know whether a medication adjustment was needed. I had the disposable income to pay for it, but what about consumers who need a laboratory test to make health decisions or for their doctor to be able to, and who cannot afford that?
… and why are patient-pay clients charged 3 times as much as the government pays for the same test? Even if a private consumer was only requesting a stand-alone test and had to pay the ~$15 blood draw fee, this test would only cost $25, not $32.
After my appointment, I wrote the regional office of the lab company and asked “to have the patient-pay lab prices for British Columbia.” I heard back from a Client Service Advisor who told me that “We do not provide a list of what we charge to patients“.
I was flabbergasted.
I’ve always made the assumption that private businesses are required to post their prices, or at least make them available when asked.

As an individual consumer, what happened at the lab would be like going to the grocery store to buy food, but none of the items for sale have marked prices. You are required to pick out the things you need, but only find out at the cash register what the price is.
When you get to the cash, you ask the cashier about the prices, and she tells you there’s no price list, but she can give you the total cost at the end, and you can either pay, or put the items back. Needing the items, you pay what you are told, and take your receipt.
When you get home, you decide to write the head office and ask if they can send you a price list, and are told there IS one, but that they can’t give it to you.
[UPDATE October 29, 2022: The way things are currently set up, one has to make an appointment with the lab, go there, line up and give the person at the desk their requisition, and only then can find out how much the patient-pay part will cost.
After investing so much time, consumers are put in a position of having to make a decision on the spot — pay whatever is being asked, or leave without the test.
Consumers should be able to access the prices online and make a decision at their leisure, before investing so much time.]
I don’t know whether private businesses in Canada required to post their prices, or make them available when asked. I’ve always assumed they were, but I could be wrong. If there is a requirement to do so, do diagnostic labs have an exemption that enables them not to make their prices available to members of the public?
UPDATE October 28, 2022: I have since found out the same company provides a price list to allied health professionals so that they can provide laboratory assessment services to their clients, and if they choose they can mark up the cost in their own billing.
There are 2 versions of this test list available. They are identical except the one for British Columbia does not have the prices indicated, whereas the Ontario one does (see below).
I have also since found out that the company DOES have patient-pay price list that is titled “British Columbia Private Price List for Commonly Ordered Lab Tests” and is dated April 2021. It is marked “confidential” and as a result cannot be publicly shared. See #3, below.
-
-
-
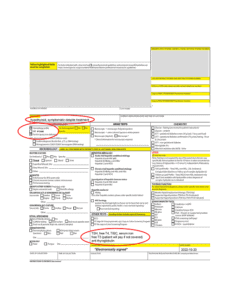
- The allied healthcare price list available in Ontario, dated November 2018 has the prices marked. I have removed the company’s identifying colours, logo, and information and posted their allied health professional test list here.
- The allied healthcare price list available in British Columbia, dated June 2020 does not have the prices marked. I have likewise removed the company’s identifying colours, logo and information and have posted their allied health professional test list here.
-
-

Above is the allied health professional cost (November 2018) for an entire thyroid panel of 6 thyroid-related lab tests, including;
-
-
-
-
- TSH
- free T4
- free T3
- reverse T3
- thyroperoxidase antibody (TPO)
- anti-thyroglobin antibody (TG-ab)
-
-
-
Compared to what the BC government pays for the same tests (minus the reverhttp://from http://www.bccss.org/bcaplm-site/Documents/Programs/laboratory_services_schedule_of_fees.pdfse T3 which isn’t paid for by MSP) the above panel costs $80. Presumably naturopaths are charged prices similar to what MSP pays.
3. I have since found out that there IS a patient-pay price list and it is titled “British Columbia Private Price List for Commonly Ordered Lab Tests” and is dated April 2021.

The prices cannot be posted because the notice at the top of the price list reads;
“This is a confidential document. Please do not disclose our prices publicly except in conversations with your patients.”
Why is the private-pay price of lab tests a confidential document, and why can’t the prices of lab tests be disclosed to the public?
Are business in British Columbia required to disclosed their prices and if so, are diagnostic labs exempt from making their private-pay prices available to consumers?
I don’t know.
How many people would be willing to order dinner at a restaurant that did not post the price of its menu items until after they ordered?
My Thoughts on Patient-Pay Prices
I believe that as consumers, private-pay individuals have a right to have access to the prices for laboratory tests in advance, so that they can consider their decision to purchase, or not purchase these services. Consumers expect grocery stores and department stores to post their prices, and it is my personal opinion that privately owned laboratories from whom private consumers purchase services should be no different.
I also think private-pay individuals have a right to know why they are required to pay a premium price for the same services that the government gets for a third the cost, and allied healthcare professionals obtain for approximately half the cost.
This differential pricing for allied health professionals is a little like retailers selling supplements to practitioners at wholesale prices, while expecting the consumer to pay full price. Even car dealerships have “employee pricing” events so that the average consumer can take advantage of the same discounts provided to their employees, but at these diagnostic labs, consumers are unable to know in advance how much they will be paying for services before they arrive at the cash.
I believe that as private businesses, diagnostic laboratories are free to set their prices as they see fit but it would seem that (1) consumers should be able to know what those prices are in advance, and (2) that consumers should also know that they are paying a premium price for the same services, compared to what the government and allied health professionals are paying.
I am very grateful to live in a country where publicly funded medical care is available. I am thankful to have access to excellent diagnostic lab tests, and don’t even mind paying the same cost the government pays for tests that I want to have done. But as a private consumer, I believe the cost of services need to be available and that there needs to be transparency with regards to pricing discounts provided to others.
To your good health,
Joy
References
- BC Guidelines & Protocols Advisory Committee, Thyroid Function Testing in the Diagnosis and Monitoring of Thyroid Function Disorder, October 24, 2018
Copyright ©2022 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.


 In 2018, both Dr. Jason Fung and the Diet Doctor website were promoting a low carb high fat (LCHF) diet of ~75% fat, 15% protein and 10% carbohydrate, but since that time, Dr. Fung has increasingly focussed on the role of regular intermittent- and long term fasting for weight loss and diabetes remission, while continuing to
In 2018, both Dr. Jason Fung and the Diet Doctor website were promoting a low carb high fat (LCHF) diet of ~75% fat, 15% protein and 10% carbohydrate, but since that time, Dr. Fung has increasingly focussed on the role of regular intermittent- and long term fasting for weight loss and diabetes remission, while continuing to 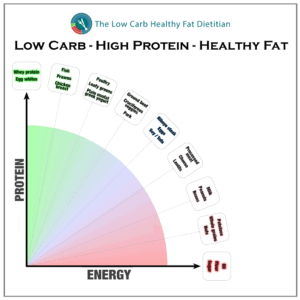 It has been my clinical experience since 2018 that a low carb higher protein diet is an excellent option for those seeking weight loss and remission of type 2 diabetes — especially those who do not do well on a very high fat diet, or for whom regular intermittent or extended fasting is not optimal due to the increased risk of sarcopenia (muscle loss).
It has been my clinical experience since 2018 that a low carb higher protein diet is an excellent option for those seeking weight loss and remission of type 2 diabetes — especially those who do not do well on a very high fat diet, or for whom regular intermittent or extended fasting is not optimal due to the increased risk of sarcopenia (muscle loss). 
 A hundred years ago, Dr. Russell M. Wilder and two Dietitians from the Mayo Clinic wrote a 69-page book titled “A Primer for Diabetic Patients – A Brief Outline of The Principles of Diabetic Treatment, Sample Menus and Food Tables[1]” which outlined the treatment of diabetes using different levels of a low carbohydrate and very low carbohydrate (ketogenic) diet, as well as short periods (12-48 hours) of fasting.
A hundred years ago, Dr. Russell M. Wilder and two Dietitians from the Mayo Clinic wrote a 69-page book titled “A Primer for Diabetic Patients – A Brief Outline of The Principles of Diabetic Treatment, Sample Menus and Food Tables[1]” which outlined the treatment of diabetes using different levels of a low carbohydrate and very low carbohydrate (ketogenic) diet, as well as short periods (12-48 hours) of fasting.
 “Insulin at that time cost five cents a unit in the market. However,
“Insulin at that time cost five cents a unit in the market. However,  In Wilder’s 1958 paper, he outlines how the
In Wilder’s 1958 paper, he outlines how the 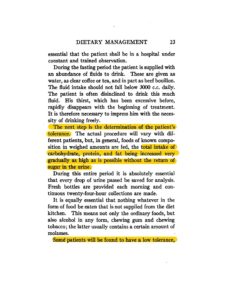 “The actual procedure will vary with different patients, but, in general, foods of known composition in weighted amounts are fed, the total intake of carbohydrate, protein and fat being increased very gradually as high as possible without the return of sugar in the urine.”
“The actual procedure will vary with different patients, but, in general, foods of known composition in weighted amounts are fed, the total intake of carbohydrate, protein and fat being increased very gradually as high as possible without the return of sugar in the urine.”

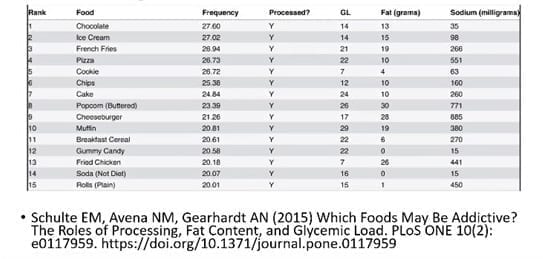
 We also know from a 2015 study on the effect of food order on the response of glucose and insulin, that
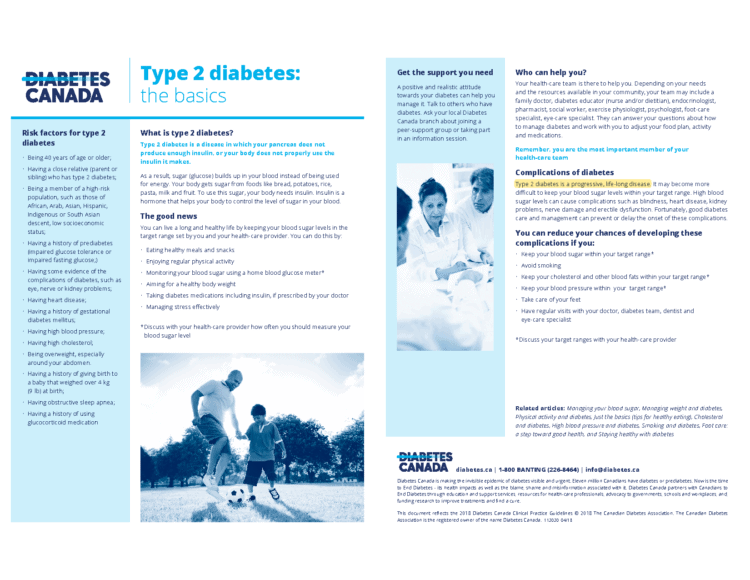
We also know from a 2015 study on the effect of food order on the response of glucose and insulin, that  The American Diabetes Association understands that a low carbohydrate diet ”limits sugar, cereals, pasta, bread, fruit & starchy vegetables” and “consist mostly of protein foods like meat and dairy, fatty foods like oil, nuts, seeds, avocado, and butter, and non-starchy vegetables” [2].
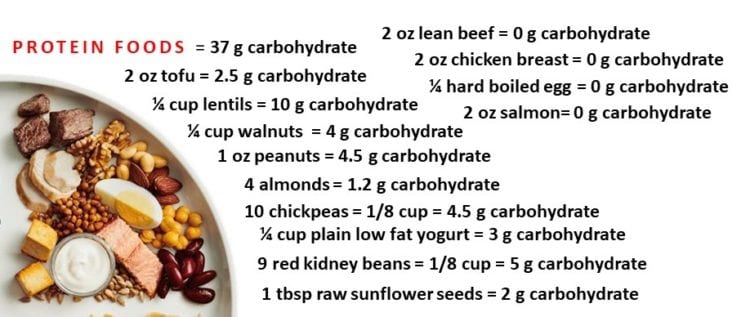
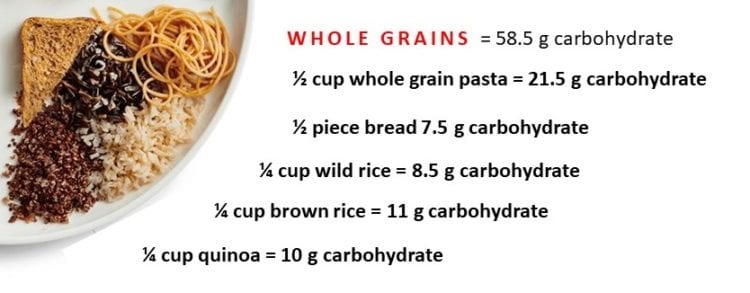
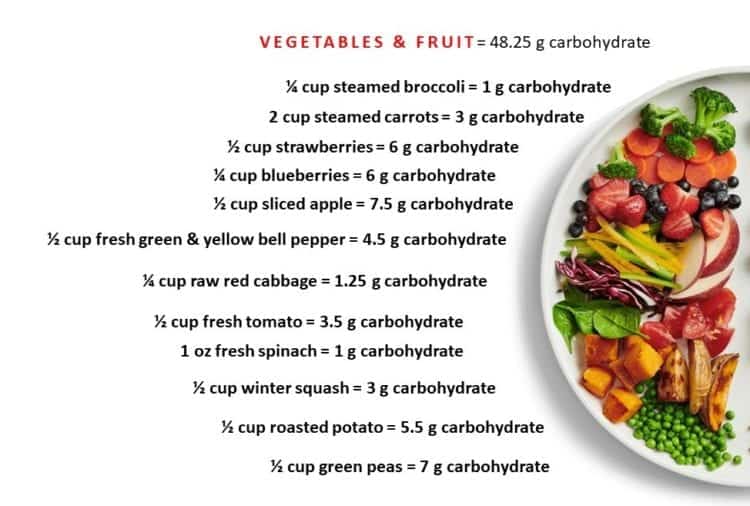
The American Diabetes Association understands that a low carbohydrate diet ”limits sugar, cereals, pasta, bread, fruit & starchy vegetables” and “consist mostly of protein foods like meat and dairy, fatty foods like oil, nuts, seeds, avocado, and butter, and non-starchy vegetables” [2].


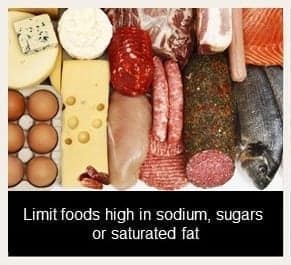
 The photo I posted is above.
The photo I posted is above.


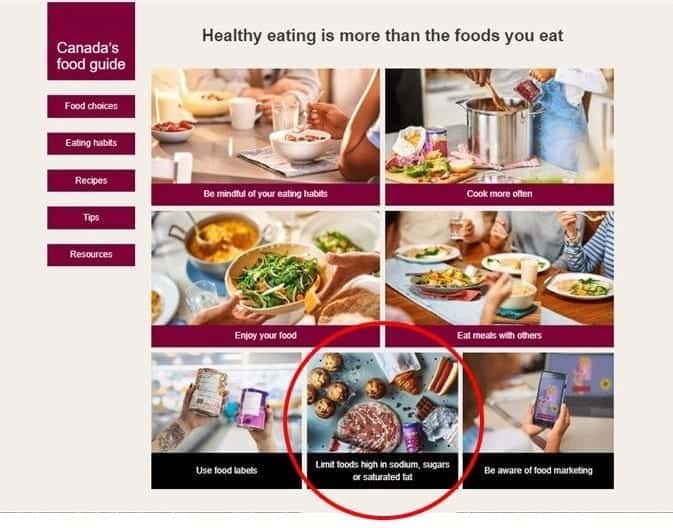
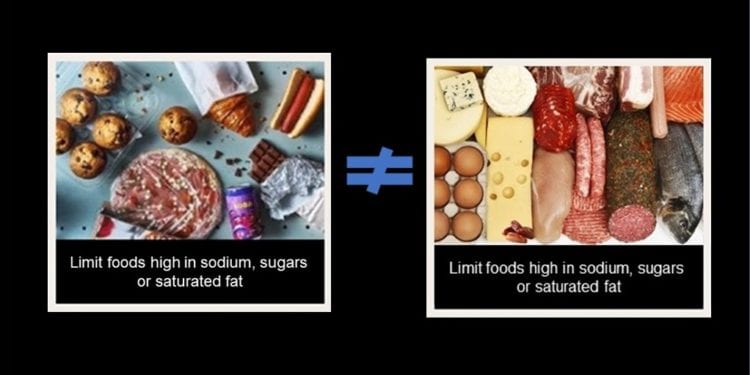
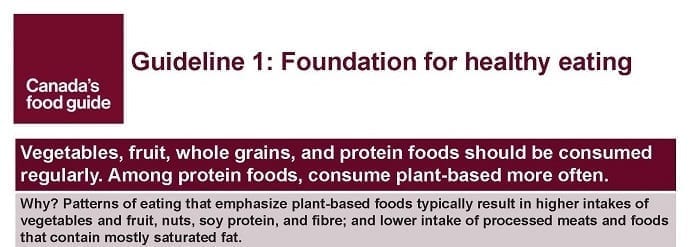
 In fact, when the image of these processed foods
In fact, when the image of these processed foods  In my opinion, it makes good sense for Health Canada to show a photo of ultra-processed foods as they had (above)with advice to limit them — but because they are ultra processed, not because they are high in saturated fat or sodium.
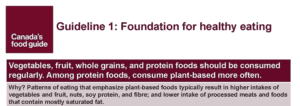
In my opinion, it makes good sense for Health Canada to show a photo of ultra-processed foods as they had (above)with advice to limit them — but because they are ultra processed, not because they are high in saturated fat or sodium. The main message of the “snapshot” is that “healthy eating is more than the foods you eat” â — which I think is an excellent way of summarizing the guidelines and recommendations and encouraging the public to want to learn more. From that point of view, the snapshot is successful in that it is likely to guide people to the website.
The main message of the “snapshot” is that “healthy eating is more than the foods you eat” â — which I think is an excellent way of summarizing the guidelines and recommendations and encouraging the public to want to learn more. From that point of view, the snapshot is successful in that it is likely to guide people to the website.