A month ago I made some changes in the macro distribution of protein to fat in my Meal Plan which has resulted in some significant progress in terms of weight loss, as well as inches lost.
Weight loss since increasing ratio of protein:fat
I knew that my weight had been decreasing about 1/2 pound a week over the previous several months, and in only the last month I had lost 7 pounds and an inch off my waist since I had increased my protein to fat ratio – that’s more than 1 1/2 pounds per week!
Over the long weekend, one of my sons took a cell phone picture of me when we were at Burrard Inlet, and he took a few to make at least one came out. This was a good thing because I would have thought that maybe it was just one photo or the camera angle that made me look slimmer. No, it wasn’t the camera angle, but the change in my weight over the last few months. It wasn’t until I saw a picture of what I looked like that I could ‘see’ it more objectively.
Here is the photo:
photo taken February 12 2018
When I got home, I remembered that in October I was out at the same location and had a photo from that day. That was 7 months into me following a low carb / ketogenic lifestyle.
I also had a photo of me from 2 1/2 years ago (taken around the time I first learned about the clinical benefits of following a low carb lifestyle) that was also taken in the same location.
Here are those three photos side by side:
Me on the left 2 1/2 years ago, 4 months ago in the middle, on the right now
I am not yet at my goal weight – which will be when my waist circumference is half my height, but I am well on my way. For me, changing the ratio of my ‘macros’ (short for ‘macronutrients’ i.e. protein, fat, carbohydrate) has helped overcome a slow and often stalled weight decrease.
Currently, what is working very well is for me is for me to plan my meals around getting sufficient protein and what is ‘sufficient’ is based on research regarding what older adults need to prevent sarcopenia (loss of muscle mass) as they age, as well as to continue to build muscle mass which helps improve insulin sensitivity.
Instead of focusing on how much and what types of fat are in my meals, I now set my attention around getting my individual need for 1.5 g protein / kg of ideal body weight. I eat the natural fat that is found in my protein source (skin on fatty fish or chicken, yolk in egg, etc.) but don’t ‘add’ much fat to my meals, except for maybe a little olive oil on salad. I eat the carbohydrates that come naturally in non-starchy vegetables and the nuts and seeds that I regularly eat, up to my carbohydrate maximum (or “carb ceiling”) for the day. For me, based on my significant degree of insulin resistance, this is working very well – but everyone is different.
My Meal Plan looks different than the Meal Plans I design for my clients because we all have different needs. Some people are overweight but insulin sensitive, others are normal body weight and insulin resistance and many already have Type 2 Diabetes (T2D). Even comparing my Meal Plan with those of my clients with T2D, mine is different because my ability to tolerate carbohydrate is very low. Think of the ability to tolerate carbohydrates for those who are insulin resistant like lactose intolerance to those who are lactose intolerant. Some people can drink some milk and be okay, whereas others are unable to tolerate even a small amount.
Something to keep in mind is that having a Meal Plan doesn’t mean it is ‘carved in stone’. Our physiological needs change as we lose weight and for those who are insulin resistant or T2D, as our level of insulin sensitivity improves over time which is why Meal Plans needs to be modified as weight loss progresses. As well, sometimes we benefit by a tweaking of the ‘macros’ (as I did with mine) to enable a more sustained and consistent weight loss.
Remember that everybody’s journey is different, because we all start from a different place.
As a result of the photo taken of me this past weekend, I have some thoughts about how we can use photos to chart our progress. While clinically, we measure our success in weight and inches lost and improved laboratory test results, often the way we as individuals can best recognize and celebrate our success is by seeing photos of ourselves over time. Don’t get me wrong, when I was obese I hated seeing photos of myself but now seeing them serves as a “sign post” of the progress I’ve made on my journey. Now, the very photos I detested I post on the internet for all to see, because I am now well on the road to much better health; with normal cholesterol and triglycerides, normal blood pressure and blood sugar levels that no longer meet the criteria for Type 2 Diabetes.
I certainly haven’t “arrived”, but today I take a moment to celebrate that progress, as I encourage my clients to do.
Have questions as to how I can help you achieve your health and nutrition goals? Please send me a note using the “Contact Me” form located on the tab, above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
As I’ve been saying from the beginning, my data is “a sample-set of one” (n=1), but yesterday data from 218 subjects that followed a low carb ketogenic diet for one year was published, so now I have something to compare my data with. Like the subjects in the study, when I began on March 5 2017, I was obese and had been diagnosed with Type 2 Diabetes more than a decade ago. The comparison between my results and those of subjects in this study is very encouraging!
Method Comparison
Carbohydrate Intake
Subjects in the study typically ate <30 g total dietary carbohydrates per day, whereas I ate 50 g of net carbohydrates per day which is approximately ~65 g of total carbohydrate per day for the first 5 months (more than double the amount of carbohydrate of those in the study). Most of these carbs came from berries and nuts.
It became clear through lab tests (fasting insulin along with fasting blood glucose) that I was quite insulin resistance and that level of carbohydrate intake was not providing me with the reduction in blood glucose I was seeking. It is only in the last 6 months that I lowered my carbohydrate intake to the level of those in the study and began to see significant progress.
Protein Intake
Subjects in the study had their protein intake targeted to a level of 1.5 / kg based on ideal body weight.
Until very recently, my protein intake was at 1.0 g / kg based on ideal body weight (which is at the minimum level of protein intake) and the bulk of my intake was from fat.
Vegetable Intake
Just as subjects in the study, I ate 3-5 servings of non-starchy vegetables per day.
My 11-month outcomes compared with 1-year data from the study
Blood Glucose Levels
At baseline, the average HbA1c level of participants in the study was 7.6% ±1.5%, with less than 20% of participants having a HbA1c level of <6.5% (with medication usage).
As I documented in my one-month update, I didn’t measure my HbA1C at baseline, but there are clinical calculators for estimating that from blood glucose levels. From laboratory tests, my fasting blood glucose the previous three years was 7.9 mmol/L (Feb 2013), 9.1 mmol/L (Sept 2014) and 9.7 (Aug 2015). Extrapolating that data to the start of my journey (March 5 2017) brought it to approximately 12 mmol/L. As documented in an earlier progress update, four months into eating low carb high fat, my fasting blood sugar was averaging 8.5 mmol/L.
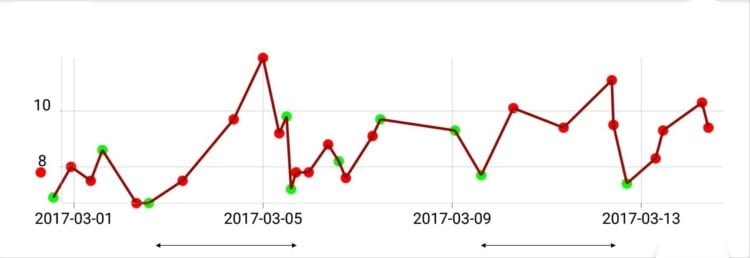
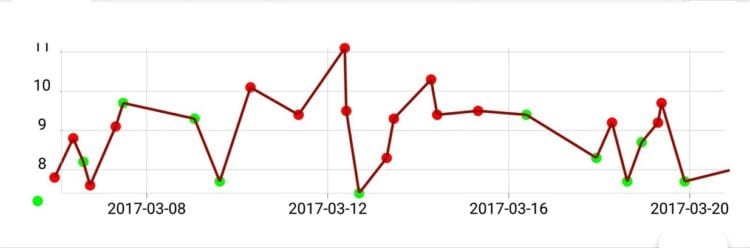
Here is a graph of my blood sugar levels the first few weeks;
My blood sugar levels a month after starting my journeyAs can be seen from the graph, my blood glucose was at lowest at 7.7 mmol/L (see photo to the left) and I had spikes well above 10 mmol/L, and I was averaging around 8.5 mmol/L over the course of the day – which is slightly higher than the average of those in the study.
On average after 1 year, participants in the study lowered HbA1c from 7.6% to 6.3% — which is in the sub-Diabetes range. A month ago, my laboratory HbA1C came back at 6.4% and in the last month, I am averaging 6.33%.
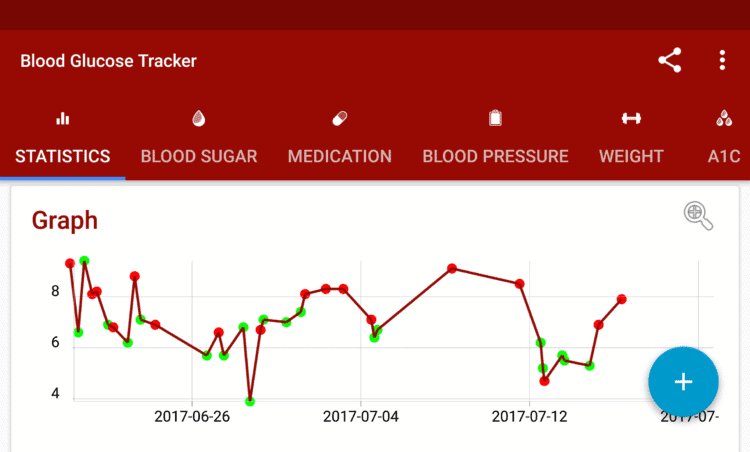
My average blood glucose readings the last two weeks
My highest ‘spikes’ are just above 7 mmol/L whereas at the beginning they were closer to 10 mmol/L.
Weight Loss
At one year, mean body mass reduction of participants in the study was 12% of their initial body weight, with an average of 30 pounds lost.
Average Weight Loss at One Year [from Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study.]At only 11 months, my body mass reduction has been 17% of of my initial body weight, with 35 lbs lost. Even eating a much higher fat diet for most of my journey and more carbs for the first 5 months, my weight loss so far has been better than the average of those in the study.
Other Metabolic Markers
At 10 months, participants in study experienced a 20% reduction in their triglycerides levels and after one year, reduction in triglycerides was at 24%. After one year, LDL increased on average by 10% however HDL increased on average by 18%.
My triglycerides dropped from .95 to .64 from the last time I had them checked in 2015 (with no change in diet until March 2017), which is a decrease of 33%, which is even better than the average 24% subjects in the study obtained. My LDL dropped from 3.26 to 2.60, which is a decrease of 20% – even better than the average of 18% from the new 1-year study data.
My HDL was previously good as I ate a liberal carb Mediterranean diet and not a standard American / Canadian diet, so it only rose 3% (from 1.91 to 1.97) from the last time I had it checked, however with the drop in my triglyceride levels, my TG:HDL ratio is now 0.32 (with <0.87 considered ideal).
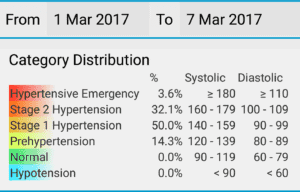
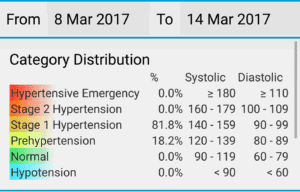
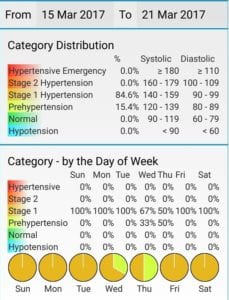
Eleven months ago, my blood pressure was 1/3 of the time in Stage 2 Hypertension with one hypertensive emergency (higher than Stage 3 hypertension!) with the rest of the time in Stage 1 hypertension. The last two weeks, my blood pressure is 50% of the time in the normal range for non-Diabetics to 50% pre-hypertension (which is considered the ‘normal range’ for those with Type 2 Diabetes) and I am off Ramipril. Except for stating that participants in the study had improvements in both systolic and diastolic blood pressure, no data was provided, so no comparison is possible.
Conclusion
Even eating almost double the amount of carbohydrates as those in the study ate for the first 5 months, my weight loss and improvements in blood glucose levels the last 6 months enabled me to match or exceed the results of those in the study!
On average after 1 year, participants in the study lowered their HbA1c from 7.6% to 6.3% and I lowered mine from 8.5% to 6.3% after 11 months.
Average weight loss in the study during the first year was 12% of body weight which on average was 30 pounds and my weight loss has been 17% of my body weight with a 35 pound weight loss, in 11 months.
My triglycerides decreased 33% which is even better than the average 24% in subjects in the 1 year study.
My LDL decreased 20% which was also better than the average of 18% from new 1-year study data.
My blood pressure was dangerously high 11 months ago and today is in the normal range for someone with Type 2 Diabetes and half the time is in the normal range for someone without it.
Finally here are two additional ways that I can measure my success to date;
Early this morning, my fasting blood glucose was 5.3 mmol/L (95 mg/dl) which is in the normal non-Diabetic range. This is a first! This was without taking Metformin.
At 10:20 AM while still fasting (today in an intermittent fast day for me), my fasting blood glucose is still 5.3 mmol/L (95 mg / dl) – also with no medication.
This is my body maintaining a stable non-diabetic fasting blood glucose level – which means my liver is not over-synthesizing new glucose (gluconeogenesis)
This is huge progress.
Up until now, my liver and muscle was so insulin resistant that my liver just kept making more and more glucose (via a process called gluconeogenesis).
Normally, the hormone insulin stops excess glucose production by stopping glucagon secretion by the pancreas (alpha cells), but I was SO insulin resistant, glucagon would be released telling my liver to make more glucose!
The fact that my fasting blood sugar has been stable for so many hours, means my liver is starting to respond to signals correctly. My liver is maintaining my blood sugar at a normal level – without any medication. This is great news.
UPDATE: My morning fasting blood glucose the following morning was just as wonderful (5.3 mmol/L / 95 mg/dl), Feb 9) and my 2 hour post prandial blood glucose after eating a high protein low carb breakfast was also amazing (5.4 mmol/L / 97 mg/dl, Feb 9). That is, the above result was not a ‘one-off’ event but the start of becoming insulin sensitive!
Finally, here are two photos of me; one from March 2017 and one from February 2018 – taken 10 months apart. Using the width of my glasses as a reference, it is easy to see the decrease in the width of my face.
Goals compared with results
March 14, 2017, I set very specific goals that I wanted to achieve and they were;
I have a long way to go to get to my goals (plural) because I’ve set the bar very high…and why not? If the literature indicates that this works, then I want;
(1) blood sugar in the non-diabetic range
(2) normal blood pressure
(3) normal / ideal cholesterol levels
(4) a waist circumference in the ”at or below” recommended values of the Heart and Stroke Foundation
Will I meet all these goals? Who knows?! But I won’t know if I don’t try and the alternative of a life of medication for blood sugar, blood pressure and eventually cholesterol too does not appeal to me!
So join me in my journey — a journey of change, of good health and on a road less traveled.
It is 11 months later this is what I have achieved;
My HbA1C is below the Diabetic range and I am much of the time, I am able to maintain my fasting blood sugar in a normal, non-Diabetic range.
My blood pressure is in the normal range for someone with Type 2 Diabetes and half the time it is in the normal range for someone without it.
I have normal / ideal HDL cholesterol and triglyceride levels and my LDL is in the normal, but not ideal range.
I have a waist circumference that is ”at or below” recommended values of the Heart and Stroke Foundation (see photo , above).
A waist circumference in the ”at or below” recommended values of the Heart and Stroke Foundation for a Caucasian woman is < 35 inches
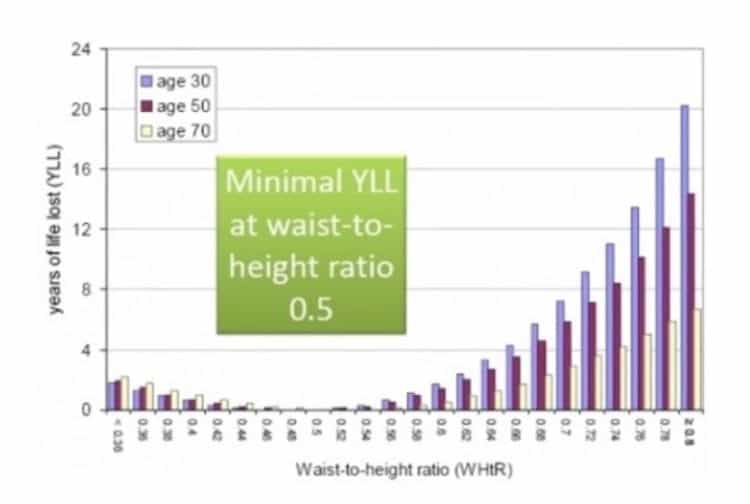
Three weeks after setting the above goals, I updated my waist circumference goal to be that I wanted my waist circumference to be half my height. This was based on a meta-analysis study from 2012 which pooled data from multiple studies with more than 300, 000 adults in several ethnic groups and which found that Waist to Height Ratio (WHTR) was a far better predictor than BMI or Waist Circumference of cardiovascular or metabolic risk factors in both sexes.
from Ashwell M, Gunn P, Gibson S (2012) Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev 13: 275—286
How to take Waist to Height ratio: Measure your waist at the location that is the mid-point between your last rib and the top of your hip bone, with the front and back of a flexible seamstress-type tape measure at the same height, and your belly fully relaxed, not sucked it in! Your waist circumference in inches should be half your height in inches.
Based on having a low-risk waist to height measurement, I still have to lose another 2- 1/2 inches off my waist. I haven’t yet “arrived” but I am certainly making progress in my own, personal health and weight loss journey.
Comparing my own results over the last 11 months to the 1 year data of over 200 adults with Type 2 Diabetes who were eating a low carb ketogenic diet, I am doing at least as well, and in some cases, better. This is reason for me to be encouraged.
NOTE: There is no “one-size-fits-all” low carb / ketogenic diet and what works for me may not be what is best for you. Before undertaking a major change in diet, please discuss your plans with your doctor.
Have questions?
Wonder how a low carb / ketogenic lifestyle can help?
Please send me a note using the ”Contact Me” form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Hallberg, S.J., McKenzie, A.L., Williams, P.T. et al. Diabetes Ther (2018). Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. https://doi.org/10.1007/s13300-018-0373-9
NOTE: A “Dietitian’s Journey” is my “sample set of one” (n=1) personal story. My results following a low carb / ketogenic lifestyle are just that; my results. There is published scientific evidence of physicians discontinuing patient’s medication following adoption of a low carb / ketogenic diet, but this post should not be viewed as objective data. This is simply me documenting my own, personal journey. Do not discontinue any medication without first consulting with your doctor.
Three years before I adopted a low carb lifestyle, I was diagnosed by the head of Immunology and Allergy at a Canadian university with a relatively rare immunological condition known as Mast Cell Activation Disorder / Syndrome (MCAD / MCAS). I had numerous debilitating symptoms that are not unlike those that accompany other immunological / autoimmune disorders such as Lupis, Rheumatoid Arthritis (RA) and fibromyalgia – plus a few unique to MCAD (such as food and environmental sensitivities and pronounced flushing). According to the Immunologist, the MCAD was likely triggered from my exposure to toxic mould exposed in a basement repair in November 2012. I was prescribed a whole host of medications in order to manage many debilitating symptoms.
In April of 2013, my Immunologist prescribed two types of antihistamines (H1 and H2) in very large quantities, including Cetirizine HCL 10 mg (H1) 4 times a day and Ranitidine 150 mg (H2) three-four times per day in an effort to lower my body’s release of inflammatory products. The dosage of Cetirizine is 4 times the amount used for treating seasonal allergies and the dosage of Ranitidine was twice the dosage typically used for treating acid reflux. These medications were in addition to two tablets of diphenhydramine hydrochloride 25 mg (Benedryl) that I took every 4 hoursfour times per day. It’s amazing I could function at all, taking that much Benedryl, but I had no choice. I also needed to use a Salbutamol (asthma) inhaler four times per day to manage my environmental sensitivity to various odors, including laundry soap and the smell of certain foods.
In November 2013, the Immunologist prescribed Sodium Nalcrom 100 mg, a mast cell stabilizer in an effort to reduce and eventually discontinue taking all the Benedryl. I took 2 capsules of Nalcrom before each meal three times per day and 2 capsules at bedtime – a total of 8 capsules per day.
Sleep disruption is one of the inconvenient symptoms of MCAD, so I was prescribed Trazadone 100 mg before bed to assist with that.
I took all of these medications as prescribed above until shortly after I began eating a low carb diet in March of 2017.
Within 3 months of beginning to eat a low carb diet (~50 gm carbohydrate per day), I was able to take less and less Nalcrom – first dropping it in the morning, then at lunch time, but continuing to take it at supper and occasionally before bed.
After about 6 months eating low carb (still ~50 gm carbohydrate per day), I was able to reduce the Cetirizine to three times per day from four and was also able to reduce the Ranitidine from 3-4 times a day to twice a day. I stopped taking the Nalcrom completely. With the MCAD much better, I was able to lower my Trazadone for sleep to half.
Once I reduced my carbs further, down to 35 gm per day (in order to better manage continued high glucose readings), I was able to reduce the Cetirizine to twice a day and the Ranitidine to just once per day, at night (which at that point was more to manage GERD than for any symptoms of MCAD). I continued to take the Trazadone ~ 3 times per week as needed for sleep.
It’s been about 3 months since I stopped taking the Ceterizine completely and about a month since I stopped taking the Ranitidine. This left me with the “baby dose” of Ramipril 2.5 mg that I asked for in July 2017, as my blood pressure had begun to creep back up. When I saw my doctor in December, we discussed when I should discontinue the Ramipril, to which he said “when your blood pressure gets too low”. I asked him to give me a number, so I could continue to monitor it. He said, when it goes below 110 / 65 then you can discontinue it.
my blood pressure readings last night
Two days ago I felt a little light headed but didn’t stop to think it might be my blood pressure. I drank more water and carried on. Yesterday late in the afternoon (when my blood pressure is usually the highest) it was 119/79. I continued to monitor it in the evening, and it continued to drop to 112/63, 109/59, 100/59 and then back up to 108/60. Based on my doctor’s instructions to me, it seemed it may be time for me to discontinue the Ramipril. Last night I didn’t take it, but this morning I took 1/2 of it as I want to make discontinuing it gradual. I will take a 1/2 dose for a few days and keep monitoring my blood pressure to make sure my body is adapting to maintaining my blood pressure without medication
This morning as I anticipate putting the Ramipril container in the pile of discontinued medication that I have on a shelf in my closet, I realized just how big that pile is!
Pile of discontinued medication (excluding the Benedryl which was discontinued before I began eating low carb)
I am not “cured” of MCAD, or of my Type 2 Diabetes, or my hypertension (high blood pressure) or GERD, or my abnormal lipids (referred to in my 11 month update). I am reasonably certain that if I began eating a high carb diet again, all, if not most of the symptoms I experienced previously would resume. I am in remission from these conditions and likely will remain in remission, provided I continue to eat low carb and continue to lose weight (until I achieve a low-risk waist to height ratio). The discontinuation of my past medications serve as “sign-posts” of my journey.
If you would like to know how I can help you on your own health and nutrition journey, please send me a note using the ”Contact Me” form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
My journey began on March 5, 2017 when I was a fat Dietitian with all the benchmark symptoms of Metabolic Syndrome including Type 2 Diabetes, high blood pressure, high LDL cholesterol and triglycerides, abdominal adiposity (i.e. “a belly”) and high BMI (high weight for height). Physically I was a mess but my biggest problem was that I was in denial. It had been months since I had monitored my own blood sugar or blood pressure even though I had been diagnosed with Type 2 Diabetes 10 years earlier. I knew better.
I would occasionally step on the scale and weigh myself, but how my clothes fit (or didn’t) already told the story. I was overweight. Actually, I was obese.
Shortly before my own turning point in March 2017, I had two girlfriends my own age – one who I knew since high school and one since university die of preventable diet-related disease within two months of each other. Both were in healthcare and took care of others practicing their profession, just as I do. I had two degrees on the wall but didn’t take care of myself.
March 5, 2017 all that changed. That was the day that the pain of remaining the same became greater than the pain of changing. So I changed. That story and the progress since then are in previous articles in A Dietitian’s Journey.
Like many others, I once believed that “Diabetes is a chronic, progressive, disease” and that it will only get worse in time. I realize now that if I had continued to eat more carbs than my body could handle, then it most certainly would have gotten worse but I have almost 11 month of evidence that supports that if I don’t, it CAN and DOES get better.
I am not “cured” by any means, but my symptoms are now in what the American Diabetes Association defines as partial remission and I may very well be able to achieve full remission, as I continue to eat a low carb diet. I will only know in time.
To achieve remission with Type 2 Diabetes (T2D) is like someone being in remission with Celiac disease; we can get well and stay well provided that we don’t eat the foods that we can’t tolerate; for a Celiac that’s gluten and for someone with T2D it is more carbohydrates than their body can handle.
I do eat some carbohydrate each day, mostly as non-starchy vegetables, the occasional berries or pomegranate seeds on a salad, as well as some nuts and seeds but I am careful to keep the amount at any one time below what my body can process while maintain blood glucose control as close to a ‘normal’ (non-Diabetic) level as possible.
This article explains how and why my body is no longer able to handle more than a small amount of carbohydrate at a time.
The good news is that I no longer meet the criteria for diagnosis with Type 2 Diabetes, as demonstrated by the Diagnostic Criteria[1] for the disease:
It does not appear that Diabetes Canada define these concepts, however the American Diabetes Association (ADA) defines “remission” as having test results below the range for Diabetes (i.e. Fasting Blood Glucose less than or equal to 5.5 mmol/L (100 mg/dL) without taking Diabetes medications or having bariatric surgery.
“Partial remission” according to the ADA is having test results lower than the range for Diabetes i.e. Fasting Blood Glucose less than or equal to 5.5 – 6.9 mmol/L (100—125 mg/dL) or HbA1C between 5.7 — 6.4% for at least 1 year.
my Fasting Blood Glucose is less than or equal to 7.0 mmol/L , so I no longer meet the diagnostic criteria and fall in the partial remission range. As you can see from the following picture, the average of my twenty-four Fasting Blood Glucose readings from January 1 2018 – January 24, 2018 has been 6.0 mmol/L. Out of the 24 glucometer readings (with a meter that I standardized with the lab when I had my tests done), only once was my blood sugar higher than the cutoff. This would indicate that I am in partial remission, by the ADA definition.
Self monitored blood glucose – January 1 2018 – January 24, 2018 – averages
I have taken seventy-five glucometer readings during the month of January so far (see photos at the bottom of this article) and none of them were greater than or equal to 11.1 mmol/L. Here is a graph of my January results:
Self monitored blood glucose – January 1 2018 – January 24, 2018 – graph
3. My 3 month glycated hemoglobin test, also known as a HbA1C (or “A1C” for short) is less than or equal to 6.5 % which means that I no longer meet the criteria for the disease and my results fall in the range for partial remission.
Glycated Hemoglobin below criteria for Type 2 Diabetes – January 23, 2018
Cholesterol and Lipids
My LDL was at the high-end cutoff two years ago, after only 4 months on a low carb high healthy fat diet, it was approaching what is considered by the existing / popular standards of ”optimal LDL” for someone who is high risk (family history of cardiovascular disease).
My LDL was 2.60 mmol/L (1.14 mg/dl), my triglycerides (TG) were 0.64 mmol/L and my HDL was 1.97 mmol/L.
Using more significant measures, my TG:HDL ratio was 0.32 (with <0.87 considered ideal). A very low TG:HDL ratio is associated with lots of large, fluffy LDL — the kind associated the lowest risk of cardiovascular disease (CVD) such as heart attack and stroke. It is the higher density, small LDL particles that are associated with CVD.
Blood Pressure
My blood pressure has been ranging from between just below the normal range to pre-hypertension for months, but to protect my kidneys I am continuing to take a ”baby dose” of Ramipril® (2.5 mg per day) that I asked the doctor to put me on until my blood pressure is consistently below normal and the meds need to be reduced or discontinued. The dose I’m on is the smallest it comes in and my doctor has switched me to tablets, which can be split if my blood pressure is consistently on the low side.
Weight and Waist Circumference
Weight
I’ve lost 35 pounds. I feel better about how I look than I have in many years, and I am a little more than half way there. I am celebrating my progress, but not letting it be ‘enough’ because health-wise, it isn’t. To truly reduce my risk of heart attack and stroke, I need to lose another 25 pounds, or whatever weight will actually put my waist circumference at half my height.
Waist Circumference
I’ve loss 7 inches off my waist. That’s more than 1/2 a foot! Crazy, eh? I only have another 3 inches to lose off my waist for me be in the low-risk category and I am guessing that will correlate to another 30 pounds of weight loss. Maybe it will be less, maybe more, but my weight loss goal is whatever it takes for my waist to be half my height. The scale won’t determine my goal, the tape measure will.
My hard earned success in achieving partial remission from Type 2 Diabetes and these significant improvements in metabolic markers would be very short-lived if I began to eat more carbohydrates than my body can handle. I am still learning how much of which kinds of foods I can eat while maintaining my blood glucose levels but my own “n=1 results” seems to indicate that full remission of Type 2 Diabetes may very well be possible. The literature seems to support that it is possible- but whether I can achieve that level has yet to be seen. I still have much more to achieve, but I am definitely on the road to better health!
If you would like to know how I can help you on your own health and nutrition journey, please send me a note using the “Contact Me” form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
P.S. For those that would like to see the “numbers” to understand my progress to date, below are 10 photographs showing all my glucometer readings since March 5, 2017 until today.
Blood Glucose Mar 5 2017 – January 24 2018 – pg 1
Blood Glucose Mar 5 2017 – January 24 2018 – pg 2
Blood Glucose Mar 5 2017 – January 24 2018 – pg 3Blood Glucose Mar 5 2017 – January 24 2018 – pg 4Blood Glucose Mar 5 2017 – January 24 2018 – pg 5
Blood Glucose Mar 5 2017 – January 24 2018 – pg 6
Blood Glucose Mar 5 2017 – January 24 2018 – pg 7Blood Glucose Mar 5 2017 – January 24 2018 – pg 8Blood Glucose Mar 5 2017 – January 24 2018 – pg 9Blood Glucose Mar 5 2017 – January 24 2018 – pg 10
References
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212, Chapter 3
Ten months ago, it was urgent. I had to make a choice between going on several types of medication to lower my crazy-high blood pressure, and high blood sugars, triglyceride and LDL cholesterol or to immediately change my lifestyle. I chose to change my lifestyle. This is a progress report, going into the final two months of my first year at this.
As with other changes we undertake, there are two ways to look at things; how far we’ve come or how far we have to go. I choose to look at my progress as both. I am certainly not “there” yet, but I am nowhere near where I was!
Back in early March of this year, when I faced my own personal health crisis, it had been two years since I had any lab work done and ages since I was monitoring my blood sugar myself, even though I was Diabetic for the previous 10 years. It really was a case of classic denial. I didn’t want to know how bad it was. That day because I didn’t feel well, I faced the truth. I took my blood pressure (multiple times, because I couldn’t believe the readings!!) and I took my blood sugar. My blood pressure was so high, for certain had I gone to see my doctor at that point, he would have prescribed at least one type of medication, maybe two. Suffice to say it was dangerously high.
My blood sugar back in March of this year was high, but what else could it be eating a carb-based diet. I had started eating low carb two years earlier, but life circumstances got in the way for a time and I failed to go back and pick up where I left off. As I could have predicted they would, things only got worse. My fasting blood sugar was between 13.0 mmol/L (234 mg/dl) and 9.0 mmol/L (162 mg/dl). That’s nuts!
I was obese (BMI > 30). I’d joke about being the “fat Dietitian” but it wasn’t funny. For the previous two years, I was teaching others to eat low carb high healthy fat in order to lower their weight and reduce their insulin resistance, but I was in classic denial when it came to myself. Yes, I knew I was fat, but I was in denial as to just how much risk I was at for a heart attack or stroke.
My LDL was high and even though my high HDL acted as a protective factor, in the context of me being Diabetic, obese and having very high blood pressure, the only place it was going to go was higher – unless I changed my lifestyle permanently. That day I did. For me, there really can’t be any turning back as it really is a matter of life and death. I am no longer in denial.
So how am I doing?
The weight has been coming off, slowly but surely. I haven’t made any major progress in the last month, but then again I didn’t gain anything of significance over the holidays. That’s a good thing. Okay, it’s a very good thing. Looking at it with the ‘glass’ being half empty I am still only 1/2 way to where I need to be to have my waist circumference 1/2 my height. Looking at it with the ‘glass’ being half-full, I’ve lost 30 pounds. I feel better about how I look than I have in many years, and I am only half way there. I am celebrating my progress, but not letting it be enough because health-wise, it isn’t. To truly reduce my risk of heart attack and stroke, I need to lose another 30 pounds, or whatever weight will actually put my waist circumference at half my height.
I’ve loss 6 inches off my waist. That’s 1/2 a foot! Crazy, eh? I only have another 4 inches to lose off my waist for me be in the low-risk category and I am guessing that will correlate to another 30 pounds of weight loss. Maybe it will be less, maybe more, but my weight loss goal is whatever it takes for my waist to be half my height. The scale won’t determine my goal, the tape measure will.
My blood pressure has been ranging from between just below the normal range to pre-hypertension for months, but to protect my kidneys I am continuing to take a “baby dose” of Ramipril® (2.5 mg per day) that I asked the doctor to put me on until my blood pressure is consistently below normal and the meds need to be reduced or discontinued. The dose I’m on is the smallest it comes in and my doctor has switched me to tablets, which can be split if my blood pressure is consistently on the low side.
As covered in an earlier update, my triglycerides and cholesterol are now in the ideal range simply from the dietary changes I have made.
My blood sugar has been a bit frustrating, because overall it isn’t going down nearly as fast as I thought it would, or as I’ve observed other people’s to do. Everybody’s different and mine is just taking this long despite all the things I am doing right. I started out eating “low carb” (50 gm carbohydrate per day) and as it turned out it wasn’t low carb enough, perhaps because of how long I’d been Diabetic and just how insulin resistant I really am. A few months ago, I added regular intermittent fasting (IF) – fasting 23 hours from the end of supper to the beginning of supper the following day (drinking ‘bone broth’ and tea and other appropriate beverages while fasting). I have done one slightly longer fast, with careful monitoring. Along with IF, a number of months ago I also lowered my carb intake to ≤ 35 gm of carbs per day and monitor my blood sugar 5-7 times per day to make sure it doesn’t dip too low. During the day time, towards the end of a 24 hour fast, my blood sugar will be in the low 4’s mmol/L (~81 mg/dl) just before I eat again, but in the morning, the lowest it has ever been is 5.8 mmol/L (105 mg/dl). No matter what I do the night before (i.e. exercise, eat very low carb) my blood sugar begins rising around 3 am and continues rising until 6 or 8 am, even though I am fasting. It is classic “dawn phenomenon” and it has been incredibly frustrating.
My HbA1C has dropped from ~9.0 % (at the beginning of March) to 7.5 % (July 25 2017) to 7.0 % (October 11 2017) in 7 months, but for the last 3 months it has remained stubbornly at 6.8 % – almost exclusively because my fasting blood sugarremains high. This led me to a decision to ask my doctor to trial me on a “baby dose” of Metformin® only at night to see if it will help bring down my fasting blood sugar and more importantly, the corresponding insulin resistance, while I continue to eat a very low carb (ketogenic) diet and practice intermittent fasting.
After reviewing the over 400 glucose readings I took from March 5, 2017 onward and seeing that my HbA1C remains only slightly lower the last 3 months despite all my lifestyle changes, my doctor agreed to trial me on the lowest dosage of Metformin® over the next 3 months (the dose given to youth with high blood sugar). It will be interesting to see its effect as of January 6, 2018. What many people may not realize is that while Metformin® is now a pharmaceutical (medication), it was initially derived from a plant called “goat’s rue” or the French lilac and has been used since the Middle Ages to treat the symptoms of Diabetes. It’s not unlike acetylsalicylic acid (ASA), which is the active compound in Aspirin® which was originally isolated from white willow bark. Aspirin® and Metformin® are both natural in origin.
In addition to its natural origins and long-standing safety record, studies indicate that people with Diabetes who take Metformin® have lower incidence of cancer and dementia and in animal models, increased longevity has also been reported. Given all of these factors, it seemed reasonable for me to ask my doctor to trial me on a small dose of Metformin® to see if it keeps my liver from manufacturing too much glucose in the early hours of the morning, thus lowering my overall insulin resistance, while I continue to eat ketogenically and practice intermittent fasting. My doctor agreed. While it is too soon to know how much impact this small dose will have, from January 6th until today, my blood sugar is averaging 6.5 mmol/L, yet still rising from 3 am until 6 am. I will give it a few more weeks and then possibly ask my doctor to try me on the same dosage of slow-release Metformin®, to see if my morning blood sugar is improved.
It may seem strange to some that I would add medication after successfully having lost so much weight, having brought my lipids into the ideal range for non-Diabetics, and having lowered my blood sugar to the ideal range for Diabetics (≤ 7.0%) solely by adopting a low carb lifestyle and practicing intermittent fasting. I view much it like wearing a brace or using a cane after injuring one’s knee. It’s not a permanent measure, but support and protection while the healing continues to take place.
This is my journey, and my progress and challenges are as individual as I am. Everyone is different and the degree of carb reduction and whether or not intermittent fasting may be helpful for you is something that will only be known it time as we work together. One thing is for certain is that unless one starts the process of working towards achieving their health and wellness goals, things will not improve on their own.
Have questions?
Please send me a note using the “Contact Me” form located on the tab above.
The photo on the left is what I looked like when I started my weight-loss and health ‘journey’ on March 16, 2017, 9 months ago. The photo on the right, is me today.
Based on my BMI, I was well into the Class I Obesity category 9 months ago. Based on my BMI today, I am just 15 pounds from my weight falling in the normal range.
At the beginning of March, my blood pressure ranged between Stage 2 Hypertension and Stage 1 Hypertension — sometimes being dangerously high. Now, my blood pressure hovers around 125/80 mmHg mark, and I am still on the ‘baby-dose’ of Ramipril for now, as it protects my kidneys.
My triglycerides and my LDL cholesterol (”bad cholesterol”) were high, certainly well above what it should have been for someone who has Type 2 Diabetes and had family risk factors. Thankfully, my HDL was good, offering some protection.
In the past 9 months, my morning fasting blood sugar has dropped from ±12 mmol/L (216 mg/dl) to anywhere from 5.8 mmol/L (105 mg/dl) to 6.5 mmol/L (117 mg/dl) – with the occasional 8.0 mmol/L (144 mg/dl) for seemingly no apparent dietary reason. For my fasting blood sugar to be in the non-diabetic range, it needs to be consistently below 5.5 mmol/L (99 mg/dl).
When I began this journey, my HbA1C was ~ 9.5% and during the last 30 days, I am averaging ~6.3% which is in the non-diabetic range. This has been entirely achieved without any medication to lower blood glucose.
I was determined to reverse the symptoms of Diabetes, high cholesterol and high blood pressure by changing how I ate and by introducing short periods of intermittent fasting and I have certainly made significant progress.
Weight and Body Measurements
I’ve lost ~25 lbs so far, but the changes in my body and face shape are even more noticeable, as evidenced by the photo above.
So far, I’ve lost;
1″³ off my upper arms
3″³ off my neck (!)
1″³ off my thighs
4 1/2″³ off my waist
This week, I reached the “goal weight” that I initially set for myself, but in order to attain an ideal waist circumference that is 1/2 my height, I probably have to lose another 20-25 pounds, which means I am half-way there.
I am entirely convinced that this is realistic and attainable.
Change only happens when the pain of staying the same is greater than the pain of changing.
Want to start your own weight loss and health journey? Why not send me a note using the “Contact Us” form above.
Wishing you and yours all the best for holiday season!
Note: I am a “sample-set of 1” – meaning my results may or may not be like anybody else’s that follows a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
It’s been 7 months since I’ve been seriously adhering to a low carb high heathy fat (LCHF) lifestyle, but like anybody else it’s easy for me to get frustrated when I don’t reach goals as quickly as I would like. I have to stop and remind myself that I didn’t become obese and Diabetic overnight and it’s going to take time to reverse these symptoms. These updates help me take stock of my progress, because after all it’s about progress, not perfection.
Joy – class 2 obesity
At my highest weight, my Body Mass Index (BMI) put me well into the Class 2 Obesity category. I felt terrible, looked terrible and was desperately unhealthy. Losing weight seemed impossible – or if not impossible, too difficult.
September 20 2015
This is what I looked like 2 1/2 years ago, when I first heard about following a low carb high healthy fat lifestyle from a retired physician-friend. At this point, I had already lost about 25 pounds by cutting portion sizes and exercising, but my weight was always fluctuating by 10 or 12 pounds and with it, my blood sugar, cholesterol and blood pressure. I was in denial about how very unwell I had become.
The sudden death of two girlfriends my own age was certainly a ‘wake up call’, but it was my blood pressure that had become dangerously high that was the final impetus for me to change. I knew that if I did nothing, I was at very high risk of having a stroke or heart attack. My choice was (1) to go on medication for high blood sugar, high cholesterol and high blood pressure or (b) change the way I ate. It was, as they say, a “no brainer”.
March 5, 2017 was the day I made the decision to change and there has been no looking back.
Change only happens when the pain of staying the same is greater than the pain of changing.
March 16 2017 – the beginning of the journey
This is what I looked like when I started. Based on my BMI, I was well into the Class I Obesity category.
My blood pressure ranged between Stage 2 Hypertension and Stage 1 Hypertension – dangerously high.
My morning fasting blood sugar was averaging ± 12 mmol/L (216 mg/dl) and my HbA1C was likely ~ 9.5%.
My triglycerides were high and my LDL cholesterol (“bad cholesterol”) was well above what it should have been for someone who was Type 2 Diabetic and had family risk factors.
I was determined to reverse the symptoms of Diabetes, high triglycerides and high blood pressure by changing how I ate.
Progress, not perfection
Blood Glucose
When I began this journey at the beginning of March, my fasting blood glucose was averaging 12 mmol/L . My HbA1C was likely ~9.5%. Four months into eating low carb high fat, my fasting blood sugar was averaging 8.5 mmol/L and my HbA1C was 7.5% – still above the ≤ 7.0% therapeutic target for those with Type 2 Diabetes.
This week, 3 months later, my HbA1C reached the ≤7.0% therapeutic target for those with Type 2 Diabetes, but that is still not good enough. My goal is to get it at or below 6.0 % – below the Diabetic cutoff range. My challenge remains that my blood sugar is frequently high in the morning when I am fasted, yet is significantly lower in the late afternoon when I have been intermittent fasting for the same length of time. I continue to suspect that cortisol remains a factor as cortisol production naturally begins to climb around midnight and reaches and is highest level between 6 am to 8 am.
This higher blood sugar in the morning is something called “Dawn Phenomenon” which I had for a good 5 years before becoming Type 2 Diabetic. When I track my blood sugar from 10 pm until 8 am, it starts going up in the wee hours of the morning and keep rising until 6:30 or 7 am so it’s evident that my fasting blood sugar is rising with the daily fluctuations in cortisol. When I am intermittent fasting for the same amount of time during the day, my fasting blood glucose is always < 5.0 mmol/L and many times less than 4.0 mmol/L – which is usually my signal to eat something. Under the effect of cortisol combined with my liver still being insulin resistant, the glucose has no where to go and just sits in my blood.
I am going to try to get back to incorporating some form of daily activity to lower stress, which kind of fell off the radar and add some short duration, high-strength / high muscle-use exercise such as squats which can help move blood glucose into the muscle.
Blood Pressure
I continue on my low very low dose of Ramipril (Altace) and my blood pressure is averaging 127/74 mmHg. When I stop the meds for a day or two to measure my blood pressure, it is still averaging 145/82 mmHg which is still too high to discontinue the medication, but it is far better than the 160/90 mmHg that it was 3 months ago.
Weight and Body Measurements
LEFT: March 16 2017, RIGHT: October 11 2017
I’ve lost 20 lbs so far but its the change in my body and face shape that is most noticible!
In terms of “inches”, I’ve lost;
1″ off my upper arms
2.5″ off my neck (which really shows!)
1″ off my thighs
4 1/2″ off my waist (which feels amazing!)
Facial lines are more visible, but when I look in the mirror I actually recognize the face looking back.
I am now below the high end of the overweight category based on BMI and am continuing to lose weight steadily.
At the beginning of this journey, I planned to lose ~30 lbs, but I realize that to attain an ideal waist circumference that is 1/2 my height, I likely have another 30 pounds to lose now which means I am not quite half-way there, but I am making progress!
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
I am not one for popular remedies for health issues. I don’t believe in “cleanses” and I don’t “eat clean” – or do I? If not eating any dairy is “clean” then I eat “dirty” because I use cream in my coffee, but if not eating gluten or grains is “clean”, then my eating is pristine.
The problem with popular beliefs around food and eating and word-of-mouth remedies is there is no standardized means to define them or evaluate their effectiveness.
Folk Remedies
Folk remedies, on the other hand, are in a different category. These practices, on which many nutraceuticals and even pharmaceuticals are based have GRAS standing (“Generally Recognized As Safe”) and have been used by cultures around the world for hundreds, if not thousands of years.
Here’s are two examples of folk-remedies in this category;
Swallow’s Nest
The Chinese have made soup out of the nest of a particular swallow which builds its home on high cliffs. This “bird’s nest soup” is highly prized and very expensive to make, but considered to have restorative properties for those with breathing difficulties. As it turns out, this particular swallow’s nest is high in theophilline, a compound that has come to be used in Western medicine as therapy for respiratory diseases such as chronic obstructive pulmonary disease (COPD) and asthma. Bird’s nest from this swallow has a GRAS standing and can legally be purchased in traditional Chinese medicine stores. One can take medication or food containing the same active substance, and in both cases one’s symptoms improve.
Bitter Melon
Bitter melon or bitter gourd / karela is widely grown in Asia, Africa and the Caribbean – both for food (prized for its bitter taste) and for its medicinal properties. In both Ayurveda, the traditional medicine (Hindu) of India and in Traditional Chinese Medicine (TCM) different parts of the bitter melon plant are brewed as a beverage and taken as a treatment for Diabetes. As it turns out, bitter melon, which has GRAS standing, contains polypeptide-p which is an insulin analogue.
Apple Cider Vinegar
I’ve been hearing about the use of apple cider vinegar (ACV) since I first started reading about low carb high fat diets in early 2015, from Dr. Jason Fung, a nephrologist (kidney specialist) from Toronto. He recommended that 1 Tbsp. of unpasteurized ACV be taken in a glass of water prior to meals and that it be add it to broths, soups and marinades. He’d said that it inactivates the production of digestive enzymes and slows down the rate of digestion, stabilizing blood sugar levels. Since the recommendation to use ACV at the time did not come with any scientific evidence, I summarily dismissed the idea of using it.
Persistently High Fasting Blood Glucose
For those who have been following my own progress following a Low Carb High Fat style of eating over the past 6 months (posted on the tab “A Dietitian’s Journey”) you know that despite losing weight, significantly lowering both my triglycerides and LDL cholesterol and my overall blood sugar levels coming down significantly, I had two ongoing problems;
(1) my morning fasting blood glucose (FBG) remained high, and
(2) my blood glucose would only drop into the 5-point-something mmol/ L range (~94 mg/dl) or to the 4-point-something mmol/ L range (76 mg/dl) range after an entire day of intermittent fasting.
Since there are physiological risks associated with high blood glucose, I was very motivated to find out why they were high in the morning and to do something about them.
I decided to keep detailed food records for 3 weeks to see if there was a patter, and ruled out diet.
Then, I decided to take my blood sugar several times each night, from midnight until 8 am, over several days, to see when it rose. As it turned out, it would drop nicely after supper (as it would after eating at any other time of the day), to 7-point-something mmol/l (~130 mg/dl) after an hour or so, and then to 6-point-something mmol/L (121 mg/dl) around midnight, and then it would gradually begin to rise from ~2 am, reaching its highest point around 8 am, following the circadian rhythm of cortisol.
Since it seemed that my high morning blood sugar was due to cortisol rising after went to bed until 8 am, and since cortisol can be affected by many things including stress, I took up going for a walk after supper. It did help! My morning blood sugars were in the mid-6-point-something mmol/L (~117 mg/dl), which was a far-cry from the 8.0 mmol/L (144 mg/dl) level it had been!
The evening walks, however, were short lived due to a shift in the winds and the raging forest fires in and around the Lower Mainland which caused the skies to fill with Fine Particulate Matter, know as PM2.5 (as the are 2.5 micrometers or less, in size). Since these can enter the lungs and the blood stream resulting in ill-effects, my walks stopped. In fact, if I did have to go out, it was with a vented N-95 mask. The smoke briefly cleared being replaced by stifling heat in the mid- to high-30 Celsius (100 F) for 10 days, followed by more smoke, so I began to look for something- anything that might lower my morning blood sugars, which at this point were hovering in the 7.6 mmol/L mmol/L (137 mg/dl) range!
At first I tried doing a short workout on my Nordic-track or using my “step” before bed, but it didn’t do much for my blood sugars and made me far too awake to fall asleep.
Having some unpasteurized, unfiltered ACV in the house, I decided to try it. It tasted terrible!! I tried adding it to water and it was still awful! I couldn’t bring myself to drink it!!
From Masking the Taste to Food as Medicine
A few years ago, in an effort to drink more water each day, I began drinking Club Soda / Selzer and then purchased a Sodastream machine, to carbonate my own (filtered) water.
I usually drink it plain, but have been known to put a twist of fresh lemon or lime in it.
ACV Ginger-aid
I tried adding 1 Tbsp of unpasteurized ACV to 1 litre (quart) of carbonated water but I still couldn’t drink it! All I tasted was sour!
Needing to mask the taste, I decided to grate a bit of fresh ginger root into it and “ACV Gingeraid” was born!
The first time, I drank a litre (~ quart) of “ACV Gingeraid” mid-morning, and my blood sugar dropped from 7.3 mmol/L (132 mg/dl) to 6.6 mmol/L (119 mg/dl) in an hour. I thought to myself that maybe it would have dropped the same amount if I had done nothing.
I hadn’t had anything to eat or drink (except a coffee with only cream in the morning) but presumably under the effect of cortisol and my body’s own making of glucose from fat stores, my blood sugar continued to rise from 6.6 mmol/L (119 mg/dl) at 5:30 AM, to 7.7 mmol/L (139 mg/dl) just before 10 AM.
That was just too high – and I hadn’t eaten!
So, I made and drank a second bottle of ACV Ginger-aid and in 1.5 hrs, my blood sugar had dropped to 6.3 mmol/L (114 mg/dl). Then by 4:00 PM, and drinking no additional ACV Ginger-aid, it was 4.8 mmol/L (86 mg/dl).
I would previously only get to those kinds of numbers just before dinner, when I was on an intermittent fast day. This was 2-2.5 hours earlier.
That couldn’t be, I thought…
Several days in a row, the same thing would happen, with only slightly different numbers, some of them lower.
My blood sugar would be around 7.3 mmol/L (137 mg/dl) 2 hours after dinner and I would drink most of a bottle of ACV Ginger-aid before bed, and in the morning my FBG would be in the 6’s mmol/L (~119 mg/dl). Could it be because of the drink?
One day, quite by chance, I had some fresh turmeric root in the house (because I use it in cooking and because I like the taste). As well, is a potent antioxidant and the curcumin (the active compound in turmeric) has been demonstrated to have anti-carcinogenic properties).
I decided to add a little bit of grated turmeric root because I thought the turmeric would taste good with the ginger (it did!).
I also added a bit of freshly ground black pepper to the Turmeric-ACV Ginger-aid, because I had read that black pepper makes the curcumin in the fresh turmeric root 2000 times more bio-available.
Turmeric ACV Ginger-aid
The drink tasted delicious!
But what happened to my blood sugars was quite surprising.
It became evident that for me, using “food as medicine” has had some very impressive results!
Just 3 days earlier, I was impressed because by 4:00 PM my blood glucose was 4.8 mmol/L (86 mg/dl) – which was a good 2.5 hours earlier than usual.
Since adding the turmeric to the ACV Ginger-aid, I was getting numbers in the mid-4 mmol/L (i.e. 4.6 mmol/L / 84 mg/dl) by 2:30 in the afternoon!
By drinking the Turmeric-ACV Ginger-aid before bed, my morning FBG is consistently in the low 6’s mmol/L (~110 mg/dl) and on a few occasions, ”ve been getting numbers in the high-5s mmol/L (103 mg/dl). I was considering Metformin to get these kinds of results!
This is by consuming ordinary food found in my kitchen!
I continue to eat LCHF and I usually intermittent fast breakfast, as I’ve never been much of a “breakfast person”. I occasionally don’t eat until mid-day as that is when I usually first feel hungry.
My blood sugars are the best they’ve been since I started measuring them.
Now, 2 hours after meals my blood sugar is usually in the low 6’s mmol/l (~110 mg/dl) and the ONLY change has been adding this beverage before bed and occasionally one plain ACV Ginger-aid through the day.
Just to be a ‘good scientist’, last night I deliberately ate 1/2 a dark chocolate bar (72% cocoa) and drank 3/4 of a bottle of plain AVC Ginger-aid (no turmeric) and tested my blood glucose this morning. It was 6.6 mmol/L (119 mg/dl). That’s crazy! I was expecting 10 or 11 mmol/L. That’s what it used to be just a few weeks ago, when I’d eat a little bit of dark chocolate!
NOTE: I wanted to see what would happen if I ate the same way but discontinued the beverage. My blood sugar went up to 8.8 mmol/L the first morning after not having any the previous day and was 8.6 mmol/L the following morning. The third day, I drank only one bottle in the afternoon and on at night before bed and the following morning, my fbg was 7.2 mmol/L (still way too high, but much lower). I anticipate it will continue to drop as I have 2-3 bottles of the mixture per day.
Even thought I am NOT exercising (first because of the smokey conditions outside and because I fell back into old “bad-habits” of getting up early and working at my desk with my coffee), my blood glucose is what I would have anticipated would have occurred if I had taken Metformin.
Keep in mind, I am “a sample-set of one”. There’s no saying that others will have the same, or even similar results. In addition, I do NOT encourage people to make any changes in the amount of medication that a doctor prescribed without being told by that doctor. This drink is NOT a substitute for medication that has been prescribed! That being said, for those who are not taking medication but have persistently high blood sugar readings does it not make good sense to consider trying such food as medicine?
NOTE: I decided to find out if there was any scientific evidence for the anti-glycemic properties of ACV and did find a 2015 study, suggesting that it increases insulin-stimulated glucose uptake in those with Type 2 Diabetes (T2D), which I have. I then decided to look and see if ginger had anti-glycemic properties and found a 2015 study that reported that ginger significantly reduced FBG as well as HbA1c, along with Apo B, Apo B/Apo A-I, MDA and increased the level of Apo A-I in T2D patients. Naturally, I looked to see if turmeric was known to have anti-glycemic properties and sure enough, it did! I found a 2013 publication that indicated it is well-known that turmeric has a stimulatory action on pancreatic β-cells, and that this may be the mechanism by which it lowers blood sugar in those with T2D. Whether these substances used together have a far greater effect on blood sugar than any of them used separately would certainly make for an interesting study!
WARNING: Given the possibility of these ordinary foods resulting in a dramatic drop in blood sugar, if you have Type 2 Diabetes or pre-diabetes, first discuss incorporating these foods into your diet with your doctor. As well, be sure to monitor your high blood sugar often if you drink these.
ACV Gingeraid Recipe
Click on the link under “Recipes” for ACV Gingeraid with Variations – food as medicine. Enjoy!
Mitrou P, Petsiou E, Papakonstantinou E, et al. Vinegar Consumption Increases Insulin-Stimulated Glucose Uptake by the Forearm Muscle in Humans with Type 2 Diabetes. Journal of Diabetes Research. 2015;2015:175204. doi:10.1155/2015/175204.
Khandouzi N, Shidfar F, Rajab A, Rahideh T, Hosseini P, Mir Taheri M. The Effects of Ginger on Fasting Blood Sugar, Hemoglobin A1c, Apolipoprotein B, Apolipoprotein A-I and Malondialdehyde in Type 2 Diabetic Patients. Iranian Journal of Pharmaceutical Research”¯: IJPR. 2015;14(1):131-140.
Zhang D, Fu M, Gao S-H, Liu J-L. Curcumin and Diabetes: A Systematic Review. Evidence-based Complementary and Alternative Medicine”¯: eCAM. 2013;2013:636053. doi:10.1155/2013/636053.
Note: Everyone's results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody's nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Finally! Like anyone else who’s been working long and hard towards achieving their health goals, I’m so excited that I’ve finally made a significant ‘breakthrough’! I didn’t think it would take this long, but when I think that it has taken me close to 20 years to become this insulin resistant, it only makes sense that it is going to take some time to become insulin sensitive again!
Last night, for the first time since I was diagnosed with Type 2 Diabetes (T2D) ten years ago, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl).
To put that in context for someone without Diabetes, blood glucose taken two hours after meals should be less than 7.8 mmol/L (140 mg/dl) – so my blood sugar after supper was not only in the non-Diabetic range, it was much better than that!
This means that the delaying the time between meals that I have been doing each weekday is starting to have its effect.
‘Hearing’ for the first time
When insulin was released after I ate dinner last night, my cells responded to insulin’s signal and took up the glucose from my blood, into my cells! This is what is supposed to happen, but from years and years of eating a diet that had far to many carbs (mostly as “healthy” fruit and milk), my cells had become non-responsive to insulin’s signal. The glucose (the blood sugar produced after food is digested) would stay at high levels in my blood because even though sufficient insulin was being produced and released by the βeta-cells of my pancreas, my cells had become insensitive to its signal. My cells had become insulin resistant – they were ‘deaf’ to insulin’s signal.
Last night, for the first time that I’ve observed, my cells responded to insulin properly! Like a hearing-impaired person hearing for the first time, my cells could ‘hear’!
Still “hearing-impaired”
My cells aren’t yet ‘healed’. They and my liver are still insulin resistant which is evidenced by the fact that even though I haven’t eaten anything since dinner last night, my blood glucose is high.
As it is supposed to do in response to both a low-carb diet and intermittent fasting, my body is breaking down my fat stores for energy (lipolysis) and the free fatty acids that are released are being used to produce glucose for my blood (in a process called gluconeogenesis) and ketones for my other organs, including my brain.
My blood glucose should increase from the gluconeogenesis, but it shouldn’t stay high!
In a perfect world, my blood glucose should be maintained around 4.0 mmol/L (72 mg/dl) when I am intermittent fasting, but it is much higher than that. The VERY good news is, it is falling to these ideal levels earlier and earlier each day, as I continue to intermittently fast Monday to Friday.
Intermittent Fasting – the missing ‘key’
It used to be late in the afternoon before my blood glucose would finally fall to 3.9 – 4.2 mmol/L, but over the six days it has been falling to these levels earlier and earlier each day.
blood glucose readings July 25 – August 23, 2017
Last Thursday, while checking my blood glucose every 2 hours, it dropped to 3.2 mmol/L at 1:55 PM and I immediately ate some carb-containing food, but the next day, late in the afternoon it only reached 4.8 mmol/L at 4:00 PM, despite me delaying the time between meals, both days. As someone with Type 2 Diabetes, I have to monitor my blood sugars every few hours when I am delaying meals, to be sure my blood sugar is being maintained by my body breaking down fat.
Monday, my blood glucose was 3.7 mmol/L (67 mg/dl) at 4:00 PM and yes, I ate something immediately.
Tuesday it was 4.6 mmol/L (83 mg/dl) at 2:30 PM
Today (Wednesday) it was 4.5 mmol/L (81 mg/dl) at noon!
Best of all was that last night, 2 hours after eating, my blood glucose was only 5.8 mmol/L (105 mg/dl) – not just ‘normal’, but well below the non-Diabetic cutoffs! This is what I have been waiting for!
Tracking Ketosis
Ketones (also called ‘ketone bodies’) are naturally occurring molecules (acetoacetate, βeta-hydroxybutyrate, and their spontaneous breakdown product, acetone) that are produced for energy while people are sleeping, or when they haven’t eaten for a while. Ketone production is natural and normal and occurs to everyone – otherwise we would need to get up at night to eat!
Ketones are picked up the body’s tissues and converted into something called ‘acetyl-CoA’ which then enters the citric acid cycle and is burned in the cell’s mitochondria (the ‘powerhouse’ of each cell) for energy. When we are sleeping, or are eating low-carb high health fat or simply not eating for a while, this is what our body uses as fuel instead of glucose. When eating low carb over an extended period of time, the body makes the little bit of glucose it needs for our brain and blood from fat and uses ketones for the rest.
A Ketostix® urine test strip (from several weeks ago)
Ketones can be easily and inexpensively detected in urine using a test strip, such as Ketostix®.
When people are at a low level of ketosis, they produce both acetoacetate and βeta-hydroxybutyrate in approximately equal quantities. These ketones are used by the muscle cells for energy. Ketostix® only measures the amount of acetoacetate in the urine.
For those that choose to eat very low carb and remain in ketosis for a while, their body’s will take the acetoacetate and convert it to βeta-hydroxybutyrate. Since Ketostix® only measures acetoacetate, the strips may become lighter and lighter because there is less acetoacetate in then urine. This is when blood ketone strips becomes helpful.
Abbott Laboratories® produce a small serum monitoring system that can test either blood glucose levels or serum β-ketone levels, using different test strips. The glucose strips cost about the same as glucose test strips used with other glucometers, but the β-ketone test strips are quite costly, costing between $3-$5 each, depending on where they are purchased. I don’t use them very often – only to make sure I don’t let my ketones get too high.
Note: I take a rather conservative approach to low carb eating and don't see any need to lower carbs to such a point as people are producing large amounts of ketones. I encourage insulin-resistant clients who are eating low carb to monitor both their blood sugar and ketone production often and to discuss their results with their doctors.
The β-ketone test strips measure the amount of βeta-hydroxybutyrate in the blood.
β-Ketone test strip, measures βeta-hydroxybutyrate in blood sample
This morning, about an hour after I measured my fasting blood glucose at 7.8 mmol/L, I measured my fasting β-ketones (which measures the amount of βeta-hyroxybuterate in my blood) at 1.6 mmol/L.
A low level of serum βeta-hyroxybuterate is considered 0.34 mmol/L and a mid-range level of serum βeta-hyroxybuterate is considered 2.36 mmol/L, so I was in the low-mid range level, which is the highest level that I go. I am also monitoring my blood sugar every two hours to make sure that my blood sugar level is being maintained adequately.
Note: as they say on TV “don’t try this at home”. Be sure to discuss following a low carb diet with your doctor first and also discuss whether there are any health reasons to avoid remaining in mild ketosis for any period of time.
At these levels, my body is happily breaking down my own fat stores for energy and the free fatty acids that are being released are being used to produce glucose for my blood (via gluconeogenesis). This is evident by my blood glucose being 7.8 mmol/L around 9:30 AM today.
This morning’s workout ‘selfie’
My body produces ketones (as evident by my βeta-hyroxybuterate being 1.6 mmol/L) an hour later and these ketones are being picked up my body’s tissues and are being converted into acetyl-CoA, which is being burned by my cells mitochondria for energy. These ketones not only fuel my brain, so I can work, they also fuel my body so I can exercise.
Yes! I aim to do some kind of exercise for 30-45 minutes most days.
This is the BIG difference between “starving” and “fasting”. I’m fat-adapted and I have plenty of fat stores to burn, so my body is really quite happy burning my own fat stores for energy while maintaining my blood sugar using the carbs in my diet and the glucose synthesized from my fat.
‘Getting moving’ and occasionally ‘breaking a sweat’
When I speak of ‘exercise’, it’s not crazy intense, but it is my getting my body ‘moving’.
All my morning walks (with and without Nordic poles) – from the very first one 5 1/2 months ago, have been done fasting.
Yesterday I did 15 minutes of aerobic exercise and 30 minutes of lower body resistance training – not in a gym, but at home. I was fasting…and continued to fast until late in the afternoon. Remember, my body is breaking down my fat stores for energy and I have plenty of those!
all the “gym” I need!
I’m not a member of a gym.
I have a corner of one room set up with my Nordic Track ski-machine, a few free-weights (2#, 5#, 10# and for the future 20#), a floor mat, 3 levels of resistance bands, and a “step”.
If I use my Nordic Track, I listen to music while I work out, and have a water bottle with homemade club soda (seltzer) close at hand. I have a Sodastream® machine, so I always have a steady supply.
I am using the “step” or doing aerobics of some kind, I use some videos I found on You-Tube of a TV show I used to exercise to years ago. I always liked them because they gave lots of instructions so that only one muscle group at a time is being worked. That way, only one part of my body needs to recover, and I can work other parts the following day.
If I am doing my free weights, I follow the routine I learned from a kinesiologist friend, when I took off the first part of the weight 5 years ago.
I keep it simple and simply make part of every day doing something that requires me to ‘get moving’ and 3 times a week I aim to make that activity something that ‘breaks a sweat’.
I don’t exercise to ‘lose weight’ – I’m active because it’s part of a healthy lifestyle. It’s good for my heart, for reducing stress and to increase muscle tone – and it makes me feel terrific.
Sure, I still have a long way to go but a each week and each month passes, I am closer to my goal that I was the week or month before. I am certainly closer than had I never started!
Here’s some more proof…
These three photos were taken on this date (August 23) in 2015, shortly after I had heard about low carb high fat eating from a retired physician-friend, last year in 2016 and today 2017. While there isn’t a huge difference weight-wise between last year and this year (14 pounds), the difference one can’t see is becoming evident.
Me – August 23 2015, 2016 and today 2017
Yes, the progress it is painfully slow and it would be easy to get discouraged except that I have read the studies and seen the results that other clinicians have obtained with their patients. It’s twenty-five weeks since I started – just about 1/2 a year, but my hard work and determination to ‘stick with it’ is paying off. Last night, for the first time since I was diagnosed as having Type 2 Diabetes, my cells provided evidence that they are beginning to respond to the signals from insulin the way they are supposed to.
This afternoon, they did it all again!
This was my blood glucose 3 hours after lunch (which I decided to eat today, because I felt hungry). As mentioned above, 4.5 mmol/L (81 mg/dl) is well below the ‘normal’, non-Diabetic post prandial glucose level of 7.8 mmol/L (140 mg/dl)
This was even better than after dinner, yesterday!
It took longer than I expect, but it’s happening!
So, one day at a time, one week at time, the weeks add up to months and the months to half a year and in half a year, I have measurable progress!
Oh, did I forget to mention that my weight is down again? I am seeing “numbers” I haven’t seen since I gave birth to my children!
Slow, yes – but very sure.
Now let’s see what I’ll accomplish in the second half of this year!
Have questions?
Want to know how I can help you accomplish your health goals? Why not send me a note using the “Contact Us” form above.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
For the last 2 weeks, the Lower Mainland has been covered in smoke due to hundreds of wildfires in the area. The very poor air quality had made going for a walk impossible.
Everywhere I went, I needed to wear an N95 mask to filter out the particulate matter and with the excessive heat and reddish-yellow skies, I had no desire to be out any longer than I needed to.
Over the weekend, cool marine finally air arrived and the air cleared for the first time in weeks. Finally it didn’t look like I was living on Tatooine.
When I woke up yesterday, the first thing I wanted to do was go for a morning walk. I walked 3 km around the local track and today I went again and decided to make a short video. When I went to upload it, I noticed how very different my face looked than from my first walk, 5 months ago (March 16 2017).
LEFT: March 16, 2017 | RIGHT: August 15 2017
I’ve only lost 13 pounds in the last 5 months since I began eating Low Carb High Healthy Fat, but the difference in how I look and how I feel is quite evident. As I’ve covered in previous “A Dietitian’s Journey” blogs, my blood work has certainly reflected the change.
I don’t really do any exercise outside of walking and even then, I only started doing it regularly 7 weeks ago (June 22, 2017) and not for the last 2 weeks (due to the air quality advisory). Five weeks of walking has helped me tone my muscles a bit and lower my overall blood sugar, but not had any significant impact my weight loss. While for the last 8 weeks, I’ve delayed the start of my first meal (intermittent fasting) which has impacted my fasting blood sugar, it hasn’t really impacted my weight, as I consume the same amount of protein, fat and carbs per day, just over a shorter period.
My weight loss has really only been accomplished by doing what I have been teaching my professional clients to do over the last 2 years; eating low carb and high healthy fat. I was tired of being the “fat Dietitian”! Now I’m now “practicing what I preach”.
Is it hard? Not at all! This has to be the easiest way to eat and requires little, if no culinary skill. Sure, one can get pretty creative making all kinds of exciting ethnic foods if they know how to cook, but it is certainly not required!
The difference in how I feel is truly all the motivation to keep doing it! Losing weight is a bonus.
Want to know how I can help you achieve your own health and nutrition goals? Why not send me a note using the “Contact Us” form above.
Note: I am a "sample-set of 1" - meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating "low carb" and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
For the last two weeks, I have been living on Tatooine. Not really, but it certainly has felt like that – with smoky, red sunrises and sunsets, inhospitable heat and high levels of ground-level ozone. British Columbia, where I live, remains under a state of emergency as 148 wildfires continue to burn across the province, with this being BC’s worst fire season in almost sixty years. As a result, the air quality in many communities, including mine, has deteriorated to dangerous levels.
This is what the sunrise has looked like from my backyard the last two weeks:
There have been high concentrations of fine particulate matter known as PM2.5 in the air, which are solid or liquid droplets with a diameter of ≤2.5µm (micrometres). Due to their small size, these particles easily penetrate indoors, even when windows are closed and are small enough to pass from the lungs into thebloodstream –putting people withlung or heart disease, Diabetes or asthma at risk.
In addition to the smoky air, temperatures each day have been in the low- to mid-thirties Celcius (90-95 degrees Fahrenheit) which is highly unusual. Here in the Greater Vancouver area, we’ll get a few days in a row like that once or twice each summer, but not for two weeks solid! Thankfully I have air conditioning, but it has been brutal to be outdoors.
Concentrations of ground-level ozone have reached and stayed at advisory levels. This is formed when pollutants given off by the forest fires and compounds from the solvents used to put out the fires react in the air, in the presence of sunlight.
Even wearing an N95 mask outside which is designed to filter out the small smoke particles, I have found my breathing very laboured.
Needless to say, my morning and after-dinner walks have been impossible. I tried exercising indoors, but my lungs were simply too irritated from the small smoke particles.
I have continued with delaying the time between meals (referred to as “intermittent fasting”)but for shorter periods of time as my body is under physiological stress and I continue to eat a low carb high fat diet. My weight has dropped another pound over these last two weeks, despite no exercise at all. My blood sugar on the other hand is considerably higher without the walks.
An air quality analyst with Metro Vancouver has reported that the weather is expected to shift this coming weekend, allowing some of the smoke to begin to dissipate. Until then, part of taking care of my health is not to exercise.
Reporting from Tatooine, British Columbia, I’m Joy Kiddie, practicing what I preach.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
It’s been 5 months since I began my own weight-loss journey, following a low carb high healthy fat diet and here is a short update.
Fasting Blood Glucose
When I began this journey at the beginning of March, my fasting blood glucose was averaging 12 mmol/L. Four months into eating low carb high fat, my fasting blood sugar was averaging 8.5 mmol/L.
July 25th, it was measured at the lab and on my home glucometer as 8.0 mmol/L – still way above the cutoffs for those with Type 2 Diabetes of 6.0 mmol/L, and way above the normal levels of 4.5-5.5 mmol/L.
It is highest is in the morning, I believe due to cortisol’s effect (see 4 month update, for details).
2 hour Post-Prandial Blood Glucose
I’ve been tracking my blood glucose regularly since I started implementing the dietary and lifestyle changes 5 months ago, and my 2 hr post prandial (after a meal) glucose had been averaging ~7.2 mmol/L, which is much better than the 7.7 – 8.6 mmol/L which is what it was at the beginning of March, but still no where good enough!
…but I noticed that after I go for my brisk 3-4 km each morning, it is 5.4 mmol/L. This gave me an idea (see below).
Blood Glucose through the night – effects of Cortisol
For about a week, I measured my blood glucose at 1 AM and 4 AM and 6 AM (in the interest of science, of course!) with a brand new glucometer that I standardized at the lab, when I had my fasting blood glucose and fasting insulin done on July 25th. My morning fasting blood glucose would rise to ~6.6 – 6.8 mmol/L (119 – 123 mg/dl) from the 5.4 mmol/L it was when I went to bed, even though I hadn’t eating or had anything to drink. This had to be the effect of cortisol!
Fasting Cortisol
I had my fasting cortisol assessed the same day that I had my fasting blood glucose assessed (July 25 2017) and it was, as I suspected, high: 421 (125-536) nmol/L
…and this is with walking 4 km / day and sleeping 8 hours (restful sleep).
I need to come up with some additional strategies for lowering stress.
Fasting Insulin & Calculating Insulin Resistance
I also had my fasting insulin assessed the same day that I had my fasting blood glucose and fasting cortisol assessed (July 25 2017).
Based on the July 25th lab work, I calculated my Insulin Resistance using both Matthews (1985) Equations (HOMA1-IR), as well as using Oxford University Center for Diabetes, Endocrinology and Metabolism homeostasis model assessment (HOMA2-IR) calculator (2013).
From when my fasting insulin and fasting blood glucose was last tested 2 years ago in August 10, 2015, my insulin resistance calculated by HOMA2-IR had gone down from 3.06 to 2.77, but it’s still too high because my fasting blood glucose remains high.
Average Insulin Resistance – in the normal population
One study reported that the average HOMA2-IR in the general (non-Diabetic) population is 2.1 +/- 2.2 (Diabetes Care, Volume 24, Number 3, March 2001), so I am guessing that a HOMA2-IR of 1.00 would be a healthy target – one that will likely take me a year to approximate.
Whether that will be possible with diet and lifestyle change alone, has yet to be seen.
That is my goal.
High Morning Glucose – assessing the problem
I believe the reason that my blood glucose remains high in the morning is due to a combination of residual hepatic (liver) insulin resistance (from years of eating way too many carbs) and high cortisol that is stimulating an overproduction of waking glucose.
Effect of Walking
The last 5 months, my fasting blood glucose has been consistently high at 8.0 – 8.5 mmol/L (144 – 153 mg/dl) and my 2 hour postprandial is fine for a Type 2 Diabetic at ~7.2 mmol/L – but a far cry from the non-Diabetic range I am seeking.
…but I noticed that after I go for my brisk 3-4 km walk each morning, my fasting blood glucose is 5.4 mmol/L (yes, I go fasting).
The effect of moderate exercise seems substantial, so I decided to see what effect there would be on my early morning fasting blood glucose levels if if I took a short walk after dinner.
The results were dramatic!
For the last week and a half, my blood glucose drops to ~5.2 – 5.4 mmol/L (94-97 mg/dl) after a very leisurely 15-20 minute walk around my neighbourhood.
High Morning Glucose – assessing the solution
Based on my high fasting blood glucose of 8.0 mmol/L on July 25th, my physician’s colleague naturally recommended that I go on Metformin, but I have decided to hold off on introducing it for 3 months provided that;
(1) I continue the dietary and lifestyle changes I have been doing for the last 5 months and…
(2) I add a 20-minute walk after dinner.
Plan to Reassess in Three Months
I am requesting that my physician provide me with a requisition to have my fasting insulin and FBG re-run in October, when I update my HbA1c, so I can recalculate my HOMA2-IR again and see how much less insulin resistant I am by then.
I want to know the magnitude of the insulin levels dropping, not just the fasting blood glucose, which I expect, will drop…after all, the goal is to lower the very high levels of insulin. High blood glucose is a symptom – the cause is too much insulin being released, due to insulin resistance.
Blood Pressure
As mentioned previously, I asked to be started on a very low dose of Ramipril (Altace) about 6 weeks ago, as my blood pressure had begun to creep up again. When I saw 160/90 mmHg two days in a row, I went to see my doctor.
10% of the time I am ≤ 119 / 79 mmHg, considered normal blood pressure
64% of the time I am ≤ 120/80 mmHg, categorized as “Prehypertension”.
…and 26% of the time, measured before I take my medication, I am ≤ 138/90 mmHg, categorized as “Stage 1 Hypertension”.
I will continue to take the blood pressure medication as a temporary measure to offer some protection against heart attack, stroke and kidney damage until I lose some more weight, and my blood pressure stays down on its own.
Weight
Overall, in the last 5 months, I have lost 12 pounds and ~3 inches off my waist. I’ve lost about the same number of inches off my neck circumference (3 inches) which has had a dramatic effect on how I look. I have a neck and ONE chin.
I’ve lost overall about an inch off my mid-arm, an inch off on my thighs (gaining muscle and losing fat, at the same time) and lost around an inch off my chest.
Lowering Stress, Lowering Insulin
I need to get my cortisol levels down, as these are driving my high morning fasting blood glucose levels. Walking in the morning has been good, adding the short evening walk even better. Now I am adding (on alternate days from my 3-4 km walks) a workout with 5 and 10 pound weights and other forms of resistance training. I am even jumping rope (which has gotten much harder since when I last did it at around age 16!).
The goal is to get my insulin levels down, and I am already doing everything that needs to happen for that; eating only the carbs necessary to have a nutritious diet, with no excess protein and extending the time between meals (intermittent fasting) a few days per week.
It is going to take time…
Over the next 3-6 months, I expect fasting insulin will keep falling.
My goal over the next year is to reach a ‘normal’ 2 hour postprandial peak of 60 mIU/L (430.5 pmol/L) as determined by Dr. Kraft’s Insulin Response curves, which should be an Insulin Resistance (HOMA2-IR) of between 1.0 and 2.0.
Over time, the fat in my liver (“hepatic adiposity”) will continue to decrease, and the derangement which took time to develop will resolve.
While the rate of resolution to for me to achieve normal insulin metabolism is unknown, I know if I keep doing what I am doing, it should happen. It doesn’t always occur, but I won’t know if I don’t try.
Have questions?
Want to know how I can help you achieve your health and weight goals? Why not send me a note using the “Contact Us” form, above.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
As I’ve made it a habit to do each weekday, this morning I went out for my walk, using Nordic poles. I had an appointment to keep, so I kept it to 3 km at a brisk pace, around that beautiful lake that I’ve previously posted a video update from.
Despite eating quite low carb and delaying the amount of time between meals each weekday, my fasting blood sugars remain high. I’ve noticed that after I walk in the morning, they come down significantly, so I’ve decided to integrate a short walk around my neighbourhood after dinner, to see if my fasting blood glucose lowers. It should, which leaves me to determine how long a walk is ideal. I don’t want to make it a “workout”, as that can interfere with sleep, but I also don’t want to make it so short that it doesn’t have any effect. Today I started with a 15 minute walk at a comfortably brisk pace. Tomorrow, I’ll try longer, to see if it changes the results in the morning, and if so by how much.
As I began my walk, I realized that I’ve lived in this neighbourhood for several years, yet never walk around it. I guess it’s time I get to take in the beauty that is all around me.
Practicing what I preach!
Joy
UPDATE
It turns out, that a leisurely 20 minute walk after dinner results in my blood glucose dropping to ~5.2 – 5.4 mmol/L (94-97 mg/dl) and staying that way through the night (measured at 1 AM and 4 AM and 6 AM in the interest of science, of course!).
Note: Everyone’s results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody’s nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
It’s been 4 months since I began my own weight-loss journey, following a low carb high healthy fat diet and I’ve been to the lab and had my blood tests. Here is an update on my progress to date.
Blood sugar
Fasting blood sugar
When I began this journey at the beginning of March, my fasting blood glucose was averaging 12 mmol/L – and this was when I was eating the ‘standard recommended diet’ for someone with Type 2 Diabetes. My diet was high in complex carbs, and low in saturated fat. Also, as has been traditionally recommended for someone with Type 2 Diabetes, I ate 3 meals per day and made sure to have 2 – 3 snacks per day (each with complex carbs and some protein).
Now, four months into eating low carb high fat, my fasting blood sugar is averaging 8.5 mmol/L. It is significantly better, but not what I had hoped which was to be at or below 6.0 mmol/L (below the Diabetic cutoff range) in this time. There were factors that I was not considering.
Firstly, my blood sugar has been persistently high in the morning since I have been in nutritional ketosis – significantly higher than 2 hours after a meal. At first, I couldn’t figure out why. I’d been tracking my blood glucose at various times of the day; fasting, before I eat, 2 hours after I eat, before bed etc., but regardless what I ate the night before, it was highest in the morning. It was then that I began to suspect that the effect of the hormone cortisol might be a factor.
Cortisol is our “fright and flight” hormone and under stressful conditions, such as being chased by someone or something, cortisol provides the body with an immediate source of glucose by breaking down our glycogen stores in our muscle and liver (a process called glycogenolysis) and uses them to manufacture glucose in the liver (a process known as gluconeogenesis).
All hormones have a natural cycle of rising and falling throughout the day and this is known as a hormone’s circadian rhythm and over the course of the night, cortisol production begins to climb around midnight and reaches and is highest level between 6 am to 8 am. When I began to track my blood sugar from 10 pm until 8 am, I noticed that it would start going up in the wee hours of the morning and keep rising until 6:30 or 7 am, am when I would take it. It was then that it became evident that my fasting blood sugarwas rising with cortisol.
Chan S, Debono M. Replication of cortisol circadian rhythm: new advances in hydrocortisone replacement therapy. Therapeutic Advances in Endocrinology and Metabolism. 2010;1(3):129-138. doi:10.1177/2042018810380214.
When we sleep, our body breaks down the glycogen stored in our muscle and liver and converts it to glucose for our blood – an entirely normal process. Since I am following a low carb high fat diet and have been in nutritional ketosis for while, my body uses ketones as its primary fuel source and make all the glucose it needs for my blood from the protein and fat in my diet. When it runs out of that, it burns my stored fat for fuel – which is exactly what I want it to do! Since I’d been keeping my carbohydrate intake consistent but not very low, when cortisol levels would rise over night, my body would break down my glycogen first, then my own fat stores to make glucose for my blood, which I suspect is the origin of my high fasting blood glucose. That, combined with my liver still being insulin resistant, the glucose has no where to go.
This made sense to me and explained why my fasting blood glucose remained high, despite no carb creep (more carbs than planned for).
Since I’m keeping myself in nutritional ketosis, I’m not concerned about my fasting blood glucose remaining higher, although I may try distributing my carbs differently – with fewer at night. Since my goal is lower insulin resistance, I am going to continue to focus on that. High blood sugar is a symptom. The problem is insulin resistance.
My blood glucose 2 hours after meals has been getting better. It is now averaging around 6.0 mmol/L (sometimes hovering around 5.5 mmol/L) which is much better than 7.2 – 8.6 mmol/L which is what it was at the beginning of March. My goal is to see it consistently below 5.0 mmol/L after meals by mid-November.
HbA1C – glycosolated Hemoglobin
Glycosolated hemoglobin (HbA1C) is the hemoglobin in our red blood cells that gets sugar molecules attached to it proportional to the amount of sugar in our blood. It is used to measure the three-month average plasma glucose concentration, based on the fact that the lifespan of a red blood cell is four months (120 days). The advantage of this test, is that one does not need to be fasting to have it.
HbA1C is most strongly correlated with fasting blood glucose (as opposed to pre-meal blood sugar or to 2 hour post-meal blood sugar) and since my fasting blood glucose has been consistently high, my HbA1C results naturally reflected this. Lab tests indicate it is 7.5%, which is above the upper cutoff for Type 2 Diabetics of 7.0% – and higher than what I was aiming for, which was below 6.0%, the Diabetic range cutoff. However, since neither fasting blood glucose nor HbA1C measure what I am trying to change (which is insulin sensitivity), I’ve decided that in November, I will pay to have my fasting insulin re-assessed. After all, the goal is to lower insulin – which underlies the high blood sugar!
Lowering Stress
I knew that I needed to get my cortisol levels down, as cortisol drives appetite, which drives eating which in turn, causes insulin to be released. More insulin means my body will be focused on fat storage, not fat burning which is the opposite of what I want. Since my goal is lowering insulin resistance, lowering cortisol makes sense. Since I can’t change cortisol’s natural circadian rhythm, I had to focus on lowering the whole curve! Lowering stress wasn’t going to happen sitting at my desk working. I had to get moving. More on that, below.
Blood Pressure
As mentioned in my last update, a month ago I asked to be started on a very low dose of Ramipril (Altace), as my blood pressure had begun to creep up again. When I saw 160/90 mmHg two days in a row, I went to see my doctor. He wasn’t there, but the locum agreed with my assessment that it was wise to protect my heart, brain and kidneys while I continued to make the dietary and lifestyle changes. She asked me to delay getting my blood work for a few weeks, to assess my electrolytes (sodium and potassium) level which can be affected by the medication.
Even two years ago, my potassium was at the high end of normal – and this was when I was dutifully eating a diet high in complex carbs and low in saturated fat, as I ate a diet high in potassium-rich foods.
This time my potassium was at the upper normal limit, so I’m tracking my intake of it and keeping it approximately 1/3 to 1/2 of what it was previously.
Taking the blood pressure medication is a temporary measure that I decided on in order to offer some protection against heart attack, stroke and kidney damage until I lose more weight, and my blood pressure stays down on its own.
Thankfully, my overall kidney function is now better than it was 2 years ago, although I did need to make a few dietary changes to be sure that I avoid getting kidney stones (something that runs in my family). When I started exercising regularly a month ago, I didn’t adequately increase my water intake – which I’ve since corrected. I had also added a calcium supplement when I stopped drinking milk in March and which was binding with certain food components in the veggies and nuts I was eating. This was probably what was resulting in calcium-oxalate being detectable in my urine. I’m no longer taking the calcium supplement and have added more hard cheese into my diet, instead.
Cholesterol
My LDL was at the high-end cutoff two years ago, but after 4 months on a low carb high healthy fat diet, it is approaching what is considered by the existing / popular standards of “optimal LDL” for someone who is high risk (family history of cardiovascular disease). My LDL is 2.60 mmol/L (1.14 mg/dl), my triglycerides (TG) were 0.64 mmol/L and my HDL was 1.97 mmol/L.
Using more significant measures, my TG:HDL ratio is now 0.32 (with <0.87 considered ideal). According to several studies (that I will go into more detail in an upcoming article), a very low TG:HDL ratio is associated with lots of large, fluffy LDL – the kind associated the lowest risk of cardiovascular disease (CVD) such as heart attack and stroke. It is the higher density, small LDL particles that are associated with CVD.
Walking
A month ago, I began walking every morning during the weekdays. I had just fractured a rib (slipping washing a bathtub!) and read that walking was good to reduce pain. Since reducing pain was high up on my “to do” list, I started with walking 1 km each morning during the week, before I began my office hours. I gradually increased it to 2 km. The last week and a half it has been 3 km.
At the beginning of last week, I saw a fellow who was in very good shape using Nordic walking poles,so I asked him why he used them. He explained that as he digs the poles into the dirt on the path and pushes himself off of them, it gives him a good upper body as well as the lower body workout that comes from walking briskly. I decided to get myself some.
I researched what height they needed to be and decided whether I would get adjustable height ones or not, and purchased them on Friday and over the weekend, I read about how to use them properly. It seemed as thought it would be pretty intuitive for me, given that I have (and use) a Nordic Track ski machine when the weather is not conducive to going out to exercise.
Nordic Walking Poles
I was skeptical that using them could actually increase the calories I burned by 30%, for the same distance walked until I tried them this morning.
I am no longer skeptical!
I was very well aware of how much better a workout I had gotten after 2 km, but did another 1 km anyways. I can’t wait to go again tomorrow.
Getting Even More Serious
Reducing Carbs
A month ago my weight was still ‘stuck’ at its 6 pound weight loss, so I decided to reduce my carbs slightly but consistently and to monitor my intake of nuts and dark chocolate, which could easily cause me to exceed my carb ceiling.
Bingo!
Intermittent Fasting
Monday – Friday I wasn’t hungry in the morning, because I would eat a very satisfying meal the night before (with adequate protein and lots of healthy fats and low carb veggies), so I was and am quite content to have only a coffee and cream for breakfast, and then go for my walk.
When I come home, most days I’m really not hungry, because my body had finally figured out how to burn my own fat stores for energy!
At first when I started exercising (nothing crazy…I was just walking briskly!) and delaying the time between meals, I needed to monitor my blood sugar even more often as it could get quite low in the late afternoon before dinner (+/- 4.0 mmol/L) – at which point I would eat something as I prepared dinner, to raise my blood sugar.
Here is a graph showing my blood glucose since I started walking and intermittent fasting;
Blood glucose since beginning walking and intermittent fasting
Weight Loss
In the last 3 weeks, my weight has dropped another 4 pounds, making it a total weight loss of 10 pounds, in all so far. I expect as I continue to walk 4 days a week and intermittent fast most weekdays and limit my carbs, that the weight and inches will continue to come off.
I am not suffering in any way!
As a Dietitian, I talk about or write about food all day long and I’m intermittent fasting and feel just fine! I’m not hungry. As I jokingly posted last week;
“My body has finally figured out how to make glucose from my fat on a low carb high fat diet. I may potentially have found the source of immortality.
Final Thoughts…
I still have at least another 30 pounds to go to get to the “goal weight” that I set at the beginning of this journey, and am now aiming to lose another 40-45 pounds instead in order to reach my ideal (healthiest) waist to height ratio. I clearly won’t accomplish this by mid-November, but if I reach close to my initial goal weight, I will be quite content.
They say a picture speaks a thousand words, so below are two photos. The one on the left, with the blue shirt is me at the beginning of this journey. The one on the right, with the burgundy shirt is me now. I am starting to see a face I recognize.
Have questions?
Want to know how I can help you reach your own nutrition goals? Please send me a note using the “Contact Us” form above, letting me know how I can help.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Today marks 3 months since I started my own weight-loss and getting-healthy journey and so I’m posting this short update.
While I’ve only lost 7 pounds, I’ve lost a remarkable 4 inches off my waist, which is greatly encouraging, as I still have another 6 inches to lose (based on my height-to-waist ratio). I know without a doubt that this is entirely ‘doable’!
I look in the mirror and recognize the person looking back. I recently bought new jeans that are a full size smaller and when the weather has been hot, I’ve not only worn shorts, but I’ve wore them out of the house.
My blood pressure is very stable and now fluctuates between stage 1 hypertension and pre-hypertension; a dramatic improvement from the wildly erratic fluctuations between stage 2 and stage 1 hypertension, with a hypertensive emergency thrown in for excitement. It was that crazy high blood pressure which started me on this journey, but what keeps me on it, is how I feel. I feel great!
My blood sugar has been great after meals, but recently has become quite a bit higher several hours after eating, even though I have not eaten or drunk anything except water. From the reading I’ve been doing in the literature, this has been reported in those who previously had what is called “dawn syndrome” (high morning fasting blood glucose – which I had) after they’ve adopted a low carb high fat diet. It seems that the second of the two stages of insulin release is suppressed in those such as myself, causing blood glucose to remain higher for a longer period of time. One way of addressing this is via exercise, so it seems I will be doing this more than once in a while to manage this.
This morning it was gorgeous out; clear sky, cool temperatures and the track was beckoning me, and so I went. I haven’t worked out more than 2 or 3 times a month since I began my journey, but despite that, I noticed a huge improvement in my fitness level today. I can only attribute that to the loss of fat around my middle. I did an extra two rounds on the track at a pretty decent clip, with a total distance of 3.2 km (2 miles). I could have done another round (maybe two) but thought I might be too stiff tomorrow, and since my goal is to do this more often to address my second stage insulin suppression, I decided to ‘call it a day’ after 3 km. As I was leaving the track, I decided to take a short video to post along with this 3-month update. Have a look at the video which is posted below, and compare it with the one from 3 months ago. My progress is evident.
Want to know how I can help you accomplish your own health and fitness goals?
Please send me a note using the “Contact Us” form above and I’ll be happy to reply.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
INTRO: Three weeks ago, the pain of changing was less than the pain of remaining the same and so I changed. At that time, my blood pressure had hit dangerously high levels and I didn’t even know what my blood sugar levels were, as I hadn’t checked them in ages. I didn’t want to know. Despite being a Dietitian, I was in classic denial. March 1st, I began eating low carb high fat (LCHF) and delaying the time until the next meal (called “intermittent fasting”). Keep in mind, three weeks is an incredibly short period of time, but I did not expect to see these kinds of results. There was not only significant weight loss (water?) but loss of inches around the waist (also water?), but lower blood sugar and blood pressure, as well.
Today is three weeks since my journey began and here is an update on my progress – three weeks in.
Blood Sugar
In the first two weeks, my blood sugar decreased substantially even on the days I was not intermittent fasting – provided I ate very few carbs. When I was eating what most would consider “low carb”, my blood sugar would spike.
arrows indicated 2 periods of eating 10-15% carbs
It became clear that as long as I kept my net carbs (carbohydrate minus fiber) fairly low, I did very well but above a certain level my body could not handle the sugar load. You can see this from the graph above.
On Saturdays I was eating more than that level of carbs, which can be seen indicated by the grey arrows, below the graph. My blood glucose would spike if I had any more than the carbs found naturally in low carb meals.
I could see clearly that I was very insulin resistant -which is no surprise, considering I was diagnosed with Diabetes ~ 10 years ago. Despite my pancreas producing more and more insulin in response to eating carbs, the insulin was unable to take the glucose (sugar) from my blood in a reasonable amount of time, to store it in my liver.
[Note: According to the research of Dr. Joseph R. Kraft between 65-75% of people with normal blood sugar are actually insulin resistant – that is, they have the same risk of hardening of the arteries and heart attack as those with Diabetes, they just don’t know it because they don’t have high blood sugar to indicate that. That’s is very sobering.
Since realizing how sensitive I was to more than the carbs naturally found in non-starchy vegetables and nuts and seeds, I cut out all other sources – including my beloved Hawaiian purple yam and homemade (baked) yam fries…for now, until my blood sugar levels are consistently in the non-diabetic range and my insulin levels, normalized. Even then, I know I will only be able to eat such things once in a while and in small servings, but that’s okay. As one of my sons would say “dying is bad“.
A week ago, I began tracking my carbs (easy to do and requiring no apps – not even a pencil). I aimed to keep them at the same lower levelsand as you can see from the graph below, there has been linear decrease in my blood glucose levels at all times of the day – including first thing in the morning, after lunch, after dinner and before bed. It’s only been three weeks!
Week three – March 15 – Mar 21
Interestingly, the little ‘spike’ yesterday was in the early morning after – I hadn’t eaten for 12 hours! The effects of cortisol, perhaps?
My body was breaking down the fat I have stored and was converting it into glucose for my blood – a process known as lipolysis. This is a ‘good’ thing. My body was doing exactly what it was designed to do;
(1) store excess glucose as fat, in times of plenty,
(2) break down stored fat for glucose, in lean times.
The issue is, there have been no “lean times”.
Blood Pressure
Week One
The first week my blood pressure was divided up between
50% Stage 1 hypertension
~30% Sage 2 Hypertension
1 hypertensive emergency (not good!)
<15% pre-hypertension
It was all over the place (very hard on the heart) and the systolic pressure (the first number in a blood pressure) was very high.
After the issue with my eyes (which was non-diet or lifestyle-related) having hypertension (high blood pressure) put me at risk for blindness. I took this very seriously!
Week Two
The second week my blood pressure dropped to;
>80% Stage 1 Hypertension
<20% pre-hypertension
This can largely be explained by the fact that the first thing that happens when we reduce insulin levels (a response to eating low carb) is something called naturesis. That is simply a medical term meaning our kidneys get rid of the excess salt by making us pee a lot. This period usually lasts ~4-10 days following going low carb.
Week Three
This week my blood pressure was;
~85% Stage 1 Hypertension
~15% pre-hypertension
Yes, it was a tiny bit higher, but very stable.
The first two weeks I ate very low sodium as I usually did, but this week I actually had to start adding salt into my diet as my kidneys had expelled all the excess sodium it was retaining and my sodium levels were too low. I felt a bit lethargic and light-headed. The reading I’ve been doing in the literature and the Conference Proceedings I’ve been watching from some of the world’s leading physicians that treat diseases (such as Diabetes, hypertension / high blood pressure, dyslipidemia / high cholesterol as well as Alzheimer’s and some cancers) using a low carb high fat diet, mentioned this need for increasing sodium after the first 10 days.
A pleasant surprise was seeing my diastolic pressure (the second number in blood pressure) hit normal levels several times.
One of the roles of insulin (besides taking the glucose in our blood and storing it in our livers as glycogen or fat) is to signal the kidney to retain salt. That makes us bloated and causes our blood pressure to go up.
Being Diabetic or insulin resistant (65-75% of people aged 3- 90 years, according to Dr. Joseph Kraft’s robust studies) causes people to retain sodium and raises their blood pressure. Hypertension (high blood pressure) is called “the silent killer” – but much of this is entirely diet related. For the most part, is not too much salt, but too many carbs and too little green leafy veggies (rich in potassium) that underlies high blood pressure.
Anthropometrics
Weight
The first week and a half, my weight dropped ~4 pounds – much of it was water, from my kidneys expelling the excess sodium. My weight didn’t budge for most of the last week and a half, but I didn’t let that discourage me. My body was now burning fat and not carbs and the weight loss necessarily had to follow.
It is now the end of the 3rd week, and I have lost 5 pounds all together.
Waist Circumference
In the first two weeks, I lost 1 inch off my waist and this week, another 1/2 inch came off. That is a very good thing – but for a different reason than I thought.
As Dietitians, we were taught that BMI (weight-to-height ratio) and waist-to-hip ratio allows us to factor in the greatest risk of cardiovascular events (heart attacks, strokes) but current research is showing that there is a much better predictor years of life lost (YLL) due to overweight, and that is the waist-to-height ratio.
Years of Life Lost (YLL) compared to Waist to Height Ration (WHtR)
Most of us have heard that where we carry our fat is even more important than how much of it we actually have. This is true.
Carrying it around the abdomen (belly fat, what Dietitians and Doctors call “central adiposity”) is a greater predictor of cardiovascular risk than BMI (weight to height ratio). Simply put, being an “apple” as opposed to a “pear” is not good.
But what should our waist circumference be?
A meta-analysis from 2012 pooled data from multiple studies which in total looked at more than 300, 000 adults in several ethnic groups, found that Waist to Height Ratio (WHTR) was a far better predictor than BMI or Waist Circumference of cardiovasular of metabolic risk factors in both sexes.
Ashwell M, Gunn P, Gibson S (2012) Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev 13: 275—286
The least amount of years of life lost is associated with a Waist to Height Ratio of 0.5 (mine was not anywhere near that!).
That is, take your height and divide it by 2.
NOTE: Measure your waist at the location that is the mid-point between your last rib and the top of your hip bone, with the front and back of a flexible seamstress-type tape measure at the same height, and your belly fully relaxed. This is not the time to suck it in! If you measure your height in inches, measure your waist in inches and if you measure your height in cm then measure your waist in cm.
If the result of your Waist to Height ratio is greater than 0.5, then welcome to the club. The question is, what to do about it?
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
In the previous article titled “A Dietitian’s Journey – the beginning”, I shared about why I am (1) following a low carb high healthy fat diet and (2) extending the time between meals in my pursuit of improved health. In this post, I talk about the smaller third of the picture, (3) exercise. Why I am doing this is because quite literally, my life and quality of my life depends on it.
This “journey” is my road to better health – to optimal health.
As a Registered Dietitian in private practice, I’ve spent the last decade helping people in the Lower Mainland of Vancouver learn how to eat healthier, lose weight, lower their blood sugar and blood pressure and have cholesterol that is in the healthy range. While I had lost 50 pounds myself a few years ago, little by little over the last 2 years, I’d put 1/2 of it back and along with the higher weight, came higher blood sugar levels, followed by high blood pressure.
My “fat picture” – prior to losing 50 lbs.
I had two choices; (1) go on medication or (2) change my lifestyle. I chose the latter. March 5 2017 was the beginning of the journey, on the road to better health.
But what was the “road”?
Over the last 2 years, I’ve done a lot of reading with regards to the physiology of why and how diets high in carbs underlie the “obesity epidemic”. I understood how excess carbs that were not needed for energy were converted to fat and stored in the liver. I also understood how this excess fat in the liver negatively impacted cholesterol levels – that it wasn’t eating fat that gave people high cholesterol (except for a very small minority with genetic conditions) but eating too many carbs.
Day in, day out in my private practice I’d explain to people how eating “plenty of fruit and vegetables” was making things worse for them because of the carb content in these foods – foods that were eaten with- and between meals. I knew that following the standard recommendations of the last 40 years – to eat low fat and high carbohydrate and restricting portions was not going to accomplish my goal.
I decided to “practice what I preach” by eating a low carb, high fat diet (LCHF), and by extending the time between meals. In time, I also hope to incorporate short periods of high intensity interval training (HIIT), but for now I just need to get moving!
Since I am not yet “fat adapted” – that is, my body hasn’t yet switched over to using my own fat stores as a fuel source, I knew that I needed to start with walking. Baby steps!
Yesterday, I set an appointment with myself to do just that, and while I was 3 hours later than I planned to be today, my ipod wasn’t charged and it was 5° C and pouring rain, I went to the track and did what I said I would do.
Note: I am a "sample-set of 1" - meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating "low carb" and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
I remember back at McGill, when I was doing my undergrad training as a Dietitian, one of my professors saying that most people chose Dietetics because they came from a background of disordered eating or diet-related health issues. True to form, most of my extended family were obese and most had Diabetes, high blood pressure and high cholesterol and were on a whole host of medications for each.
Fast-forward 20 years (and several children later) and despite losing 35 of the 60 pounds I had to lose, I became Diabetic. More recently, I’ve had high blood pressure.
Unable to answer my questions regarding addressing both of these through a low-carb-high-healthy-fat eating plan, my GP referred me to an Endocrinologist. After a thorough physical examination and a whole host of blood work, she asked me about how I planned to address this, given that I am a Dietitian. Hesitantly, I told her that I planned to eat a high healthy-fat diet and low carb diet with a medium amount of protein and use intermittent fasting to lower insulin resistance. She asked me what percent of “net-carbs” (total carbs minus fiber) I was aiming for and what percentage of protein and what my fat sources would be, and I told her. I was waiting for an extremely negative reaction, but instead was completely taken aback by her reply. She said that from she’s been reading in the literature, my plan was not only evidenced-based, but that if I didn’t don’t lose the rest of the weight and eat this way, that I will end up on both medication for my blood sugar, and cholesterol and likely for my blood pressure, too.
I began to implement the dietary and lifestyle changes and was seeing my “numbers” coming down, but like many people, life happened and I didn’t follow through. The weight crept up and presumably so did my blood sugar and pressure, but I had stopped monitoring those ages ago. But it was a problem with my eyes — one whose cause was unrelated to being Diabetic or having high blood pressure that was a game-changer for me. Having these conditions put me at higher risk of losing my vision and this was simply not something I was willing to risk.
Two weeks ago, I arrived at a fork-in-the-road. One direction was the same as most of my family took; with medication for blood sugar, blood pressure and cholesterol. The other was the road that I am taking; the one less traveled, but very well-researched, and with the encouragement of my Endocrinologist – a low-carb-high-healthy-fat way of eating, with extended periods of time between meals, and periods of days of eating and then not eating. Not “starving”, but “intermittent fasting”.
The difference?
Starving results in the body lowering its metabolism to spare calories and intermittent fasting and alternate-day fasting results in the body raising its metabolism and burning stored fat.
The expected outcome?
The first goal begins with lowering insulin resistance; which is the underlying cause of Type 2 Diabetes, and with lower insulin resistance follows lower blood sugar levels – both fasting blood sugar and A1C (3 month average).
A change in diet and strategic use of fasting, lowers insulin and cortisol levels which in turn, lower triglycerides (TG). TG are largely a byproduct of a high-carb diet (especially affected by fructose), so lowering these results in lower TG and in turn, lower levels of LDL (bad cholesterol) and higher levels of HDL (good cholesterol). Lower insulin and cortisol as well as less abdominal fat, results in lower, more normalized blood pressure.
Will it work? The research seems to indicate it will and over the weeks to come, I will posting the results of some of that research so that the context of what I’m doing can be understood. After all, I am a Dietitian and a scientist — it has to be evidenced-based.
The First Two Weeks – off to a good start
Blood Sugar
Of course this is an incredibly small period of time to look at, but in the first two weeks since I started my low-carb-high-healthy-fat eating with intermittent- and alternate-day fasting , my blood sugar has decreased substantially even on the days I was eating, provided I was eating very few carbs.
arrows indicated 2 periods of eating 10-15% carbs
Blood Pressure
My blood pressure went from 50% Stage 1 hypertension with 1 hypertensive emergency (scary!) and ~30% Stage 2 Hypertension the first week:
…to approximately 80% Stage 1 Hypertension and almost 20% pre-hypertension the second week.
That is a significant change!
My weight is only down ~ 4 pounds, but I’ve lost 1 inch off my waist.
I am not hungry on my intermittent-fast days …and keep in mind, I talk about food all day long with my clients. If I am not talking about food, I am working on meal plans and writing about food! If I was hungry, this would be torture, but it’s not. In fact, the last time I ate was last night at supper and I feel fine. I should have had a coffee though (as I get caffeine headaches if I don’t). I’ll make one soon.
I’ve only taken one alternative-day fast so far and it went fine. I drank “bone-broth” (I’ll explain in coming blogs!) and had my morning coffee with a little cream, no milk because of the carbs. I don’t really like cream, but it was okay. Bone broth is interesting — a bit like chicken broth, but different.
One side-bonus that I never expected, is that I am sleeping better than I have in years. Crazy good sleep and waking up rested. What a great added bonus.
I have a long way to go to get to my goals (plural) because I’ve set the bar very high…and why not? If the literature indicates that this works, then I want;
(1) blood sugar in the non-diabetic range
(2) normal blood pressure
(3) normal / ideal cholesterol levels
(4) a waist circumference in the “at or below” recommended values of the Heart and Stroke Foundation
Will I meet all these goals? Who knows?! But I won’t know if I don’t try and the alternative of a life of medication for blood sugar, blood pressure and eventually cholesterol too does not appeal to me!
So join me in my journey – a journey of change, of good health and on a road less traveled.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.





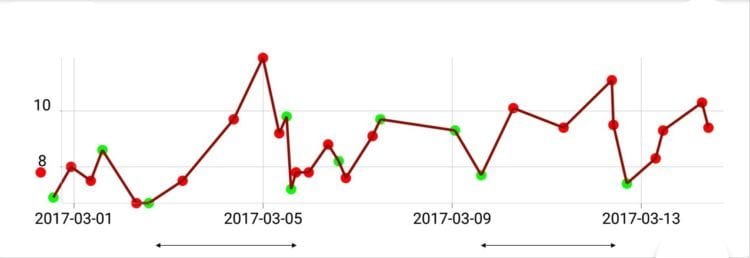
 As can be seen from the graph, my blood glucose was at lowest at 7.7 mmol/L (see photo to the left) and I had spikes well above 10 mmol/L, and I was averaging around 8.5 mmol/L over the course of the day – which is slightly higher than the average of those in the study.
As can be seen from the graph, my blood glucose was at lowest at 7.7 mmol/L (see photo to the left) and I had spikes well above 10 mmol/L, and I was averaging around 8.5 mmol/L over the course of the day – which is slightly higher than the average of those in the study.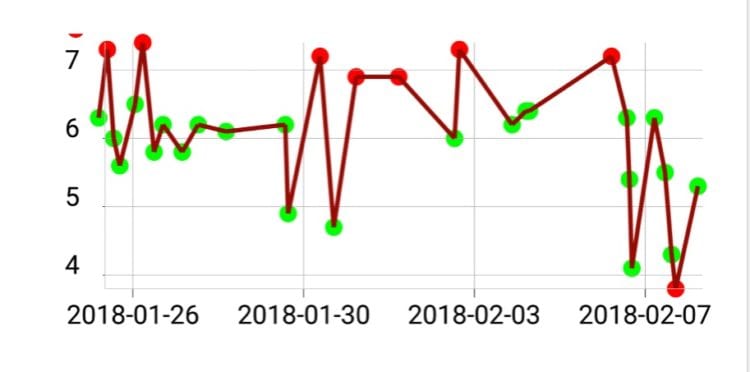
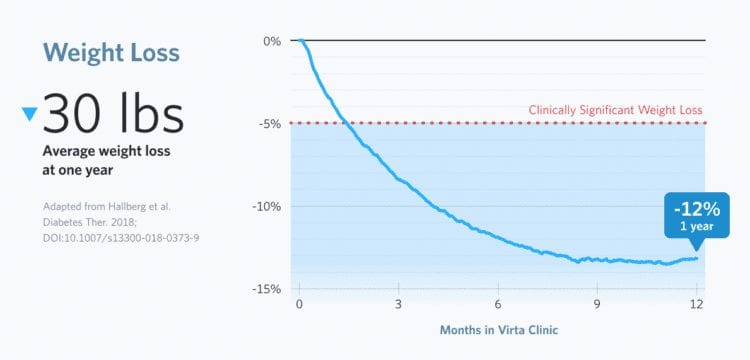
 Early this morning, my fasting blood glucose was 5.3 mmol/L (95 mg/dl) which is in the normal non-Diabetic range. This is a first! This was without taking Metformin.
Early this morning, my fasting blood glucose was 5.3 mmol/L (95 mg/dl) which is in the normal non-Diabetic range. This is a first! This was without taking Metformin.

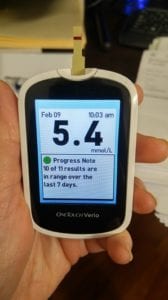





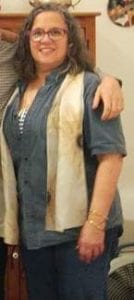 My journey began on March 5, 2017 when I was a fat Dietitian with all the benchmark symptoms of Metabolic Syndrome including Type 2 Diabetes, high blood pressure, high LDL cholesterol and triglycerides, abdominal adiposity (i.e. “a belly”) and high BMI (high weight for height). Physically I was a mess but my biggest problem was that I was in denial. It had been months since I had monitored my own blood sugar or blood pressure even though I had been diagnosed with Type 2 Diabetes 10 years earlier. I knew better.
My journey began on March 5, 2017 when I was a fat Dietitian with all the benchmark symptoms of Metabolic Syndrome including Type 2 Diabetes, high blood pressure, high LDL cholesterol and triglycerides, abdominal adiposity (i.e. “a belly”) and high BMI (high weight for height). Physically I was a mess but my biggest problem was that I was in denial. It had been months since I had monitored my own blood sugar or blood pressure even though I had been diagnosed with Type 2 Diabetes 10 years earlier. I knew better.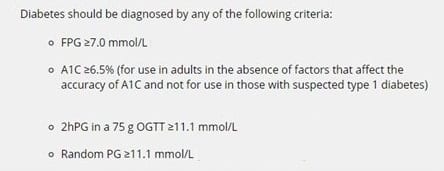
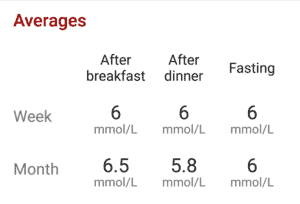
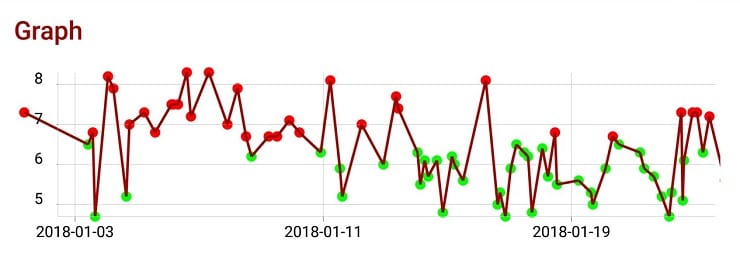
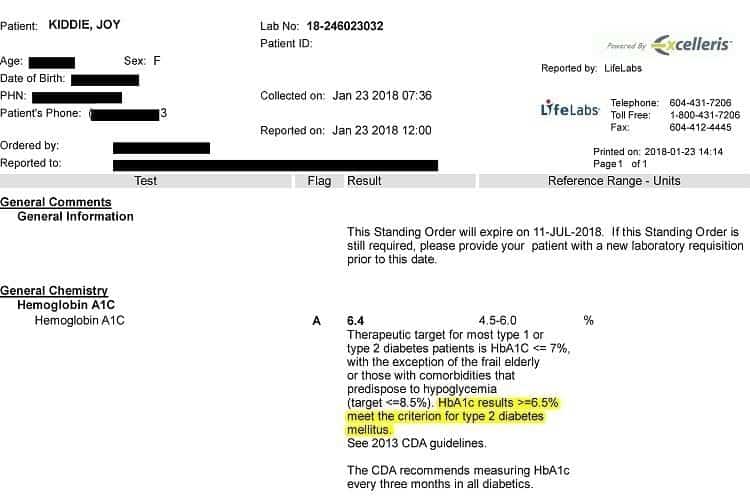
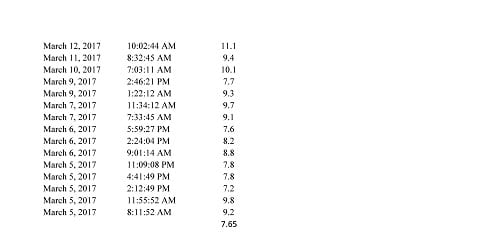
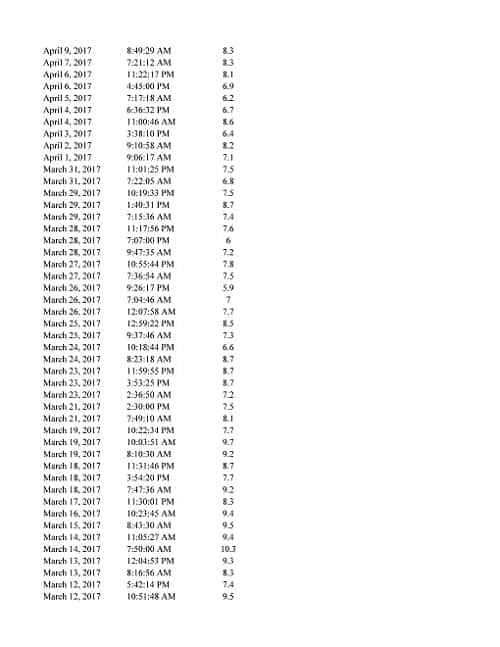
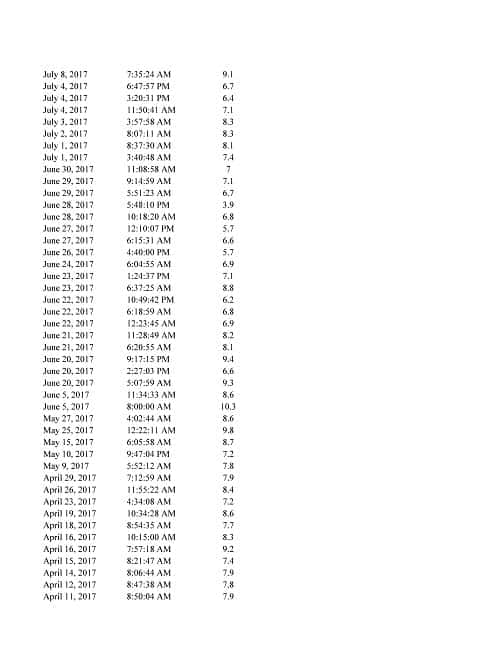
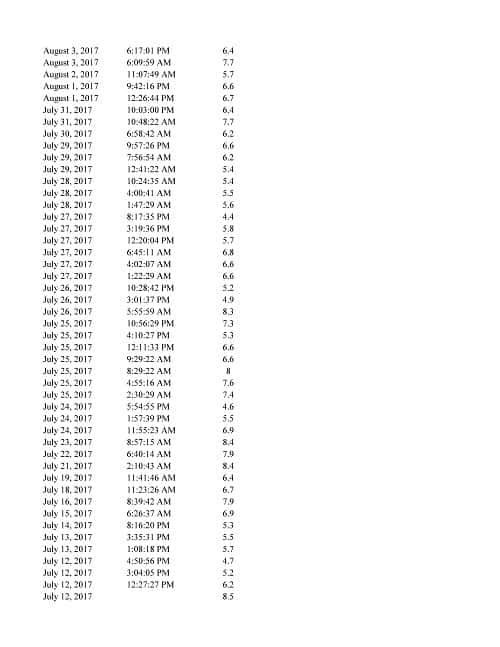
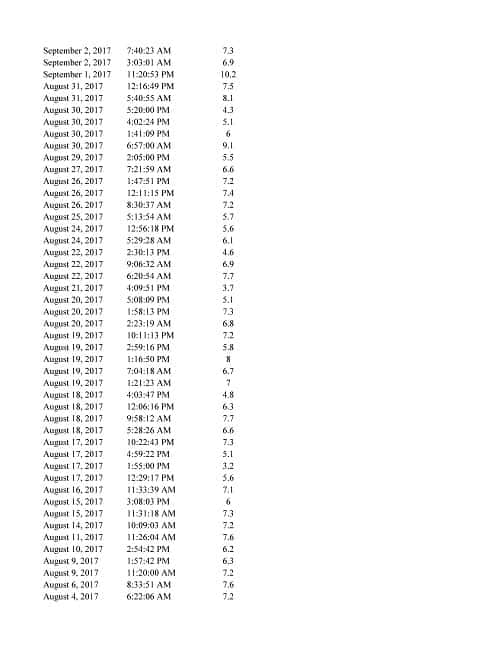
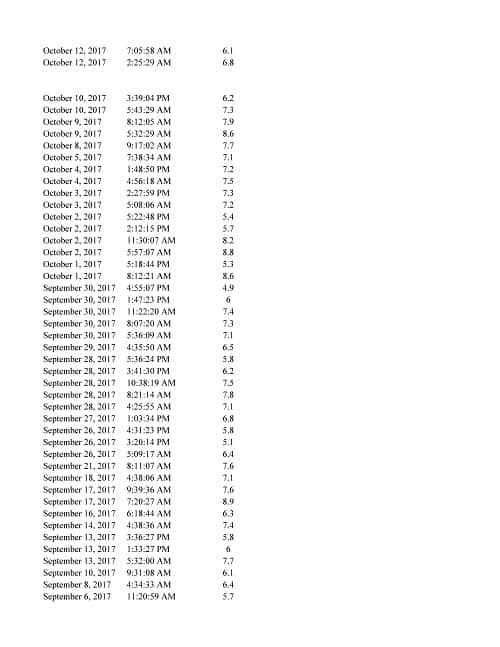
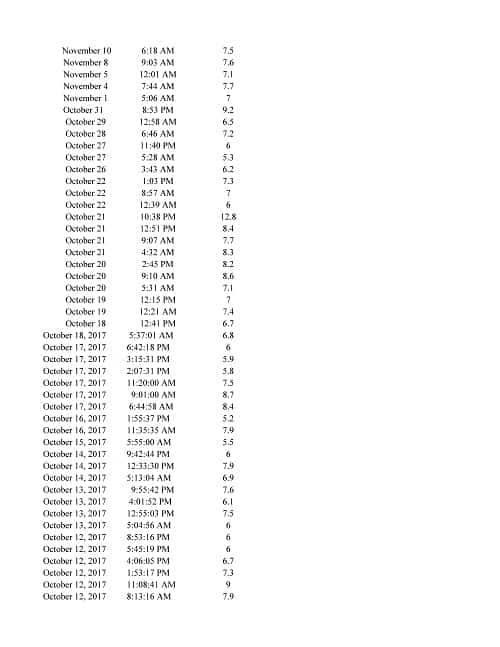
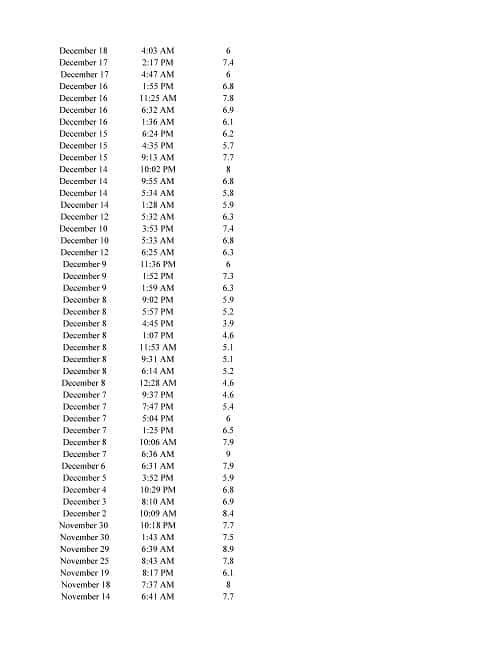
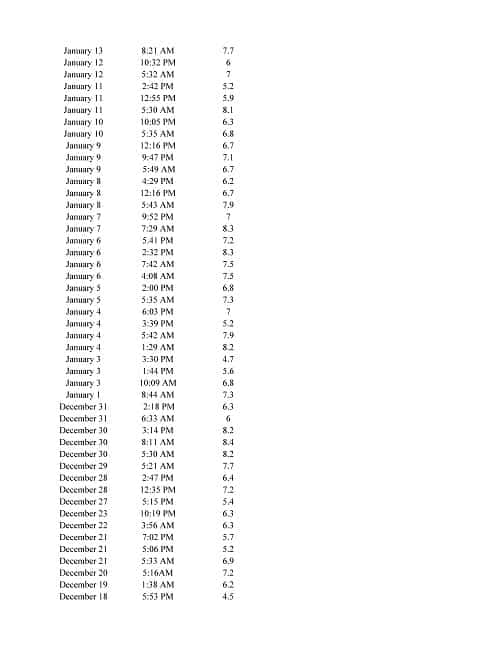
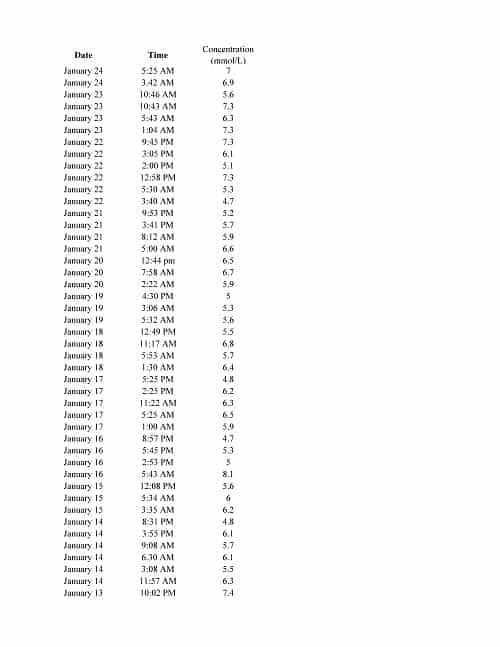










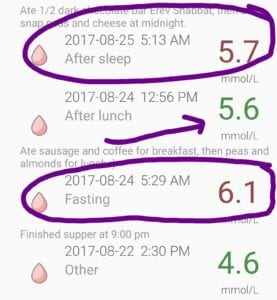
 Last night, for the first time since I was diagnosed with Type 2 Diabetes (T2D) ten years ago, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl).
Last night, for the first time since I was diagnosed with Type 2 Diabetes (T2D) ten years ago, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl). My cells aren’t yet ‘healed’. They and my liver are still insulin resistant which is evidenced by the fact that even though I haven’t eaten anything since dinner last night, my blood glucose is high.
My cells aren’t yet ‘healed’. They and my liver are still insulin resistant which is evidenced by the fact that even though I haven’t eaten anything since dinner last night, my blood glucose is high.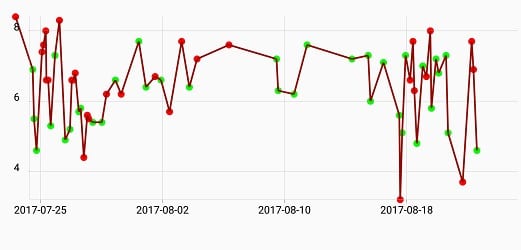
 Monday, my blood glucose was 3.7 mmol/L (67 mg/dl) at 4:00 PM and yes, I ate something immediately.
Monday, my blood glucose was 3.7 mmol/L (67 mg/dl) at 4:00 PM and yes, I ate something immediately.





 For the last 2 weeks, the Lower Mainland has been covered in smoke due to hundreds of wildfires in the area. The very poor air quality had made going for a walk impossible.
For the last 2 weeks, the Lower Mainland has been covered in smoke due to hundreds of wildfires in the area. The very poor air quality had made going for a walk impossible.


 Even wearing an N95 mask outside which is designed to filter out the small smoke particles, I have found my breathing very laboured.
Even wearing an N95 mask outside which is designed to filter out the small smoke particles, I have found my breathing very laboured.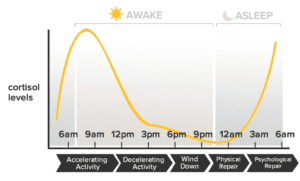
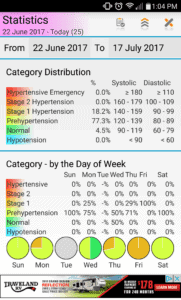 Taking the blood pressure medication is a temporary measure that I decided on in order to offer some protection against heart attack, stroke and kidney damage until I lose more weight, and my blood pressure stays down on its own.
Taking the blood pressure medication is a temporary measure that I decided on in order to offer some protection against heart attack, stroke and kidney damage until I lose more weight, and my blood pressure stays down on its own.