
This past weekend, thousands of American Certified Diabetes Educators (CDE) gathered at the American Association of Diabetes Educators (AADEs) annual conference in Houston, Texas. Objectives of the conference were for CDEs to learn how to implement novel and innovative ways to advance chronic disease prevention and management, and one of those novel ways was through the use of a Low Carbohydrate Diet.
It is very exciting that CDEs are now learning how to implement the American Diabetes Association’s (ADA) new 2019 Standards of Medical Care in Diabetes that was released this past December and which includes use of a low carbohydrate diet (you can read more about that here).
This conference provided education to enable CDEs to apply the content outlined in the ADA’s April 18, 2019 Consensus Report, which added the use of a very low carbohydrate (ketogenic) diet of 20-50 grams of carbs to the choice of meal patterns to manage both type 1 and type 2 diabetes. You can read more about the Consensus Report here.
As mentioned in the previous post, there were two Educational Sessions this past Saturday, August 11, 2019 about the use of a Low Carbohydrate Diet to manage and treat diabetes. The first session was titled Low Carbohydrate Diets; Fad or Evidence Based Course of Action and was given by Dr. Jim Painter, PhD, RD and Professor Emeritus from Eastern Illinois University, in Charleston, Illinois and this article covers that presentation in detail, including each of the slides and references used.
The second session was titled Person-Centered Implementation of Low Carbohydrate Eating Plans and was given as a joint-session by Dawn Noe, RDN, CDE and Diana Isaacs, PharmaD, CDE, both from Cleveland Clinic Diabetes Center. This second session is the subject of this article.
Copies of the slides and speaking notes for this presentation were sent to me by Dawn Noe, RDN, CDE. Many thanks to her and her colleague Diana Isaacs, PharmaD, CDE for sharing them with us!
The first part of the presentation was given by Registered Dietitian Nutritionist Dawn Noe and is covered in Part A and the second part was given by Doctor of Pharmacy Diana Isaacs and is covered in Part B.
Note: In a few places below, I have added my own clarifications that are clearly marked as *Note (bolded red asterisk *).
Person-Centered Implementation of Low Carbohydrate Eating Plans
Slide 1
 The first slide was a disclosure of financial relation / financial conflict of interest, as well as a statement of non-endorsement of products.
The first slide was a disclosure of financial relation / financial conflict of interest, as well as a statement of non-endorsement of products.
 Slide 2 – The second slide was a photo of each of the presenters, along with their credentials.
Slide 2 – The second slide was a photo of each of the presenters, along with their credentials.
Part A: Nutritional Approach – Dawn Noe, RD, CDE
Slide 3 – list of learning objectives.
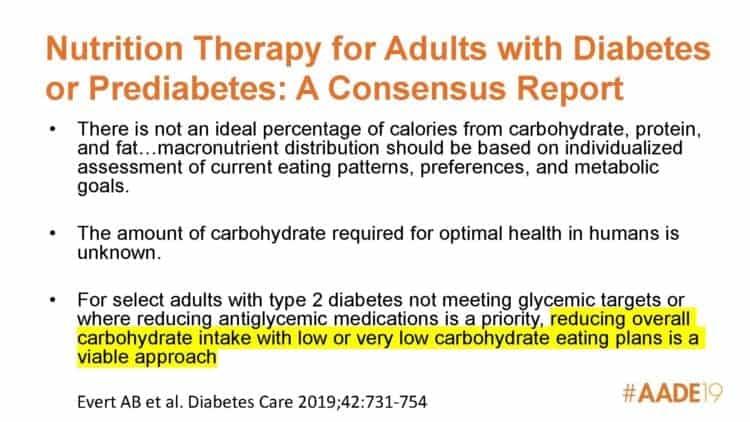
Slide 4 – Summarized some key points from the American Diabetes Association’s (ADA) Consensus Report
(Evert AB et al. Diabetes Care 2019; 43: 731-754.)
Speaking Point Summary
- There is no ‘ideal percentage of carbs’ shown in the literature, but despite this
many people with diabetes are told to eat ~60 grams of carbs at each meal, assuming 3 meals per day.
- These numbers are essentially calculated to be 50% of the calories coming from carbohydrate on a 1500 calorie meal plan.
- The 130 grams of carb per day recommended for adults without diabetes (which is determined in part by the brain’s requirement for glucose) can be fulfilled by the body’s metabolic processes with include glycogenolysis, gluconeogenesis, and/or ketogensis in the setting of very low dietary carbohydrate intake.
Note: This previous article outlines the ADA’s updated position that the brain’s need for glucose can be fulfilled by the body.
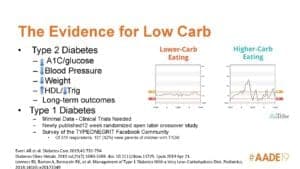
Slide 5 – The Evidence for Low Carb in Type 2 Diabetes and Type 1 Diabetes
Speaking Point Summary
- Low carb and very low carb eating patterns are among the most studied eating patterns for type 2 diabetes (T2D).
- Long-term outcomes of Virta Health’s 2-year data published in May 2019 were not included in the new ADA Consensus Report.
- For those with type 1 diabetes (T1D), no trials met the inclusion criteria for the ADA’s Consensus Report, however one small study limited carbs to 47 grams per day, and another limited carbs to 75 grams per day with positive results relating less glycemic variability, and lower HbA1C respectively.
- The ADA Consensus Report states that this evidence suggests that a very low carb eating pattern may have potential benefits for adults with type 1 diabetes, but clinical trials of sufficient size and duration are needed to confirm prior findings.
From 2019 Standards of Care
- Providers should maintain consistent medical oversight and recognize that certain groups are not appropriate for low-carbohydrate eating plans, including pregnant or lactating women, children, people who have renal disease or disordered eating behavior.
- Low carb and very low carb eating plans should be used with caution for those taking SGLT2 inhibitors due to potential risk of ketoacidosis.
- There is inadequate research about dietary patterns for type 1 diabetes to support one eating plan over another at this time.
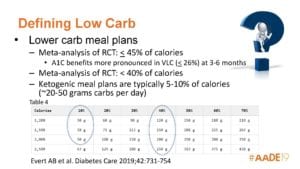 Slide 6 – Different Ways to Define “Low Carb”
Slide 6 – Different Ways to Define “Low Carb”
Speaking Points Summary
In the ADA’s Consensus Report, Nutrition Therapy for Adults included 2 meta-analysis where “low carb” was defined differently (≤ 45% calories, < 40% of calories) and 1 meta analysis where “ketogenic” was defined as 5-10% calories / ~20-50 grams carbohydrate per day.
In general, the presenters define “low carb” as being ~50 – 130 grams carbs per day, since < 50 grams of carbs could be a ketogenic for some people.
Feinman et al defined three categories of reduced-carbohydrate diets:
(a) very low carbohydrate ketogenic: carbs limited to 20—50 g per day or < 10% of total energy intake.
(b) low carbohydrate: carbs limited to < 130 g per day or < 26% of total energy intake.
(c) moderate carbohydrate: carbs limited to 130—225 g per day or 26—45% of total energy intake.
(Feinman RD, Pogozelski WK, Astrup A, Bernstein RK, Fine EJ,Westman EC, et al. Dietary Carbohydrate Restriction as the First Approach in Diabetes Management: critical review and evidence base. Nutrition. 2015;31(1):1—13.)
 Slide 7 – Teaching Low Carb
Slide 7 – Teaching Low Carb
Speaking Points Summary
- Food Lists: customize to each patient / client. Some people prefer to stop buying / eating certain foods which automatically limits their carb choices, e.g. they don’t want to buy bread or keep it in the house
- Carb Counting: could vary and be personalized depending on the client / patient’s post-prandial (after meal) glucose responses, e.g. up to ___ carbs per day versus set number of carbs at each meal
- Food Label Reading: focusing on carbs and/or sugars in the ingredient list
- Track Macros: use of an app such as MyFitnessPal or CarbManager, can be individualized to be gluten free, Mediterranean, etc.
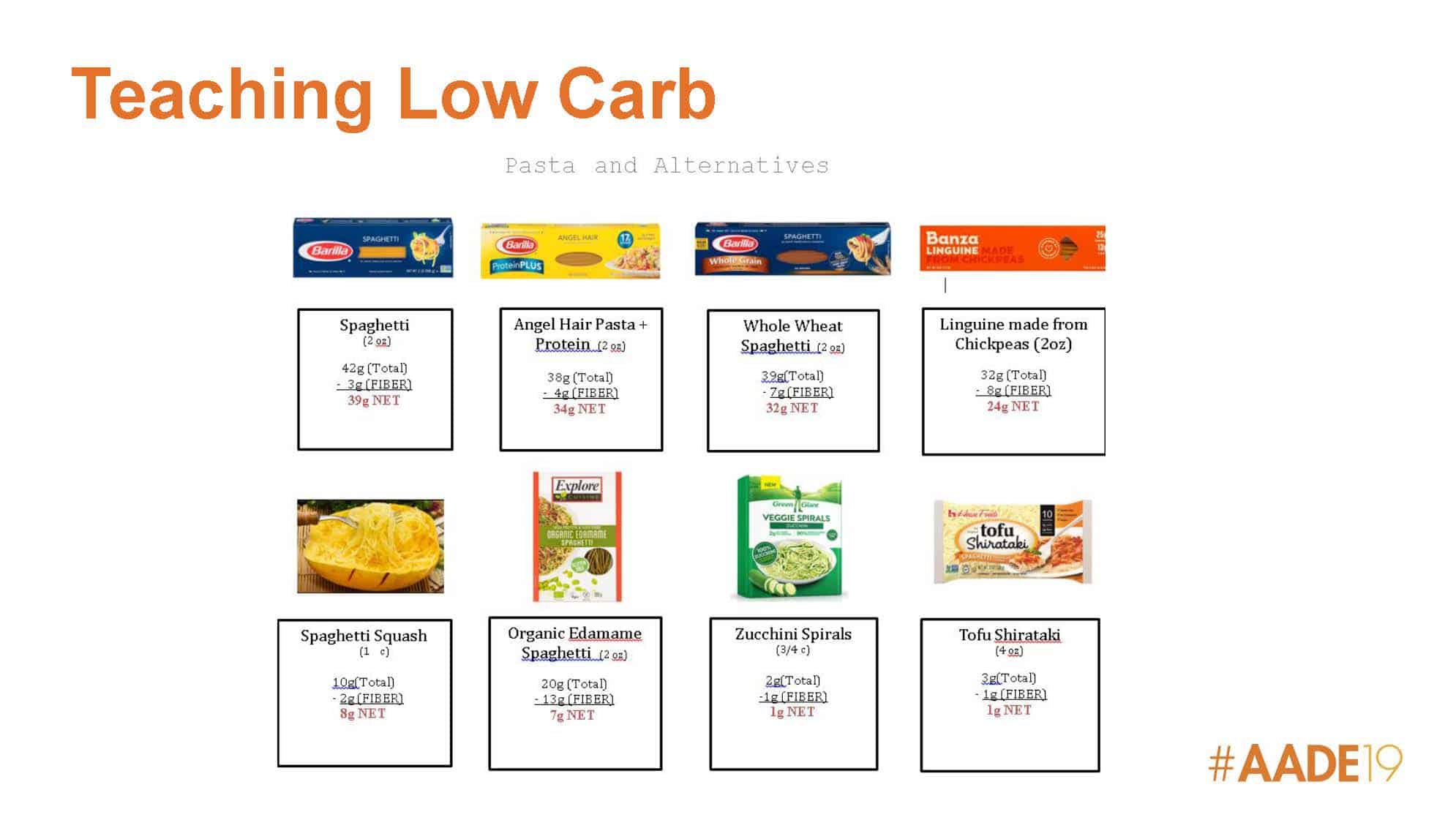
Slide 8 – Teaching Low Carb (cont’d) – shows a handout used in practice to show lower carb options for traditional pasta.

Slide 9– Teaching Low Carb – making it easy
e.g. using leftover vegetables from dinner for breakfast, sample meal plans with carb amounts, resources with recipes and pictures, no—cook put together meal ideas.
Slide 10 – Clinical Pearls for Providing Support
- real food when possible
- option when convenience is needed
- ways to make carb foods less carb-based; e.g. substituting plain yogurt with vanilla for sweetened vanilla yogurt
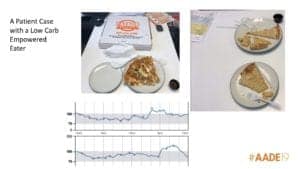
Slide 11 -Low Carb Empowered Eater
This slide gave an example of a person with diabetes who started eating lower carb on his own by using a Continuous Glucose Monitor (CGM).
i.e. eats the topping off a pizza to minimize glucose spike and is empowered to do so because he can see the results in real-time.
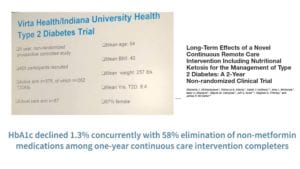
Slide 12 -Virta Health Type 2 Diabetes Trial was not included in the ADA’s Consensus Report because subjects self-selected which group they would be in, i.e. not randomized.
However, the 1-year data showed HbA1C declined 1.3% concurrently with elimination of non-metformin medications in the continuous care intervention group which is notable.
The 2-year data was published in 2019, just prior to the ADA Consensus Report but was not included.
Slide 13 – slide from Virta Health
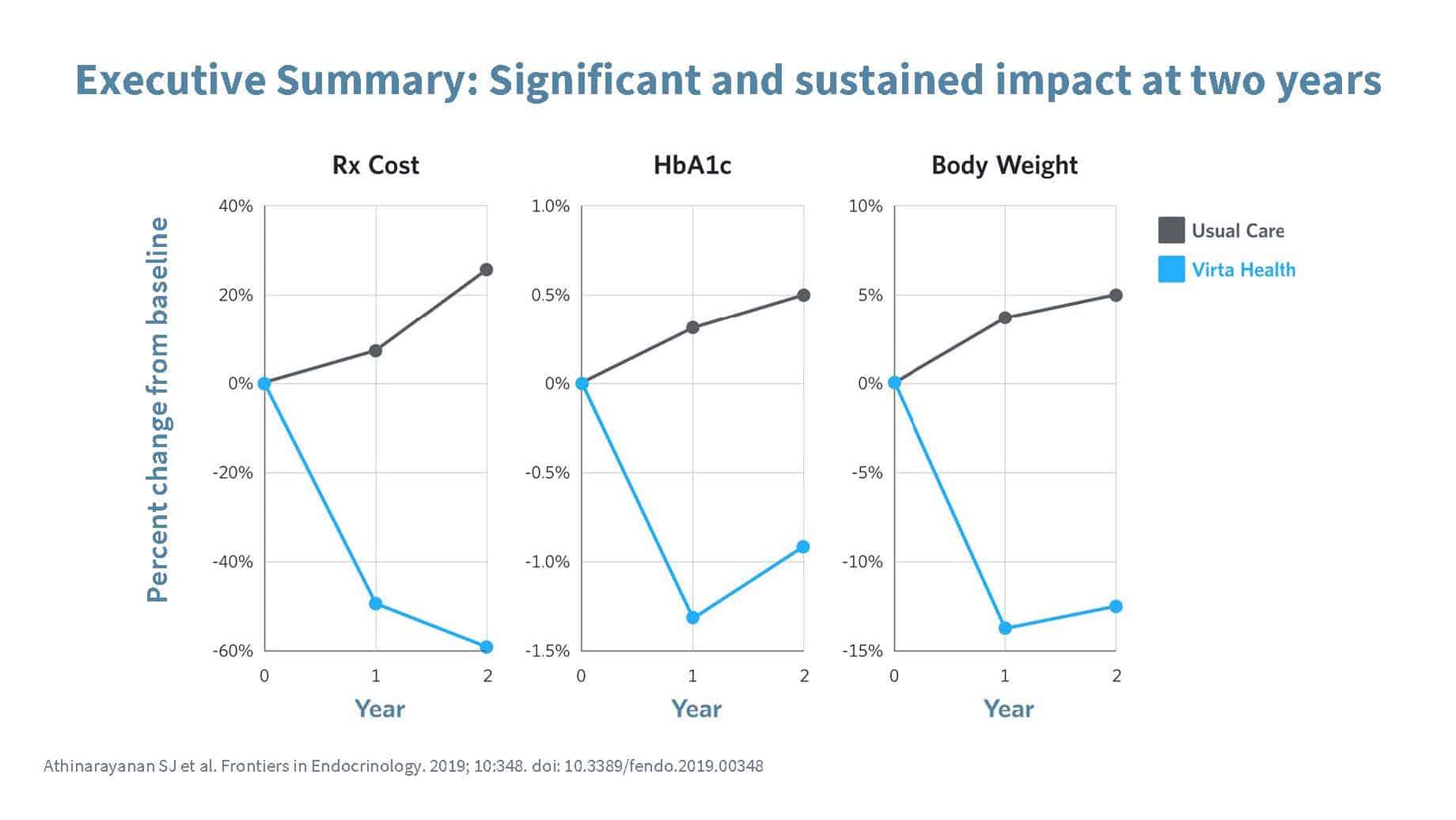
This slide represents the actual percentage point reduction in prescription (Rx) costs, HbA1C and Body Weight of intervention group compared to the usual care group.
Slide 14 – What people think “keto” is, versus what keto actually is.
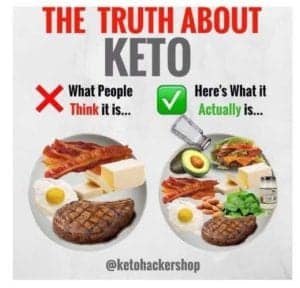 The idea here is that people think that all one eats on a ketogenic diet is meat, eggs, butter and lots of bacon, but there is a variety of foods one can eat, including vegetables, nuts, avocado (amongst other things).
The idea here is that people think that all one eats on a ketogenic diet is meat, eggs, butter and lots of bacon, but there is a variety of foods one can eat, including vegetables, nuts, avocado (amongst other things).
Slide 15 – 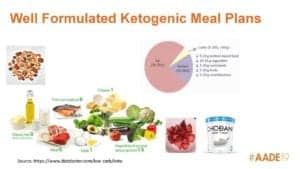 Well Formulated Ketogenic Meal Plans
Well Formulated Ketogenic Meal Plans
A well formulated, ketogenic meal plans can be a great way for people to learn to eat whole, less-processed, and plant foods such as vegetables, nuts and olives and to learn about carbohydrates; a win-win for people with diabetes.
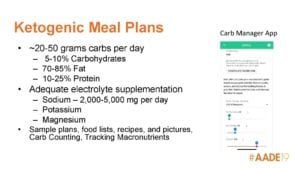
Slide 16 – Ketogenic Meal Plans
- 20-50 grams carbs per day: 5-10% carbohydrate, 70-85% fat*, 10-25% protein*
[*Note: this is not the only way to define a “ketogenic diet”, but the one the presenters use. Some clinicians use a higher protein/lower fat approach. What makes a diet ketogenic is the number of grams of carbs being ; 50 g per day or less, for men / 35 g of carbs per day or less, for women.]
- adequate electrolyte supplementation: sodium; 2,000-5,000 mg per day, plus potassium, magnesium
- can include sample plans, food lists, recipes, pictures, carb counting, tracking macros
 Slide 17 – Ketogenic Meal Plans (cont’d)
Slide 17 – Ketogenic Meal Plans (cont’d)
Keto meal plans can be customized and individualized to the client’s / patient’s food preferences.
(e.g. gluten free, Mediterranean, etc.)
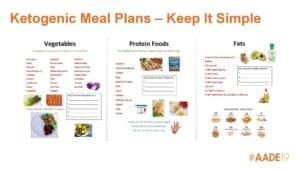
Slide 18 – Ketogenic Meal Plans – keeping it simple.
Many people benefit from basic simple food lists (eg. a “vegetable” list with types of vegetables, a place for them to list their 5 favourite types, along with some pictures).
These food lists can also be used to teach low carb eating.

Slide 19 – Examples of how to include options such as dessert, alcohol, etc. in very low carb eating plans.
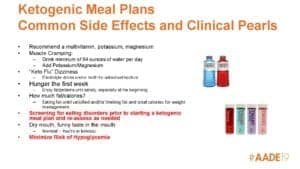
Slide 20 – Recommendations:
- supplement with multivitamin
- drink 64 oz / 2 liters water/day, add potassium / magnesium
- use electrolyte drinks or bone broth to minimize symptoms of “keto flu”
- the first week: fat / protein to satiety to address hunger
- after the first week: either eat fat until satisfied and/or limit fat and total calories for weight management*
*Note: Some clinicians encourage people to eat lean protein until satiated, then add some fat for taste. Many clinicians do not limit total calories, but focus on increasing satiety instead, as the end result will be a decrease in overall calories (as a result rather than as an input).
Slide 21 – What is an Individualized Plan (slide credit: Shamera Robinson, RDN)
The following components should all be
considered when assessing, teaching and coaching with any nutrition intervention;
- energy deficit*
- dietary preferences
- health literacy / numeracy
- resources
- food availability
- cooking skills
- disordered eating
- sustainability
*Note: Many clinicians do not create an energy deficit (i.e. do not limit total calories) but focus on increasing satiety. Increasing satiety ends up resulting in an energy deficit as a result, which some clinicians prefer over restricting calories as an input.
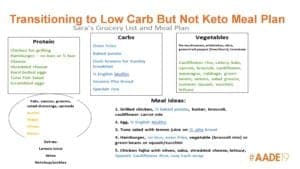
Slide 22 – Transitioning to a Low Carb (from a Keto) Meal Plan
- Some people will not want to do very low carb / keto diet forever and/or may benefit from taking planned breaks
- this requires a period of transitioning from a ketogenic meal plan to other meal plan (e.g. low carb), depending on client / patient’s wishes/needs
- transition should be customized to the individual
- can be a mixture of carbohydrate food (e.g. 1/2 baked potato*, 1/2 pita bread*) along with low-carb alternatives (e.g. cauliflower “rice”, zucchini “zoodles”)
* Note: in this type of case, some clinicians would recommend low Glycemic Index / high fiber carbohydrates such as winter squash or peas, instead of potato or bread.
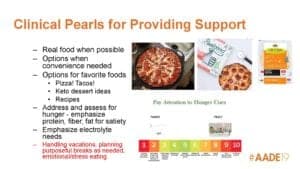
Slide 23 – Clinical Pearls for Providing Support
- aim for real food when possible
- convenience options could be protein shakes, pre-portioned cheese or nuts, ready-made mashed cauliflower, ready-made low-carb pizza or low carb wraps
- emphasize protein, fiber, fat for satiety, electrolyte needs
- keto dessert ideas
- how to handle vacations, emotional / stress eating
- consider incorporating “mindful eating” / “intuitive eating”; rating hunger levels to teach clients to listen to their bodies, eat when they are hungry and stop when full*, etc.
*Note: this approach may not be suitable for those with very high insulin levels that drive food cravings, or addiction to specific foods.
Part B: Pharmacology Approach – Diana Isaacs, PharmaD, CDE

Slide 24 – Medication Adjustment for Low Carb Eating
Slide 25 – ADA Consensus Report nutrition guidelines
- adopting a very low carb eating plan can cause increased production of urine (diuresis) and a rapid reduction in blood glucose
- consultation with a knowledgeable practitioner at the onset is necessary to prevent dehydration, reduce injected insulin and blood sugar lowering medications in order to prevent hypoglycemia (low blood sugar)
(Evert AB et al. Diabetes Care 2019; 43: 731-754.)
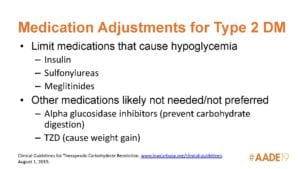
Slide 26 – Medication Adjustments for Type 2 Diabetes (T2D)
The first speaking point was to confirm that the patient is truly a type 2 diabetic
i.e. not LADA (Latent Autoimmune Diabetes of Adulthood) which is a form of type 1 diabetes that develops later into adulthood
Medication Adjustments for Type 2 Diabetes (T2D)
- limit medications that cause hypoglycemia, such as insulin, sulfonylureas, meglitinides (more on that below)
- other medication likely not needed / not preferred: alpha glucosidase inhibitors (prevent carb digestion), thiazolidinediones (TzD), also known as glitazones (more on that below)
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines)
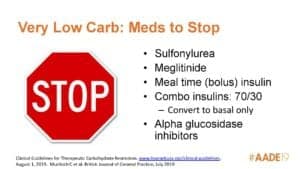
Slide 27 – Medications to Stop on a Very Low Carbohydrate Diet
- sulfonylurea, increase insulin release e.g. GlyburideⓇ
- meglitinide (also called glinides), e.g. PrandinⓇ
- bolus (meal time) insulin
- combo insulins: 70/30, convert to basal only
- alpha glucosidase inhibitors (acarbose), prevent carbohydrate absorption, e.g. GlucobayⓇ
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines), Murdoch C et al, British Journal of General Practice, July 2019)
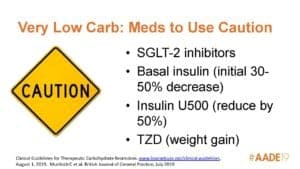 Slide 28 – Medications to Use Caution on a Very Low Carbohydrate Diet
Slide 28 – Medications to Use Caution on a Very Low Carbohydrate Diet
- Sodium-glucose co-transporter protein 2 inhibitors SGLT-2 inhibitors (also called gliflozins), e.g. InvokanaⓇ, JardianceⓇ
- basal insulin (initial 30-50% decrease)
- insulin U500: cut dose in half
- thiazolidinediones (TzD), also known as glitazones (risk of weight gain)
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines), Murdoch C et al, British Journal of General Practice, July 2019)
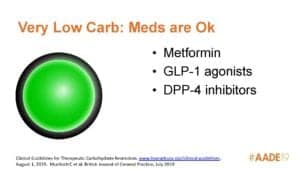 Slide 29 – Medications that are Okay to Use on a Very Low Carbohydrate Diet
Slide 29 – Medications that are Okay to Use on a Very Low Carbohydrate Diet
- MetforminⓇ
- Glucagon-like peptide 1 inhibitors (GLP-1 agonists) e.g. VictozaⓇ, SaxendaⓇ
- Dipeptidyl peptidase 4 inhibitors (DPP-4 inhibitors) e.g. JanuviaⓇ
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines, Murdoch C et al, British Journal of General Practice, July 2019)
Slide 30 – Medications Adjustments for Type 1 Diabetes on a Low Carbohydrate Diet
- bolus insulin: may need to intensify carb ratio, ? bolus for protein
- monitor ketones
- avoid sodium-glucose co-transporter protein 2 inhibitors (SGLT-2 inhibitors), also called gliflozins, e.g. InvokanaⓇ, JardianceⓇ
- caution with hybrid closed loop pumps
- close follow-up required
(Eisworth M et al, Endocrinol Diabetes Metab Case Rep 2018, 2018:18-0002, Krebs JD et al, Asia Pacific Journal of Clinical Nutrt 2016 25:78-84, Nielsen JV et al Upsala Journal of Medical Sciences 2005; 110 267-273)
Slide 31 – Blood Pressure Medications
- important to keep in mind the initial diuretic effect of a low carb or very low carb diet
- consider cutting dosage in half or stopping diuretic (e.g. HCTZ or chlorthalidone)
- monitor blood pressure
(Hussain TA et al, Nutrition 28 (2012) 1016-1021, Evert AB et al. Diabetes Care 2019; 43: 731-754.)
Slide 32 – Other Concerns
- drink > 2 liters (64 oz /) water/day
- to avoid muscle cramps, supplement magnesium 200-400 mg/day
- watch for deficiency in vitamin K, sodium, chloride, vitamin B12, folate, calcium, vitamin D
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines)
Note: Slide 33 and Slide 34 were part of a case study of a 52 year old woman with T2D along with several co-morbid conditions, and on multiple medications who planned to start a ketogenic diet the follow day. The case study reviewed the medications that should be stopped or the dosage changed, and what her new medication regimen would look like. They are not included here.
Many thanks once again to Dawn Noe, RDN, CDE and her colleague Diana Isaacs, PharmaD, CDE for sharing their slides and speaking points with us.
More Info?
Please note that I am not a CDE and as a result do not provide clinical services to those with type 1 diabetes, or to those with type 2 diabetes who are currently on insulin or insulin-analogue.
For those with T2D who have only been recently prescribed insulin, I have experience working with people’s endocrinologists and GPs as they seek to transition over to a low carbohydrate / ketogenic diet to manage and treat their diabetes.
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchf-rd/
Instagram: https://www.instagram.com/lchf_rd
Fipboard: http://flip.it/ynX-aq
Copyright ©2019 The Low Carb Healthy Fat Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Share to Flipboard:
