
This weekend, thousands of American Certified Diabetes Educators (CDE) gathered at the American Association of Diabetes Educators (AADEs) annual conference in Houston, Texas.
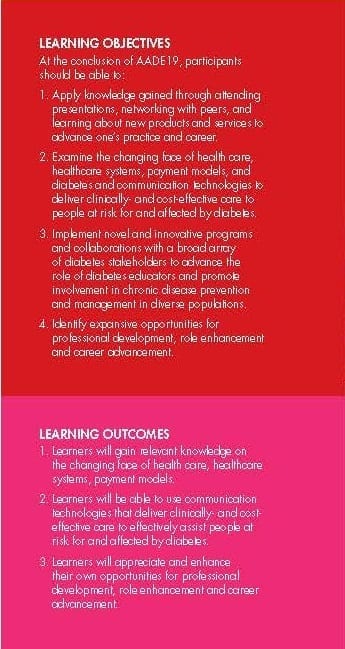
One of the Learning Objectives of the conference was for CDEs to learn how to implement novel and innovative ways to advance chronic disease prevention and management, and one of those novel ways was through the use of a Low Carbohydrate Diet.
CDEs are healthcare professionals from a variety of backgrounds who are specialized in diabetes prevention and management and include Registered Dietitians, Registered Nurses, Pharmacists, Physician Assistants and Nurse Practitioners.
This is very exciting news indeed!
It means that CDEs are now learning how to implement the American Diabetes Association’s (ADA) new 2019 Standards of Medical Care in Diabetes that was released this past December, and which includes use of a low carbohydrate diet (you can read more about that here).
This conference provided education to enable CDEs to apply the content of the ADA’s April 18, 2019 Consensus Report which added the use of a very low carbohydrate (ketogenic) diet of 20-50 grams of carbs to the choice of meal patterns to manage both type 1 and type 2 diabetes. You can read more about the Consensus Report here.
Two Educational Sessions on Use of a Low Carbohydrate Diet
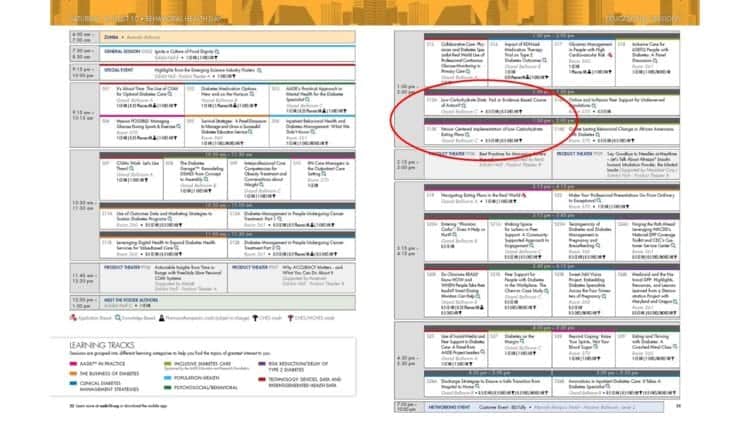
Saturday, August 11, 2019 there were two Educational Sessions at the AADE 2019 Annual Conference related to therapeutic use of a low carbohydrate diet.
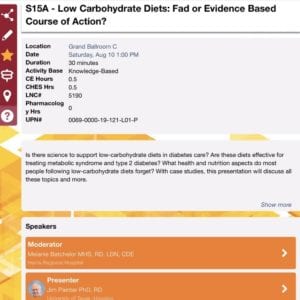
The first session was titled Low Carbohydrate Diets; Fad or Evidence Based Course of Action and was given by Dr. Jim Painter, PhD, RD and Professor Emeritus from Eastern Illinois University, in Charleston, Illinois.
The second session was titled Person-Centered Implementation of Low Carbohydrate Eating Plans and was given by Diana Isaacs, PharmaD, CDE and Dawn Noe, RD, CDE both from Cleveland Clinic Diabetes Center. Link to this presentation, including the slides and speaking notes is at the bottom or this article.
This post is a summary of Dr. Jim Painter’s educational session at the AADE’s 2019 Annual Conference titled Low Carbohydrate Diets; Fad or Evidence Based Course of Action.
Note: Photos of the slides were posted on Twitter® on August 10, 2019 by Jake Kushner, MD (@JakeKushnerMD).
Low Carbohydrate Diets: Fad or Evidence Based Course of Action
Slide 1
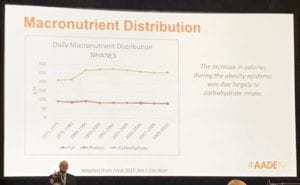
Dr. Painter’s first slide demonstrates using National Health and Nutrition Examination Survey (NHANES) data (adapted from Ford 2015 Am J Clin Nutr) how carbohydrate content of the US diet increased dramatically after 1980 and continued high, while protein content (and fat content, not visible in this slide) remained stable.
“The increase in calories during the obesity epidemic was due largely to carbohydrate intake.“
Slide 2
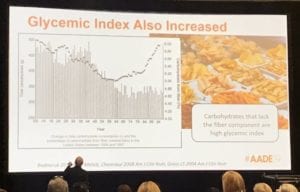 Dr. Painter’s second slide pointed out that not only did carbohydrate consumption increase (dotted graph), the percentage of carbohydrate from fiber decreased (bar graph).
Dr. Painter’s second slide pointed out that not only did carbohydrate consumption increase (dotted graph), the percentage of carbohydrate from fiber decreased (bar graph).
The point Dr. Painter made is that “carbohydrates that lack fiber are high glycemic index” carbs — and these highly refined carbs result in a higher increase in blood sugar than carbohydrates that contain fiber.
Slide 3
Dr. Painter then defined what a “low carbohydrate diet” is according to the American Diabetes Association and the Academy of Nutrition and Dietetics.
What is a low-carbohydrate diet?
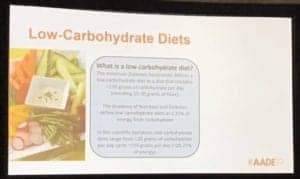
The American Diabetes Association defines a low-carbohydrate diet as a diet that contains < 130 grams of carbohydrate per day (including 25-30 grams of fiber)
i.e. ~100-105 net grams of carbs
Note: Dr. Painter didn’t define a very low carbohydrate diet, which the American Diabetes Association defined in its new Consensus Report as 20-50 g carbs per day. You can read more about that here.
The Academy of Nutrition and Dietetics defined low carbohydrate diets as ≤ 35% of energy from carbohydrates.
In the scientific literature, low-carbohydrate diets range from 20 grams of carbohydrate per day up to ~150 grams per day (~20-25% of energy).
Slide 4
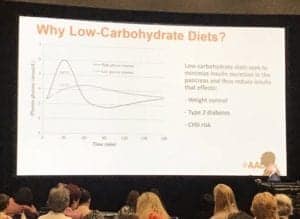 Dr. Painter then explained how low carbohydrate diets seek to minimize insulin secretion in the pancreas via their very low glycemic response, and how the reduced insulin affects;
Dr. Painter then explained how low carbohydrate diets seek to minimize insulin secretion in the pancreas via their very low glycemic response, and how the reduced insulin affects;
- weight control
- type 2 diabetes
- coronary heart disease (CHD)
Slide 5
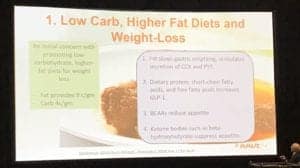 Dr. Painter explained how an initial concern with a low carbohydrate diet was with the higher fat aspect, particularly for weight loss, as fat provides 9 kcals / gram and carbs only provides 4 kcals/grams, however;
Dr. Painter explained how an initial concern with a low carbohydrate diet was with the higher fat aspect, particularly for weight loss, as fat provides 9 kcals / gram and carbs only provides 4 kcals/grams, however;
- Fat slow gastric emptying and stimulates the secretion of cholecystokinin (CCK) and Peptide YY (PYY) — which are satiety hormones that result in people feeling full.
- Dietary proteins, short chain fatty acids and free fatty acids increase GLP-1 (which is one of the incretin hormones). Glucagon-like Peptide-1 (GLP-1) acts on the brain to decrease appetite, increase satiety (feeling full) and decrease food intake. You can read more about that here.
- Branched Chain Amino Acides (BCAA) found in protein reduces appetite.
- Ketone bodies (produced in very low carbohydrate diets) such as beta-hydroxybuterate suppress appetite.
Slide 6
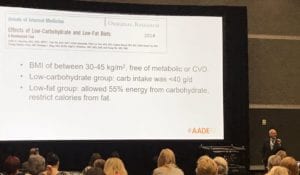 Dr. Painter then outlined the findings of a 2014 study titled Effects of low-carbohydrate and low-fat diets: a randomized trial (Baranna LA, Hu T, Reynalds K et al, Ann Intern Med. 2014 Sep 2;161(5):309-18. doi: 10.7326/M14-0180).
Dr. Painter then outlined the findings of a 2014 study titled Effects of low-carbohydrate and low-fat diets: a randomized trial (Baranna LA, Hu T, Reynalds K et al, Ann Intern Med. 2014 Sep 2;161(5):309-18. doi: 10.7326/M14-0180).
Participants in this study had a BMI of between 30-45 kg per meter squared (meaning they were obese to morbidly obese), but did not have any metabolic diseases such as diabetes or cardiovascular disease (CVD).
The low carb group had carbohydrate intake of < 40 grams/day and the low fat group was allowed 55% of energy from carbohydrate (which is with the Recommended Dietary Intake of 45-55%), but restricted calories from fat.
There were 59-60 participants in both the low carb or low fat group…
Slide 7
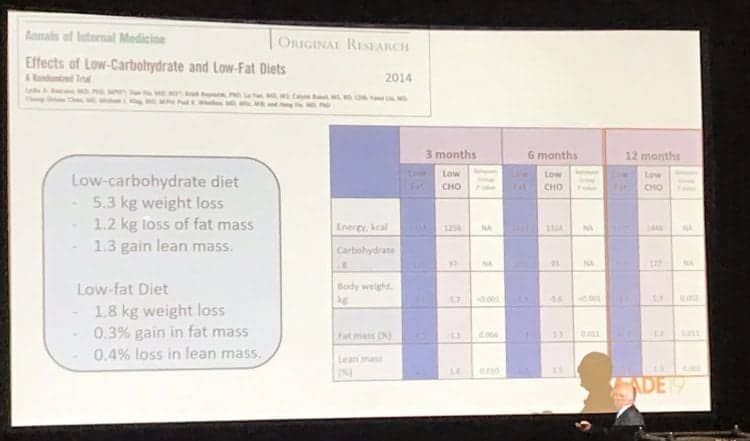
…and after a year, those in the low carb group had a greater decrease in weight, fat mass, ratio of total-high-density lipoprotein (HDL) cholesterol, triglyceride level, and greater increases in HDL cholesterol level than those on the low-fat diet.
Dr. Painter highlighted that at the end of 12 months; these were the results of the two groups;
Low-carbohydrate diet
- 5.3 kg weight loss
- 1.2 kg loss of fat mass
- 1.3 gain lean body mass
Low-fat diet
- 1.8 kg weight loss
- 0.3% gain in fat mass
- 0.4% loss in lean mass
Slide 8
 Dr. Painter then went over the results from a 2006 study by Gannon MC and Nutall FQ, titled Control of Blood Glucose in Type 2 Diabetes Without Weight Loss by Modification of Diet Composition (Nutr Metab. (2006 Mar 23;3:16. doi: 10.1186/1743-7075-3-16) which found that even without weight loss, altering the diet composition to a low carb diet (carbs < 20% of energy) can enable people with type 2 diabetes to lower their blood sugar level without weight loss or diabetes medications, and achieve significantly better glycated hemoglobin (HbA1C) levels.
Dr. Painter then went over the results from a 2006 study by Gannon MC and Nutall FQ, titled Control of Blood Glucose in Type 2 Diabetes Without Weight Loss by Modification of Diet Composition (Nutr Metab. (2006 Mar 23;3:16. doi: 10.1186/1743-7075-3-16) which found that even without weight loss, altering the diet composition to a low carb diet (carbs < 20% of energy) can enable people with type 2 diabetes to lower their blood sugar level without weight loss or diabetes medications, and achieve significantly better glycated hemoglobin (HbA1C) levels.
Slide 9
 In this slide, Dr. Painter addressed a prevailing concern among many healthcare professionals that a low carbohydrate diet increase cardiovascular disease risk.
In this slide, Dr. Painter addressed a prevailing concern among many healthcare professionals that a low carbohydrate diet increase cardiovascular disease risk.
Does a Low-Carbohydrate Intake Increase Cardiovascular Disease Risk?
Dr. Painter outlined that a 2017 by Chui demonstrated that HDL cholesterol increases in a low carb diet and that while LDL cholesterol does increase, it tends to be the large buoyant LDL that increase, with no change in the athlersclerotic small, dense LDL.
He also outlined that a 2012 meta-study analysis of 19 randomized control trials (RCTs) by Santos et al reported a global decrease in triglyceride levels of 29.71 mg/dL (0.34 mmol/L) and that a 2014 study by Bazzano reported that a low carbohydrate diet had a greater decrease in 10-year cardiovascular heart disease (CHD) risk score based on the Framingham Risk Score, than those on the low fat diet.
Slide 10
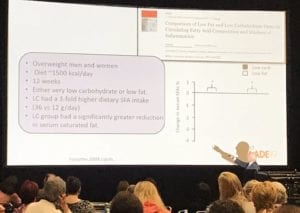 Dr. Painter then elaborated on a study from 2008 by Forsythe CE et al titled Comparison of Low Fat and Low Carbohydrate Diets on Circulating Fatty Acid Composition and Markers of Inflammation that was published in the Journal Lipids (Lipids. 2008 Jan;43(1):65-77. Epub 2007 Nov 29).
Dr. Painter then elaborated on a study from 2008 by Forsythe CE et al titled Comparison of Low Fat and Low Carbohydrate Diets on Circulating Fatty Acid Composition and Markers of Inflammation that was published in the Journal Lipids (Lipids. 2008 Jan;43(1):65-77. Epub 2007 Nov 29).
In this study overweight men and women were put on either a low carb or low fat ~1500 kcal / day diet for 12 weeks. Results indicated that the low carb diet had a 3-fold higher dietary intake of saturated fatty acids (SFA) (36 grams/day versus 12 grams/day) yet the low carb group had a significantly greater reduction in their serum saturated fat levels.
That is, people in the low carb group they ate 3x the amount of saturated fat yet had a significantly greater reduction in their blood levels of saturated fat.
Slide 11
 Dr. Painter then reviewed a 2004 study by Volek JS et al titled Dietary Carbohydrate Restriction Induces a Unique Metabolic State Positively Affecting Atherogenic Dyslipidemia, Fatty Acid Partitioning, and Metabolic Syndrome which indicated how a very low carbohydrate (VLCKD) compared to a low carbohydrate diet (LCD) significantly improved body mass, abdominal fat, triglycerides (TG), ApoB:ApoA1 ratio, small dense LDL, TG:HDL ratio, insulin levels, and HOMA-IR score.
Dr. Painter then reviewed a 2004 study by Volek JS et al titled Dietary Carbohydrate Restriction Induces a Unique Metabolic State Positively Affecting Atherogenic Dyslipidemia, Fatty Acid Partitioning, and Metabolic Syndrome which indicated how a very low carbohydrate (VLCKD) compared to a low carbohydrate diet (LCD) significantly improved body mass, abdominal fat, triglycerides (TG), ApoB:ApoA1 ratio, small dense LDL, TG:HDL ratio, insulin levels, and HOMA-IR score.
Slide 12
 Dr. Painter then looked at the “why” for using a low carbohydrate diet for type 2 Diabetes Mellitus (T2DM).
Dr. Painter then looked at the “why” for using a low carbohydrate diet for type 2 Diabetes Mellitus (T2DM).
Dr. Painter outlined the results of a 2015 study titled Prevalence of and Trends in Diabetes Among Adults in the United States, 1988-2012 by Menke A et al (JAMA. 2015 Sep 8;314(10):1021-9. doi: 10.1001/jama.2015.10029) which indicated that;
“Recent data indicates 52% of the American population is either diabetic or prediabetic. The cost of diabetes (in the US) is estimated to be over $320 billion annually”.
Slide 13
 Dr. Painter then cited a 2013 systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes (Ajala et al) titled Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes, Am J Clin Nutr. 2013 Mar;97(3):505-16. doi: 10.3945/ajcn.112.042457. Epub 2013 Jan 30.).
Dr. Painter then cited a 2013 systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes (Ajala et al) titled Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes, Am J Clin Nutr. 2013 Mar;97(3):505-16. doi: 10.3945/ajcn.112.042457. Epub 2013 Jan 30.).
This paper looked at 20 randomized control trials (RCTs) across 3460 randomly assigned subjects and which found that a low-carbohydrate diet, low-GI diet, Mediterranean diet, and high-protein diet all led to a greater improvement in glycemic control and with the low-carbohydrate diet and Mediterranean diet leading to greater weight loss.
Dr. Painter indicated that each of these dietary philosophies show effectiveness of lower carbohydrate and lower GI diets for treating T2DM.
Slide 14
Dr. Painter then outlined the findings of a 2017 study by Snorgaard O et al titled Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes (
“Upon subgroup analysis, it was found that carbohydrate of < 26% of energy produces the greatest reduction whereas carbohydrate reduction of 26-45% of total energy produces no additional benefit over low-fat diets.”
Slide 15
 In Dr. Painter’s next slide, he summarized the finding of a 2018 systematic review and meta-study paper by Sainsbury E et al with respect to medication use, titled Effect of Dietary Carbohydrate Restriction on Glycemic Control in Adults with Diabetes: A systematic review and meta-analysis (Diabetes Res Clin Pract. 2018 May;139:239-252. doi: 10.1016/j.diabres.2018.02.026. Epub 2018 Mar 6).
In Dr. Painter’s next slide, he summarized the finding of a 2018 systematic review and meta-study paper by Sainsbury E et al with respect to medication use, titled Effect of Dietary Carbohydrate Restriction on Glycemic Control in Adults with Diabetes: A systematic review and meta-analysis (Diabetes Res Clin Pract. 2018 May;139:239-252. doi: 10.1016/j.diabres.2018.02.026. Epub 2018 Mar 6).
“There was a greater reduction in medication use for participants on carbohydrate-restricted diets compared with high carbohydrate diets at every time point.”
- reduced the dosage of oral medication and/or insulin
- or an elimination of medication
Sainsbury 2018
Slide 16
 Dr. Painter then outlined some highlights of a 2015 review paper titled Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base by Feinman RD, et al; namely;
Dr. Painter then outlined some highlights of a 2015 review paper titled Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base by Feinman RD, et al; namely;
- The benefits of carbohydrate restriction in diabetes are immediate and well- documented
- Dietary carbohydrate restriction reliably reduces high blood glucose, does not require weight loss…and leads to the reduction or elimination of medication.
Slide 17
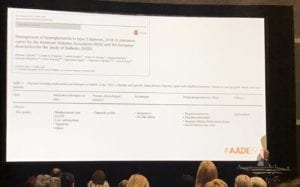 Dr. Painter next slide highlighted Table 2 from the consensus report of October 2018 by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) where they classified a low carbohydrate diet as Medical Nutrition Therapy (covered in this previous article). Table 2 outlines the full range of therapeutic options, including lifestyle management, medication and obesity management and lists a low carbohydrate diet as one of the available therapeutic diets.
Dr. Painter next slide highlighted Table 2 from the consensus report of October 2018 by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) where they classified a low carbohydrate diet as Medical Nutrition Therapy (covered in this previous article). Table 2 outlines the full range of therapeutic options, including lifestyle management, medication and obesity management and lists a low carbohydrate diet as one of the available therapeutic diets.

Slide 18
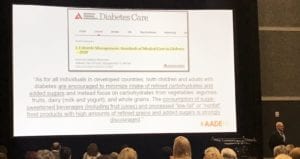 Dr. Painter then went over the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes which was released on December 17, 2018 (covered in this previous article) and which outlined key recommendations regardless which of the different types of approved eating patterns people choose, namely;
Dr. Painter then went over the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes which was released on December 17, 2018 (covered in this previous article) and which outlined key recommendations regardless which of the different types of approved eating patterns people choose, namely;
“As for all individuals in developed countries, both children and adults with diabetes are encouraged to minimize intake of refined carbohydrate and added sugars and instead focus on carbohydrate from vegetables, legumes, fruit, dairy (milk and yogurt) and whole grains. The consumption of sugar-sweetened beverages (including fruit juices) and processed “low fat” or “non-fat” food products with high amounts of refined grains and added sugars is strongly discouraged.”
Slide 19
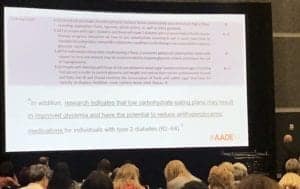 The next slide was a continuation from the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes, and Dr. Painter highlighted that;
The next slide was a continuation from the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes, and Dr. Painter highlighted that;
“In addition, research indicates that low carbohydrate eating plans may result in improved glycemia and have the potential to reduce anti-hyperglycemic medications for individuals with type 2 diabetes.”
Slide 20
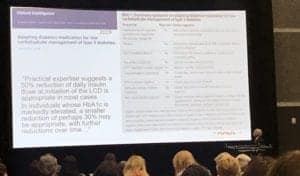 Dr. Painter next highlighted the necessity of medication adjustment soon after initiating a low carbohydrate diet in order to prevent hypoglycemia.
Dr. Painter next highlighted the necessity of medication adjustment soon after initiating a low carbohydrate diet in order to prevent hypoglycemia.
Box 1 from Adapting Diabetes Medication for Low Carbohydrate Management of Type 2 Diabetes: a practical guide by Murdoch C et al (2019), was presented and is as follows;
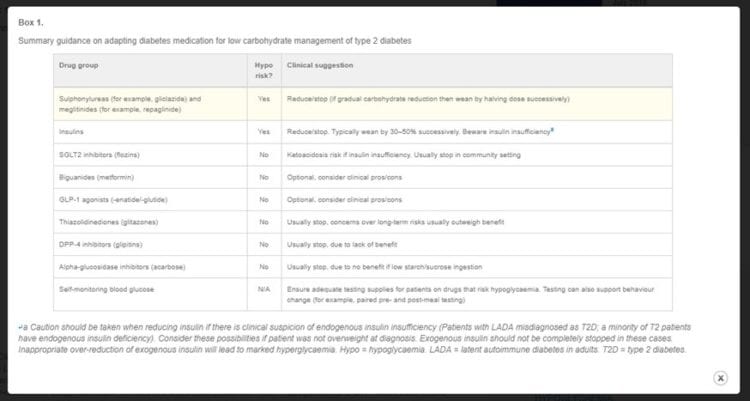
Dr. Painter highlighted the following on his slide;
“Practice expertise suggests a 50% reduction of daily insulin dose at initiation of the low carbohydrate diet (LCD) is appropriate in most cases. In individuals whose HbA1C is markedly elevated, a smaller reduction of perhaps 30% may be appropriate, with further reductions over time…”
Slide 21
 Dr. Painter’s next slide simply read;
Dr. Painter’s next slide simply read;
“Be encouraged! Reversal of Type 2 Diabetes??”
…as if to challenge his listeners to consider that diabetes reversal using a low carbohydrate diet is possible.
Slide 22
 Dr. Painter then reviewed the DiRECT randomized control trial by Lean et al, titled Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial (The Lancet, 391 (10120). pp. 541-551. ISSN 0140-6736).
Dr. Painter then reviewed the DiRECT randomized control trial by Lean et al, titled Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial (The Lancet, 391 (10120). pp. 541-551. ISSN 0140-6736).
In that study, the 300+ participants from almost 50 primary care sites in the UK were randomly assigned to either a weight management program (which was the intervention group) or to best-practice care by guidelines (which was the control group).
Slide 23
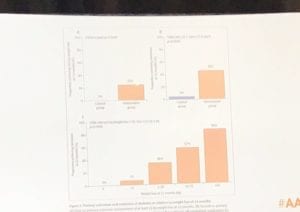 Dr. Painter outlined the results of the DiRECT trial, which found that at 12 months, 24% of the participants in the intervention group lost 15 kg or more, with no weight loss in the control group.
Dr. Painter outlined the results of the DiRECT trial, which found that at 12 months, 24% of the participants in the intervention group lost 15 kg or more, with no weight loss in the control group.
Diabetes remission varied with weight loss;
- no remission in those who gained weight
- 7% achieved remission with under 5 kg of weight loss
- 34% achieved remission lost between 5—10 kg
- 57% achieved remission with 10—15 kg loss
- 86% achieved remission with weight loss of 15 kg or more
“Our findings show that, at 12 months almost half of participants achieved remission to a non-diabetic state and off anti-diabetic drugs. Remission of type 2 diabetes is a practical target for primary care“.
Slide 24
 Dr. Painter then proceeded to addressed 3 common misperceptions about low carbohydrate diets, namely;
Dr. Painter then proceeded to addressed 3 common misperceptions about low carbohydrate diets, namely;
- A low carbohydrate diet puts participants at risk of ketoacidosis…
- Low carbohydrate diets ignore the principles of moderation and result in a nutrient-deficient diet…
- The majority of weight loss comes from water and lean body mass…
Slide 25 – addressing the misperception that a low carbohydrate diet puts participants at risk of ketoacidosis…
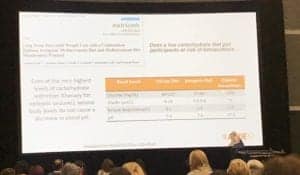 Dr. Painter cited a 2013 study titled Long Term Successful Weight Loss with a Combination Biphasic Ketogenic Mediterranean diet and Mediterranean Diet Maintenance Protocol by Paoli A et al (Nutrients. 2013 Dec 18;5(12):5205-17. doi: 10.3390/nu5125205).
Dr. Painter cited a 2013 study titled Long Term Successful Weight Loss with a Combination Biphasic Ketogenic Mediterranean diet and Mediterranean Diet Maintenance Protocol by Paoli A et al (Nutrients. 2013 Dec 18;5(12):5205-17. doi: 10.3390/nu5125205).
Using the data from that study, Dr. Painter demonstrated how the glucose range, insulin rang and ketone body range in a ketogenic diet is nothing like the ranges in Diabetic Ketoacidosis.
Normal Diet
Glucose (mg/dl) 80-100
Insulin (uU/L) 6-23
Ketone Bodies (mmol/L) 0.1
Ketogenic Diet
Glucose (mg/dl) 65-80
Insulin (uU/L) 5.5-9.4
Ketone Bodies (mmol/L) 1-8
Diabetic Ketoacidosis
Glucose (mg/dl) >300
Insulin (uU/L) ~0
Ketone Bodies (mmol/L) >25
Slide 26 – addressing the misperception that low carbohydrate diets ignore the principles of moderation and result in a nutrient-deficient diet…
 Dr. Painter cited the paper by Zinn C et al, titled Assessing the Nutrient Intake of a Low-Carbohydrate, High-Fat (LCHF) Diet: a hypothetical case study design and highlighted that despite macronutrient proportions not aligning with current national dietary guidelines, that when well-designed a low carbohydrate diet provides all of the essential micronutrients needed by the body.
Dr. Painter cited the paper by Zinn C et al, titled Assessing the Nutrient Intake of a Low-Carbohydrate, High-Fat (LCHF) Diet: a hypothetical case study design and highlighted that despite macronutrient proportions not aligning with current national dietary guidelines, that when well-designed a low carbohydrate diet provides all of the essential micronutrients needed by the body.
Even at the lower end of the carbohydrate spectrum, you can still get all of the essential nutrients and energy your body needs by selecting from a broad array of nutrient-dense vegetables and fruit, e.g.:
-
-
- raspberries
- strawberries
- blueberries
- tomatoes
- olives
- avocados
- plain greek yogurt
- nuts/seeds
-
“Zinn et all demonstrated that a well-planned Low-Carbohydrate, High-Fat (LCHF) meal plan can be considered micronutrient replete.”
Slide 27 – addressing the misperception that the majority of weight loss comes from water and lean body mass…
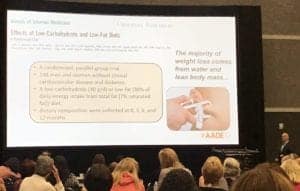 Dr. Painter cited the 2014 study by Bazzano LA et al, titled Effects of Low-Carbohydrate and Low-Fat Diets: a randomized trial which found that of the ~60 subjects randomized to either the low-carbohydrate diet (<40 grams/day) or low-fat diet (<30% of daily energy intake from total fat [<7% saturated fat]) which found that at 12 months, participants on the low-carbohydrate diet lost 3.5 kg more weight and lost 1.5% more fat mass, than those in the low-fat diet group.
Dr. Painter cited the 2014 study by Bazzano LA et al, titled Effects of Low-Carbohydrate and Low-Fat Diets: a randomized trial which found that of the ~60 subjects randomized to either the low-carbohydrate diet (<40 grams/day) or low-fat diet (<30% of daily energy intake from total fat [<7% saturated fat]) which found that at 12 months, participants on the low-carbohydrate diet lost 3.5 kg more weight and lost 1.5% more fat mass, than those in the low-fat diet group.
Slide 28
 Dr. Painter concluded his talk by saying that he feels that most low carbohydrate diets are ‘harmful in practice’ because they are low in fiber, but that that can be addressed by;
Dr. Painter concluded his talk by saying that he feels that most low carbohydrate diets are ‘harmful in practice’ because they are low in fiber, but that that can be addressed by;
- Start with a foundation of 6-8 servings of non-starchy, fiber-rich vegetables (~ 15 grams net carbs per day)
- Include additional calories from added fats. Nuts and seeds can provide additional fiber
- Depending on weight loss and healthy goals, low glycemic carbohydrates found in whole grains and fruit can be used to provide additional fiber.
For those who want to make sure to meet current fiber consumption recommendations while eating a low carbohydrate diet, please have a look at the article I wrote titled Surprising Ways to Get Adequate Fiber Eating Low Carb High Fat (LCHF), located here.
Final Thoughts…
Just a few years ago, it was viewed as quite ‘radical’ for healthcare professionals to consider a well-designed low carbohydrate or very low carbohydrate (ketogenic) diet as therapeutic, but now organizations in Europe (such as the EASD), the UK and Australia — along with the American Diabetes Association (ADA) consider both meal patterns Medical Nutrition Therapy for management of diabetes and for treating overweight and obesity.
What an exciting time!
Here it is, less than a year after the ADA released their 2019 Standards of Medical Care in Diabetes and only 4 months after the ADA released its Consensus Report and this past weekend, thousands of American Certified Diabetes Educators (CDE) gathered at their annual conference znd ~500 learned how to implement a low carbohydrate or ketogenic diet to advance chronic disease prevention and management.
It is my sincere hope that it won’t be much longer before clinicians in Canada are provided with diabetes Standards of Care that support the use of a well-designed low carbohydrate and very low carbohydrate diet as therapeutic options.
More Info?
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchf-rd/
Instagram: https://www.instagram.com/lchf_rd
Fipboard: http://flip.it/ynX-aq
UPDATE (August 16 2019): You can find the second presentation from the American Certified Diabetes Educators conference here. This is where hundreds of CDEs learned about dietary and medication management of lowcarb and ketogenic diets from a Registered Dietitian and Dr. of Pharmacy with CDE certification.
Copyright ©2019 The Low Carb Healthy Fat Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
- American Association of Diabetes Educators, Annual Conference, Houston Texas, Friday August 9 – Monday August 12, 2019, https://www.aademeeting.org/
- National Certification Board for Diabetes Educators (NCBDE), What is a CDE, https://www.ncbde.org/certification_info/what-is-a-cde/
Share to Flipboard:
