
Note (February 12, 2021): This article is provided for nutrition information only and is not an endorsement of any specific type of low carbohydrate diet. Everyone’s nutritional needs are different.
Except for specific conditions such as epilepsy, seizure disorder and glioblastoma — or for those seeking the specific benefits of high ketones, I tend to recommend a higher protein, lower fat version of a ketogenic diet when helping people with weight loss. The main reason is that for weight loss, the high fat version is normally paired with frequent- or extended-periods of fasting which, as I will outline below has some key drawbacks.
The popularized keto diet which is 75% fat has, by definition lots of added fat in the form of whipping cream, avocado, bacon and fatty meat to make up for the lower protein of 15%, as well as very low carbs (10%). While it is enticing to eat this way, ~1/3 of my clients come to me for dietary support after either failing to lose more than a little initial weight, or gaining weight. I think that is because they may have ‘missed’ that a high fat keto diet for weight loss necessarily goes along with frequent periods of fasting, but not everyone “gets” that message or even wants to ‘fast’.
Often times people will implement the ‘high fat keto diet part’ without implementing the ‘regular or extended fasting part’ — adding tons of dietary fat to food. This approach will not enable someone to reduce their own body fat stores, which is why in such cases I will recommend a slightly lower fat, higher protein approach.
Something I have observed over the last several years is that the very high fat approach often does not work well for peri- and post-menopausal women. I hypothesize that it is the change in hormones — especially estrogen at menopause that may lower metabolic rate and thus contribute to a slowing of weight loss. Combined with lots of added fat, this becomes a recipe for failure with many peri- and post-menopausal women. I’ve also noticed that in some older women, a very high fat approach triggers cravings for ‘fat bombs’ and high-fat “keto treats” and I think this may be related to the dopamine release associated with either high fat or high carb intake — and which becomes substantially higher when with foods with both fat and carbs are eaten together. Many of these women became obese eating high-fat high-carb foods, which leads me to believe that the reward-centre of the brain may be triggering that same desire via eating lots of high fat foods.
I have discovered from those who come to me after eating a high fat keto diet that they came to believe from what they’ve read online that (1) dietary fat is “the” source of satiety (no longer feeling hungry) and that (2) that when “eating “keto”, calories don’t count”.
In this article I will address these two beliefs, starting with the second.
Calories Don’t Count When Eating “Keto”
Proponents of the popularized keto diet are often heard to say that the “calories in calories out (CICO) model” is irrelevant, and that counting calories doesn’t apply “when eating keto”.
The problem is that calories are thought of as a “thing”, rather than a process. A calorie isn’t counted, but is calculated from heat and work.
A calorie was originally defined as “the amount of heat required to raise the temperature of 1 gram of water by 1° Celsius at a standard atmospheric pressure”. Since the amount of heat required to raise the temperature of 1 gram of water by 1° Celsius is known to vary by as much as 1% at different temperatures, a calorie (small “c”) is defined as “the amount of heat that will raise the temperature of 1 gram of water from 14.5° to 15.5° Celsius. This is based on the first law of thermodynamics (Law of Conservation of Energy) — that energy cannot be created or destroyed.
The number of calories in a given food is determined by burning that food in a bomb calorimeter, which is a box with two chambers, one inside the other. A sample of the food is weighed, put on a dish in the inner chamber of the calorimeter., and burned. When the food burns, if the temperature of the water goes up 1 degree Celsius per kilogram, the food is said to have 1 calorie.
As Professor Dr. Richard Feinman said recently on social media, it’s impossible to keep track of ‘grams-in of food’ and ‘grams-out of energy’ (CO2 and exhaled water) in daily life, so in that sense the “calories in calories out model” isn’t meaningful.
The law of thermodynamics doesn’t stop applying because one is eating a keto diet. In fact, when using therapeutic ketogenic diets for conditions such as epilepsy, seizure disorder and glioblastoma, diets such as the classic Ketogenic Diet (KD) with a 4:1 ratio of fat to protein, a Modified Ketogenic Diet (MKD) with a 3:1 ratio of fat to protein, and a Modified Atkins Diet (MAD) with a 2:1 ratio of fat to protein are all calculated based on the caloric needs of the individual. These high fat diets are intended to produce large amounts of ketones for therapeutic purposes and calories definitely count when following a ketogenic (keto) diet.
The popularized keto diet which is usually thought of as being ~75% fat, 15% protein and 10% carbohydrate is basically a hybrid between the Modified Ketogenic Diet (MKD) and the Modified Atkins Diet (MAD) — neither of which are weight loss diets. In fact, these diets were specifically designed to not result in weight loss. Unless the popularized high fat ‘keto’ diet is combined with frequent periods of fasting <24 hours and/or extended periods of fasting >24 hour, weight loss is unlikely to occur. This is why the two main proponents of the high fat ‘keto’ diet, Dr. Jason Fung and Diet Doctor both promote the high fat ‘keto’ diet together with periods of fasting. While many people are successful losing weight this way, the question is does weight loss occur because of the fasting?
Many who follow this type of diet will say that it is the high fat that makes the fasting possible, and point to fat providing “satiety” (feeling of not being hungry) but as I will elaborate on below, high fat is not the only — or even the best way to increase satiety. Not only is protein far better at providing satiety, the amount of protein recommended by Dr. Stephen Phinney, MD, PhD and Dr. Jeff Volek, PhD, RD in their 2011 book the Art and Science of Low Carbohydrate Living is up to double the amount of the popularized keto diet.
Fat (9 calories per gram) is more than twice the calories of carbohydrate and protein (4 calories per gram each), so unless one is fasting frequently and/or for extended periods of time, it makes absolutely no sense to eat a high added fat diet if one is seeking weight loss and fasting has its drawbacks.
Frequent and/or Extended Fasting
The problem with fasting for periods longer than 24 hours is there is a loss of lean body mass (muscle) that goes along with it.
According to a 1979 research article published in the American Journal of Clinical Nutrition[1], protein is lost during extended fasting beginning on day 1 and continues until it reaches at maximum on day 3, then slowly declines. These results are validated in other studies, including one from Owen and Cahill in 1969 [2,3].
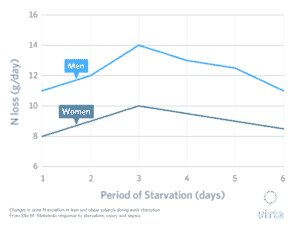
This graph from Virta Health [3] based on the same research [1] shows the losses in grams of nitrogen per day, where each gram represents the loss of about 1 ounce of lean tissue.
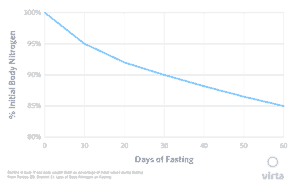 This graph also from Virta Health [3] and based on the same research shows the long-term loss of body nitrogen (protein) as % of pre-fasting value. While loss of protein slows somewhat after day 10, it continues right up to 60 days.
This graph also from Virta Health [3] and based on the same research shows the long-term loss of body nitrogen (protein) as % of pre-fasting value. While loss of protein slows somewhat after day 10, it continues right up to 60 days.
Based on this data, healthy overweight adults who fast for 10 days will lose 5 pounds of lean muscle [3].
According to a 1983 study by by Cahill, normal protein breakdown is ~75 g per day and while protein breakdown will eventually slow by ~25% when people are fasting long term in order to spare muscle, this is only as the “final stage of adaptation” and only “once ketoacid levels (ketones) reach a plateau and the brain is preferentially using ketoacids as fuel [4]“.
This time frame is consistent with the research above [1,2] showing that the slowing of muscle loss only occurs after 10 days of fasting, when ketones become the preferred fuel.
For older adults — especially post-menopausal women who are already at risk of sarcopenia (muscle loss), I do not recommend fasting longer than 24 hours.
Dietary Fat or Dietary Protein as the Source of Satiety
Proponents of the high fat ‘keto’ diet say that it is the high dietary fat that makes them so much less hungry, which makes them able to fast frequently and for extended period of time, and which results in them eating less over all. I don’t doubt this, but fat is not the only — or even the best source of satiety. Protein is far better at producing satiety and at less than half the calories of fat!
According to a 2010 study titled Energy Density of Foods: Effect on Energy Intake [3];
“when the satiating effects of macronutrients on appetite and energy intake (EI) are compared as nutrients come in the diet (and fat contributes disproportionately to energy density (ED), Joule-for-Joule, protein is consistently (at doses above 1.2 to 1.4 MJ) more satiating than carbohydrate (CHO), which is more satiating than fat.
When energy density (ED) is controlled, protein is still far more satiating than fat or carbohydrate.”
Given that protein produces more satiety than fat and has less than half the calories as fat, it makes much more sense if someone is seeking weight loss, to provide substantially more protein in the diet and significantly less dietary fat.
But how much protein?
Protein Intake in a Ketogenic Diet
In their classic 2011 book the Art and Science of Low Carbohydrate Living, Dr. Stephen Phinney, a physician with a PhD and Dr. Jeff Volek, a Dietitian with a PhD recommend that during weight loss, fat intake be 60% of calories and protein intake be to up to 30% of calories, with carbohydrate intake be 7.5-10% of calories for men, 2.5-6.5% of calories for women [4]. This mix of 60% fat, up to 30% protein and ~10% carbohydrate has up to twice the protein intake of the popularized ‘keto’ diet (75% fat, 15% protein, 10% carbohydrate).
NOTE (February 8, 2021): A ketogenic diet that is 30% protein might have most of its fat in the meat, eggs, and cheese that comprise it — and need not have any “added fat”. It is definitely not “low fat” (<30% fat) but is approximately ~60% fat. A ketogenic diet that has only 15% protein has to have lots of added fat (75%) to make up the rest of calories, because carbs are limited to 10%.
In relation to protein intake, Phinney and Volek write on page 210;
”…our studies of muscle retention and function during carbohydrate restriction [27,78,87], we recommend daily protein intakes between 1.5 and 2.5 grams per day per kg of reference body weight [6].”
What would this amount of protein look like in terms of intake?
A woman who is 5′ 4.25″(1.63 m) tall has an IBW (lean body mass) of 127 pounds (55 kg), so protein intake according to Phinney and Volek should be between 82.5 g protein (at 1.5 g/kg) to 137.5 g protein (at 2.5 g/kg).
A man who is 5’9″ (1.75 m) tall has an IBW (lean body mass) of 155 pounds (70 kg), which means that based on of reference body weight which is the half according to Phinney and Volek, protein intake should be 105 g protein (at 1.5 per kg) to 175.0 g protein (at 2.5 g/kg).
In a more recent 2018 article published online by Drs. Phinney and Volek along with Dr. Brittanie Volk, who is also a Dietitian with a PhD write;
”While a precise analysis of dose-response to varying protein intakes during nutritional ketosis has not been done in humans, we have performed a number of studies indicating that most healthy humans maintain lean body mass and function during a ketogenic diet providing between 1.5 and 1.75 grams of protein per kg of reference body weight’ (Phinney 1983, Davis 1990). Furthermore, there are no convincing human studies showing any benefit from dietary protein above 2.0 g/kg reference weight for adults following a ketogenic diet.” [7]
Reference body weight is considered to be “roughly normal lean body mass, rather than total body weight.“ [7].
So what does this updated recommendation look like in terms of intake?
A woman who is 5′ 4.25″(1.63 m) tall has an IBW (lean body mass) of 121 pounds (55 kg), so protein intake during nutritional ketosis according to Phinney, Volek and Volk should be between 82.5 g protein (at 1.5 g/kg) to 96.25 g protein (at 1.75 g/kg).
A man who is 5’9″ (1.75 m) tall has an IBW (lean body mass) of 155 pounds (70 kg), which means that according to Phinney, Volek and Volk should be 105 g protein (at 1.5 per kg) to 122.5 g protein (at 1.75 g/kg).
Protein to Energy (P:E) Ratio
In 2019, I was following with interest the evolving thoughts of Dr. Ted Naiman with regards to the amount of protein he was thinking that we should be eating.
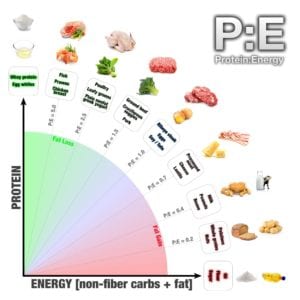 As I wrote about in a 2019 article, his ”P:E” ratio determines the Protein to Energy ratio of a food — with a focus on eating the most amount of protein for the least amount of energy (calories).
As I wrote about in a 2019 article, his ”P:E” ratio determines the Protein to Energy ratio of a food — with a focus on eating the most amount of protein for the least amount of energy (calories).
The P:E Diet was published as a book in 2020 and can best be described as a high protein, low fat and low-ish carb diet. I say “low-ish” carb because some calculations recommend carbs >130 g per day, which is the cut-off for low carb in most of the literature. On his web site the macros are clearly represented as being for healthy people without metabolic conditions, but I question whether they could even be considered for use in those with type 2 diabetes because of the higher carb intake. After all, type 2 diabetes is the end-state of an inability to appropriately handle carbohydrates in the diet.
After listening to a recent talk of Dr. Naiman’s last week on YouTube, I have begun following his posts on social media to try to understand his implementation of these recommended macros. It is important to keep in mind that Dr. Naiman’s focus is on healthy individuals seeking optimal muscle / lean body mass and not for those seeking remission of metabolic conditions, such as type 2 diabetes.
I was curious what the P:E calculator (available at p2eq.com) would assess the macros for the sample woman and sample man, above.
Note: Since it was not possible to select 5.4.25 in the tool for the height of the sample woman, I chose 5’4.5″ — the closest match.
According to the P:E ratio, a woman who is 5′ 4.5″ (1.64 m) should weigh 121 pounds (55 kg). According to this calculator and assuming she is metabolically healthy, this hypothetical woman should eat 1,470 kcals per day as 147 g protein (2.67 g protein /kg IBW), 49 g of fat and 110 g of total carbs.
According to Dr. Naiman’s P:E ratio, a man who is 5’9″ (1.75 m) tall should weigh 155 pounds (70 kg). According to this calculator and assuming this man is metabolically healthy, he should should eat 1,860 kcals as 186 g protein (2.66 g pro/kg IBW), 62 g of fat and 140 g of total carbs.
In this calculation, the amount of protein recommended for both the woman and the man in the P:E ratio at ~2.66 g protein/kg IDW is higher than the range that Phinney and Volek determined in their 2011 book, The Art and Science of of Low Carbohydrate Living, which is based on 2.0 g protein/kg of ideal body weight.
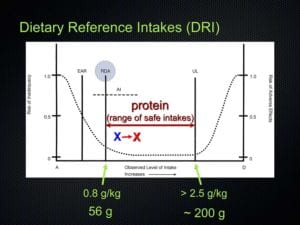 As I wrote about in an earlier article, according to Dr. Donald Layman, PhD, Professor Emeritus, University of Illinois, the highest end of the range of safe intake of protein is 2.5 g protein/ kg per day (maximum of 200 g / day).
As I wrote about in an earlier article, according to Dr. Donald Layman, PhD, Professor Emeritus, University of Illinois, the highest end of the range of safe intake of protein is 2.5 g protein/ kg per day (maximum of 200 g / day).
The high end of Phinney and Volek’s recommendations from their 2011 book of 2.5 g protein/kg IDW are at what Dr. Layman indicates is the high end of the safe range. While Dr. Naiman’s recommendations at 2.66 g protein/kg IDW is slightly higher than the 2.5 g protein/kg IDW, it is not in terms of the absolute number of grams of protein (>200 g/day).
NOTE (February 23, 2021):
The upper limit for using protein for energy is the determined by the disposal of ammonia from the protein, as urea in the urine. Humans apparently saturate disposal at ~3.21 g of protein / kg of lean body mass. Therefore, a safe upper limit of protein as a percentage of total energy requires knowing lean mass and estimated energy consumption (i.e. how many calories need to remain weight stable.
Example 1:
A 100 kg man with 20% body fat would have 80 kg lean mass, so would have a maximum protein ceiling of ~256g/day (based on the maximum amount of ammonia disposal of 3.21 g of protein / kg of lean body mass). Assuming his energy consumption is 2500 kcal/day, 256 g of protein is around 41% of total energy.
Example 2:
(a) A 60 kg woman with 25% body fat, would have 45 kg of lean mass, so would have a maximum protein ceiling of 144 g/day. Assuming her energy consumption is 2000 kcal/day, 144 g of protein would be 29% of total energy.
BUT
(b) The same 60 kg woman who has only 10% body fat would have 54 kg lean mass, so would have a maximum protein ceiling of 173 g pro/day (2000 kcal/day) which would be 35% of energy. The woman is the same size, but her amount of lean mass is greater, so she can safely have a higher percentage of energy as protein.
[special thanks to Richard Morris, research biochemist for the information on ammonia disposal rates in humans.]
People seeking follow a low carb diet come with very different needs. Some people can’t necessarily afford to eat “keto” without fasting (as it reduces costs if one is not eating every day, or is only eating a few days per week) — so if that is the only way they can afford to do it, then one has to weigh the effect of fasting on lean body mass versus the risk of them remaining obese or diabetic.
A person seeking weight loss and/or improved metabolic health has a wide range of low carb and ketogenic options to choose from, with a choice of protein intake ranging from 1.5 g protein – 2.5 g protein per kilogram of ideal body weight.
NOTE (February 8, 2021): I should make it clear that Phinney and Volek do not use ideal body weight as a means to determine what a person’s weight should be, but as a means for determining the amount of protein one should eat, based on their lean body mass (with IBW being a good estimate). In my practice, I use ideal body weight the same way. Since my focus is on metabolic health, I use waist to height ratio as the primary determinant, along with optimal lab results. When people reach a waist-to-height ratio of 0.50 with optimal lab markers, then I consider everything else a matter of aesthetics.
The “best macros” are the one’s based on your individual needs and health- and weight-loss goals.
Note (February 9, 2021):
If someone is metabolically healthy and seeking to build lean body mass (muscle), then a diet that is 40% protein and 30% fat and 30% carbs may be appropriate.
If someone is overweight, obese or lean (e.g. TOFI – thin on the outside, fat on the inside), but has diabetes or prediabetes, then a diet that is 40% protein BUT 30% carbs would not be such a great idea.
If someone prefers to seek weight loss or the benefits of ketone production — and is not at risk for sarcopenia (muscle loss), then a ketogenic diet which is only 15% protein and which uses the combination of a high fat diet (75%) with regular periods of fasting may be the way to go.
Someone preferring up to 30% protein instead of only 15% protein may prefer a ketogenic diet with only 60% fat due to protein having the highest satiety.
There is no one-sized-fits-all low carb or keto diet.
More Info?
If you would like more information about my services then please have a look under the tab of that name or send me a note through the Contact Me form.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchfRD/
Instagram: https://www.instagram.com/lchf_rd
Copyright ©2021 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
- G B Forbes, E J Drenick, Loss of body nitrogen on fasting, The American Journal of Clinical Nutrition, Volume 32, Issue 8, August 1979, Pages 1570—1574, https://doi.org/10.1093/ajcn/32.8.1570
- Owen OE, Felig P, Morgan AP, Wahren J, Cahill GF Jr. Liver and kidney metabolism during prolonged starvation. J Clin Invest. 1969 Mar;48(3):574-83. doi: 10.1172/JCI106016. PMID: 5773093; PMCID: PMC535723.
- Phinney SD, Volek JS, To Fast of Not to Fast: what are the Risks of Fasting?, December 5, 2017, Virta Health, https://www.virtahealth.com/blog/science-of-intermittent-fasting
- Cahill GF Jr. President’s address. Starvation. Trans Am Clin Climatol Assoc. 1983;94:1-21.
- Stubbs J, Ferres S, Horgan G, Energy Density of Foods: Effects on Energy Intake, Critical Reviews in Food Science and Nutrition, 40:6, 481-515, 2010
- Volek JS, Phinney SD, The Art and Science of Low Carbohydrate Living: An Expert Guide, Beyond Obesity, 2011
- Phinney SD, Volek JS, Volk B, How Much Protein Do You Need In Nutritional Ketosis? February 21, 2018, Virta Health, https://www.virtahealth.com/blog/how-much-protein-on-keto