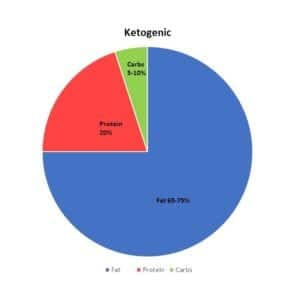
As I wrote about in a recent article, there’s more than one way to eat a low carb ketogenic diet including (1) low carb high fat (2) low carb high protein and (3) a mixed approach of higher protein lower fat during weight loss, then a moderate protein high fat during weight maintenance. Up until very recently my approach with my own weight loss has been low carb high fat – with the focus on monounsaturated fats such as olive oil, avocado oil, nut and seeds (and their oils) and omega 3 fatty acids from fatty fish. The problem has been that the last while, my weight loss and the rate at which my blood sugars were coming down has been too slow. As I do with my clients, it was time for a different approach. Since both of the other two types of low carb diet involves higher protein and lower fat I knew this is what I needed to do, but how much protein? How much fat? Do I keep carbs the same or lower them? In answering these questions, I have achieved a major breakthrough in my own ‘journey’ to better health.
I started with carbs. In discussion with my endocrinologist, I knew she supported carbs at 10% or less of my intake so I calculated my needs based on my gender, height, weight, activity level and weight loss goal – just as I do for my clients, and then figured out how many grams of carbs I could have in a day at this level. It was even lower than the amount of carbohydrate that I had been eating (which had been lowered twice over the last 10 months – from moderate, to low and now to very low), but since this ‘very low’ limit was in line with what my endocrinologist recommended, I set my carb limit at that.
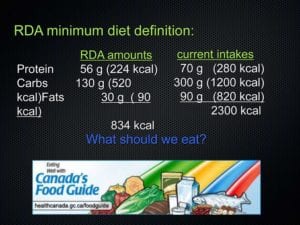
Protein, rather than fat had to be the second macronutrient I needed to set and since it was to be based on lean body mass and not my total weight, I determined my fat percentage. Then, I calculated how much protein I needed to eat per day based on the research studies. As it turned out, the lowest end of the range was considerably more than I had been eating, and only just slightly higher than what the average Canadian or American eats in a day. This was a bit of an obstacle for me, as I am not a big egg eater also not a big red-meat eater and there’s only so much chicken I can handle. I knew I wanted to continue to eat a few ounces of cheese every day as this is a major calcium source, but that meant factoring in the fat the cheese would add, which I did. Nuts again cropped up as a significant problem – not for their carb content, as much as their fat content. Eating lower fat and higher protein meant nuts and seeds were going to be limited to a sprinkle on a salad and cream in my coffee was limited to a little bit once a day. I needed to look at option that would work for me in terms of protein and since I don’t eat pork or shellfish, that left me focusing on freshwater and sea fishes as well as finding ways to include beef and lamb along with different kinds of poultry.
Even though I live on the West Coast, there are many kinds of fish available to me to eat besides the ubiquitous sockeye salmon and halibut. I began exploring what was available frozen and rediscovered sea fishes such as whole mullet, mackerel and milkfish, fresh water fish such as whitefish, as well as the bags of filleted cod for quick preparation (I avoid basa and talapia because they are high in omega 6 fat, which makes them pro-inflammatory). I cooked a whole salmon on Friday and have been eating the leftovers cold for breakfast, since I am not that fond of eggs.
I began to think of poultry beyond chicken and bought and roasted a turkey (which also left leftovers to eat for my early meal) and began to think of ways to cook quail and duck (minus all the fat).
Eating a wide variety of fish and poultry with some cheese thrown in there has provided me with sufficient protein on most days and for the occasional time that I just can’t handle eating more, I mix some cocoa powder with whey isolate and drink that.
I should add that when I eat, I am not trying to 'fulfill' my macronutrient distribution (gms of protein, carbohydrate and fat) but rather, I eat as much whole food protein at my two meals (one mid-morning and the other around supper time) then eat a good 2-3 cups of low carb veggies with the protein. I add a little bit of mayo, butter or cream to make things taste good, and don't "count" anything except carbs. In fact, I encourage my clients to do likewise. I focus on maximizing whole food protein within my Meal Plan and the fat that I end up with is what naturally comes with those. It's a very "easy" lifestyle to follow, once the calculations are done - and since I do those for my clients, it only makes sense for me to do them for myself, too. Leading by example, right?
The results have been astounding.
I’ve lost 4 pounds in 2 weeks and as significantly, I have seemingly lost most of it off my abdomen and not just the fat under the skin (sub-cutaneous fat), but the fat deep in my belly, around my organs (visceral fat).
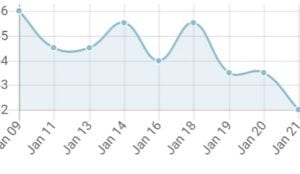
This is HUGE because it visceral fat is most highly correlated to insulin resistance – which is what I am trying to reverse. Just look what’s happened to my blood sugar over the weekend:
My fasting blood sugar actually went down after it went up in the wee hours of the morning (the effects of Dawn Phenomena) which would seem to indicate that the loss of belly fat is indeed making me more insulin sensitive! When my early morning blood sugar goes up due to Dawn Phenomena, my cells are now more responsive to the resulting spike in insulin, and the excess sugar is now being taken into the cells, like it is supposed to!
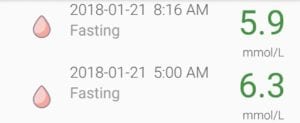
This wasn’t a one-off thing either. This is what happened yesterday and this morning;

These changes cannot be attributed to the baby dose of Metformin that I’m taking before bed (which is lowering the magnitude of the Dawn Phenomena rise), but is reasonably related to the only other change that I have made which is the increase in the amount of protein I am eating (in grams) and the reduction in the amount of fat and carbs I am eating.
We do know that over time, the body gets adapted to the changes we make – whether dietary or exercise changes and that to continue to get results at the rate that we want, we need to change the approach. I do this in my follow-up approach with my client over their weight-loss and health journeys and it was necessary for me to this for myself, as well.
While it is much ‘easier’ for me to eat a lower protein, higher fat diet as these are the foods I prefer, my goal is to reverse the symptoms of Diabetes and put myself into remission (have normal fasting blood glucose and normal HbA1C long term).
”Let food be thy medicine and medicine be thy food.”
– Hippocrates
For me, while it is not the easiest of most natural way for me to eat, increasing the amount of protein, decreasing the amount of fat and limiting my carbs to those contained in non-starchy vegetables is allowing my body to heal in the ways in needs to – allowing food to be my medicine.
The question arises “was it the lower carbs or higher protein that has made the difference?”. I had tried a few times before to lower my carbs down to almost as low as I am now and to made up most of the extra intake (outside of my basic protein need) from fat, but this did not contribute as much to me not being hungry (i.e. satiety) as this higher ratio of protein with the rest from the same sources of fat (which is still “high” by most standards). So yes, it is partially due to the lower carb content, but reasonably to the higher protein content, as well.
My entire ‘journey’ has been (and is) about me doing whatever it takes to achieve my goals with a healthy and evidence-based diet and it’s hard to argue that with 30 years of combined research in this area that Phinney and Volek aren’t reliable in terms of evidence. It mades sense for me to do what they recommend, even it if isn’t the most “natural” way for me to eat.
My hope is that in time, when I am no longer insulin resistant, that I can switch over to a moderate protein high fat intake as Phinney and Volek recommend, but for now this is what is best because it is working and because it is in accordance with what my endocrinologist recommended, and under the supervision of my doctor.
The ironic thing is that most of my clients do really well on moderate to low carb restriction with a fairly high intake of monounsaturated and omega 3 fat and are content with their rate of progress which is great. For those that will need, in time, to make changes to the way they pursue a low carb lifestyle, I hope by me leading by example, it will be encouraging to them.
Tomorrow I am scheduled to have my HbA1C level checked which won’t factor in much of these new changes in blood sugar levels because the test looks at the amount of glucose which stays attached to hemoglobin (Hb) for the life of the red blood cell (i.e. glycated hemoglobin), which is normally about 120 days / 3-4 months. At my last test 3 months ago, my glycated hemoglobin was 7.0% and what I am ultimately aiming for is a HbA1C of <6.0%, which would be in the non-Diabetic range. Whether its this time or the next time isn’t really as significant is that it has been more than 10 months where I have diligently been working towards that goal.
I’ve successfully normalized my triglycerides and lipids and brought them into the ideal range and have substantially lowered my blood pressure – and both of these were done by diet alone. It will be interesting to see the effect of these diet changes on my HbA1C, as well as have some indication of how much more I have yet to do.
It’s all about progress, not perfection and significant progress is being made, as evidenced by this recent personal breakthrough.
If you’d like to know how I can help you achieve your health and nutrition goals, please send me a note using the “Contact Me” form on this web page.
To our good health!
Joy
You can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
Copyright ©2018 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
























 So much for people’s good intentions of substituting a healthy monounsaturated fat for a refined, industrial seed oil like canola.
So much for people’s good intentions of substituting a healthy monounsaturated fat for a refined, industrial seed oil like canola.









 If you’re in a rush, this shake can be made quickly in a bowl and poured over ice and enjoyed…
If you’re in a rush, this shake can be made quickly in a bowl and poured over ice and enjoyed… …or if you have a few extra minutes and a blender, it can be whirred with a little extra ice to make a wonderful meal replacement smoothie.
…or if you have a few extra minutes and a blender, it can be whirred with a little extra ice to make a wonderful meal replacement smoothie.