This is Part 1 in a new series titled Bad Fat Enduring Beliefs and this article looks at how and when saturated fat was vilified and why sugar was vindicated as the cause of heart disease.
The Diet-Heart Hypothesis
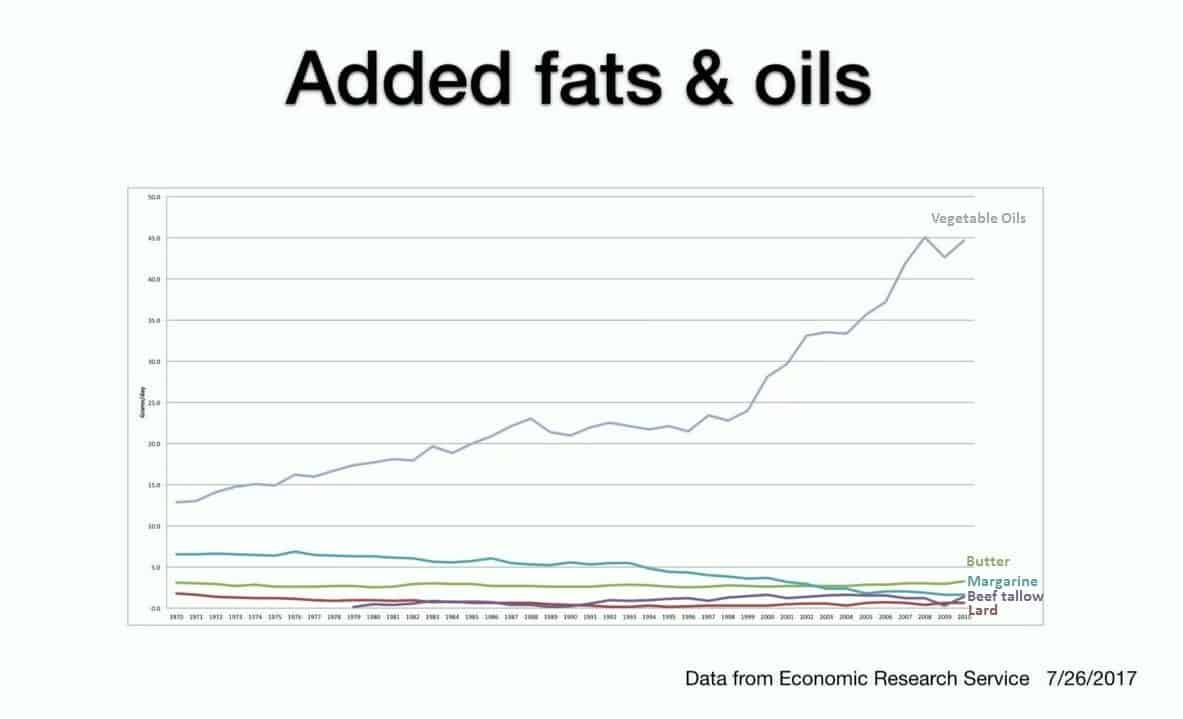
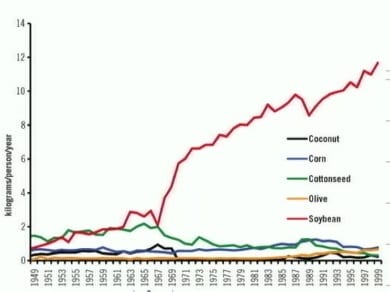
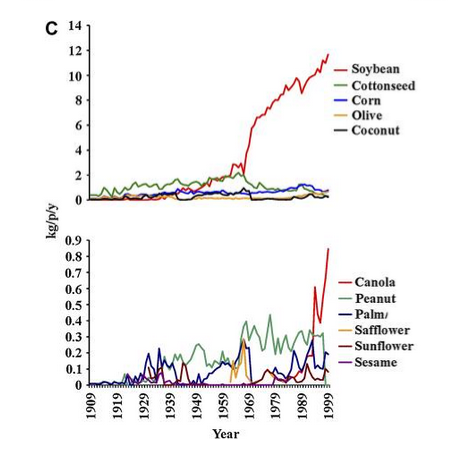
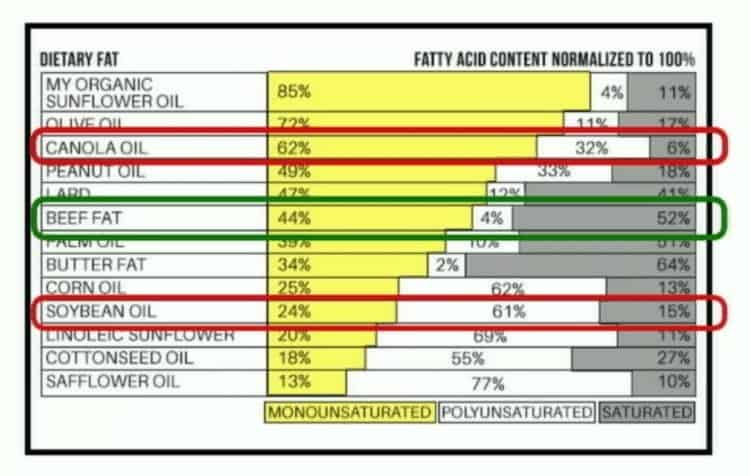
The diet-heart hypothesis is the belief that eating foods high in saturated fat contributed to heart disease was first proposed in the 1950s by a scientist named Ancel Keys who believed that by replacing saturated fat from meat, butter and eggs with newly-created industrial polyunsaturated vegetable oil (such as soybean oil) that heart disease and the deaths allegedly associated with it would be reduced by lowering blood cholesterol levels.
In 1952, Keys suggested that Americans should reduce their fat consumption by 1/3 and in 1953, Keys published a study where he said that he had demonstrated that there was an association between dietary fat as a percentage of daily calories and death from degenerative heart disease [1].
Four years later, in 1957, Yerushalamy et al published a paper with data from 22 countries[2] which showed a weak relationship between dietary fat and death by coronary heart disease — a much weaker relationship than was suggested by Keys’s in 1953. Nevertheless, in 1989 Keys and colleagues published their Seven Countries Study[3] which maintained there was an associative relationship between increased dietary saturated fat and Coronary Heart Disease — basically ignoring the data presented in Yerushalamy’s 1957 study, and which failed to study countries where Yerushalamy found no relationship between dietary fat and heart disease, such as in France. The paper maintained that the average consumption of animal foods (with the exception of fish) was positively associated with 25-year Coronary Heart Disease death rates and the average intake of saturated fat was strongly related to 10 and 25-year Coronary Heart Disease death rates. Keys and colleagues knew of the Yerushalamy’s data from 1957 and seemingly dismissed it.

Keys et al – Epidemiological studies related to coronary heart disease: characteristics of men aged 40—59 in seven countries [1]

The Sugar Industry Funding of Research Vilifying Fat
In August of 1967, Stare, Hegsted and McGandy – the 3 Harvard researchers paid by the sugar industry published their review in the New England Journal of Medicine, titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which vindicated sugar as a contributor of heart disease and laid the blame on dietary fat and in particular, saturated fat and dietary cholesterol (previous article on that topic here).
Stare, Hegsted and McGandy concluded that there was “only one avenue” by which diet contributed to the development and progression of “hardening of the arteries” (atherosclerosis) and resulting heart disease and that was due to how much dietary cholesterol people ate and its effect on blood lipids;
”Since diets low in fat and high in sugar are rarely taken, we conclude that the practical significance of differences in dietary carbohydrate is minimal in comparison to those related to dietary fat and cholesterol…the major evidence today suggests only one avenue by which diet may affect the development and progression of atherosclerosis. This is by influencing the levels of serum lipids [fats], especially serum cholesterol.” [4]
These researchers concluded that there was major evidence available at the time which suggested that there was only ONE avenue for diet to contribute to hardening of the arteries and the development of heart disease – yet a year later in 1968 the report of the Diet-Heart Review Panel of the National Heart Institute made the recommendation that a major study be conducted to determine whether changes in dietary fat intake prevented heart disease because such a study had not yet been done [5];
”the committee strongly recommended to the National Heart Institute that a major definitive study of the effect of diet on the primary prevention of myocardial infarction be planned and put into operation as soon as possible. “
This is an important point; prior to a major study having ever been conducted to determine whether changes in dietary cholesterol impacts heart disease, 3 Harvard researchers paid by the sugar industry concluded that there was “only one avenue” by which diet contributed to the development and progression of atherosclerosis (i.e. “hardening of the arteries”) and heart disease and that was due to how much dietary cholesterol people ate and its effect on blood lipids.
Researcher Paid by the Sugar Industry Helps Develop the 1977 US Dietary Guidelines
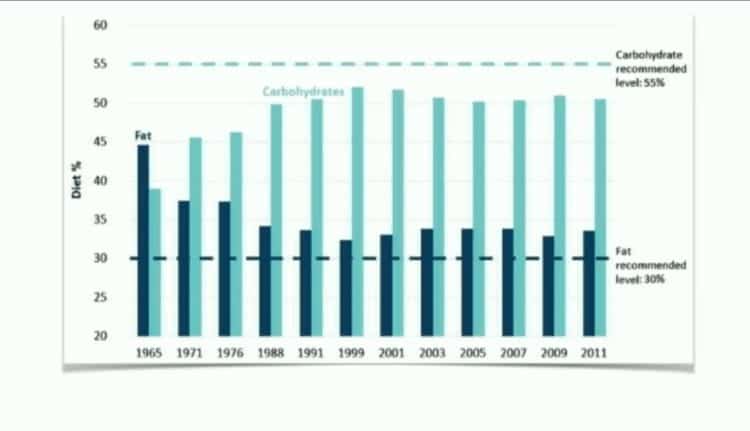
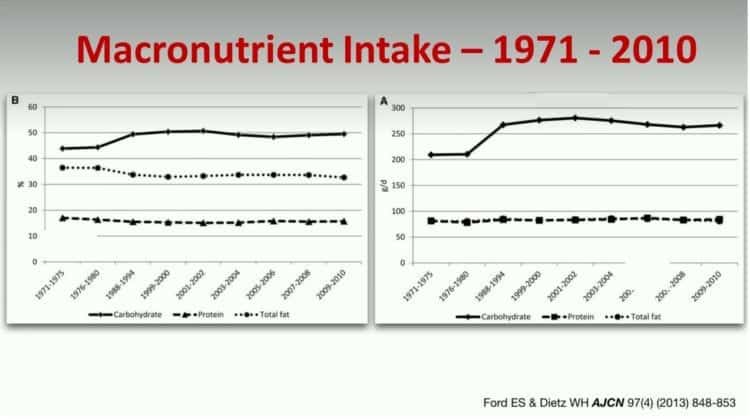
Only ten years after the sugar industry paid Stare, Hegsted and McGandy to write their reviews, the same Dr. Hegsted was directly involved with developing and editing the 1977 US Dietary Guidelines [6] which recommended an increase in dietary carbohydrate and a decrease in saturated fat and cholesterol in the diet.
Historic changes in the Dietary Recommendation in Canada have largely been based on changes to the Dietary Recommendations in the US, and as a result both stemmed from a belief that eating saturated fat increases total cholesterol and therefore increases the risk of heart disease.
The problem is this belief is just that, a belief.
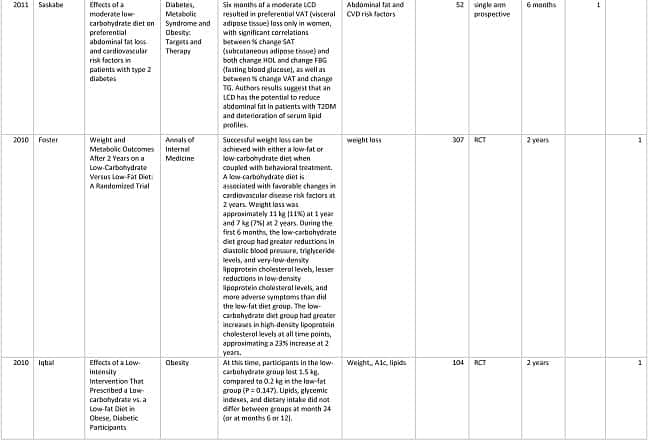
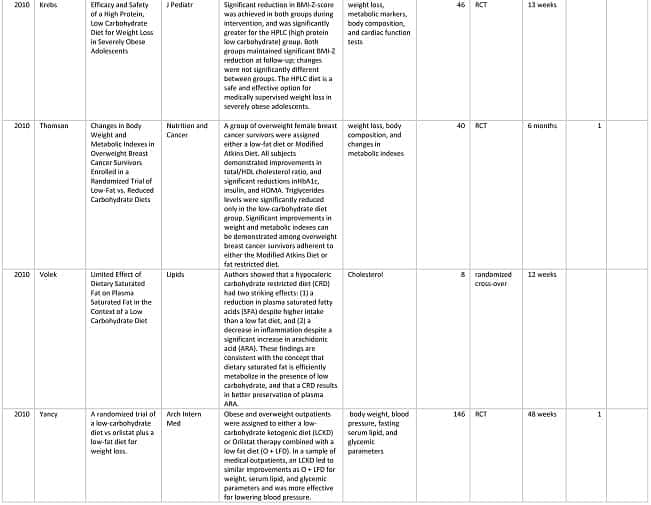
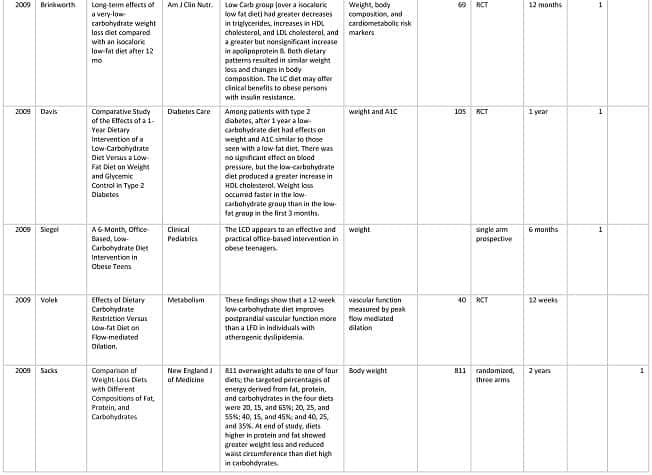
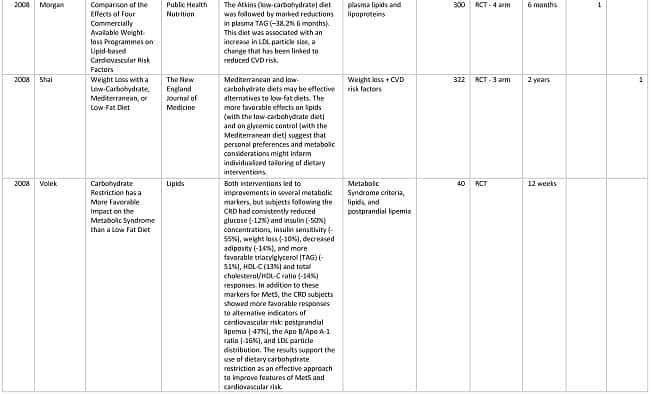
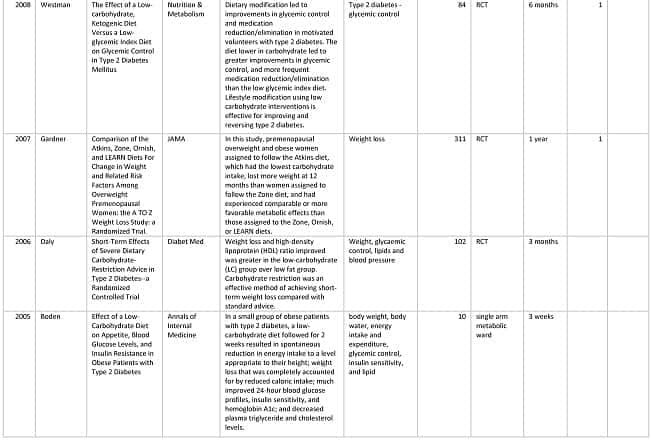
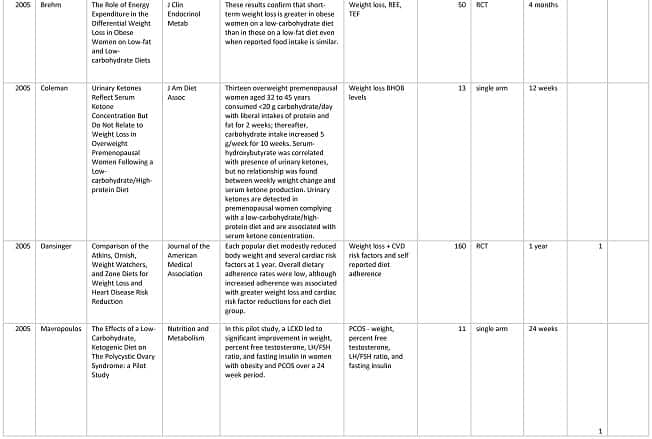
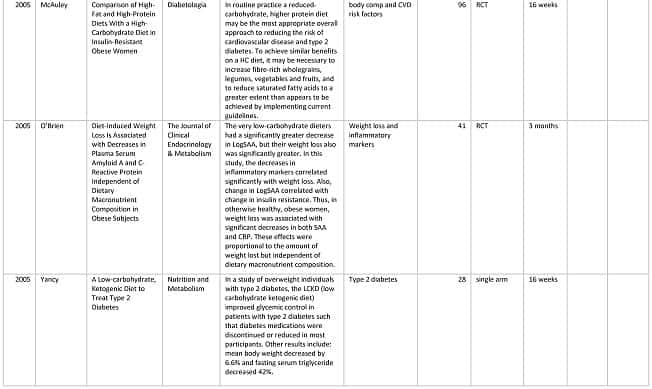
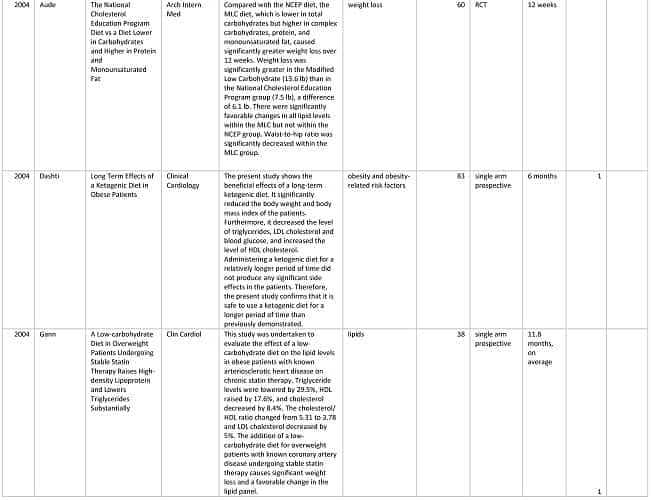
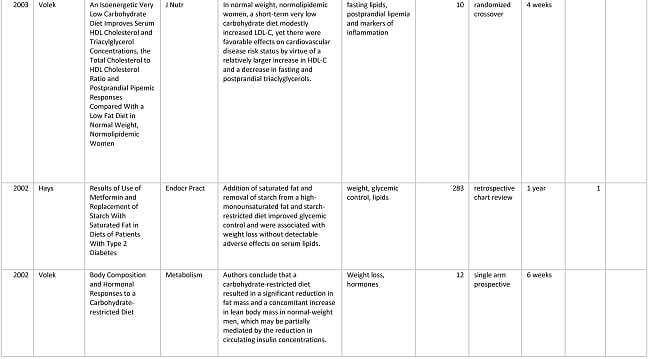
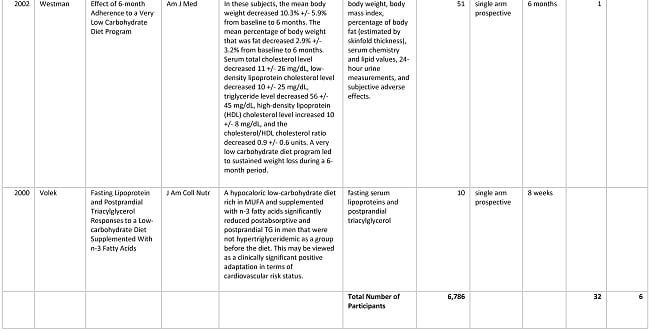
There have been many studies that have disproved this including a randomized, controlled dietary intervention trial from 2008 which compared a low calorie, low in fat with a low carbohydrate, high fat diet of the same number of calories. This study found that overall heart health is significantly improved when carbohydrate is restricted, rather than fat [7,8].
Not all LDL cholesterol is “bad” cholesterol.
Small, dense LDL (“Pattern B”) causes more “hardening of the arteries” than the large, fluffy LDL particles (“Pattern A”)[9].
It has been reported that when dietary fat is replaced by carbohydrate, the percentage of the small, dense LDL particles (the ones that cause hardening of the arteries) is increased, increasing risk for heart disease. Furthermore, the low carb diet increased HDL (so-called “good” cholesterol), which are protective against heart disease and HDL and small, dense LDL were made worse on the low fat diet. Quite opposite to the “Diet-Heart Hypothesis, this study demonstrated improvements in the risk of heart disease for those eating a low carbohydrate, high fat diet compared to those eating a low fat, low calorie diet – which is not all that surprising given that it had been reported previously that a diet high in saturated fat actually lowers small, dense LDL (the type of LDL that causes hardening of the arteries) and raises the large fluffy LDL; actually improving risk factors for heart disease [15].
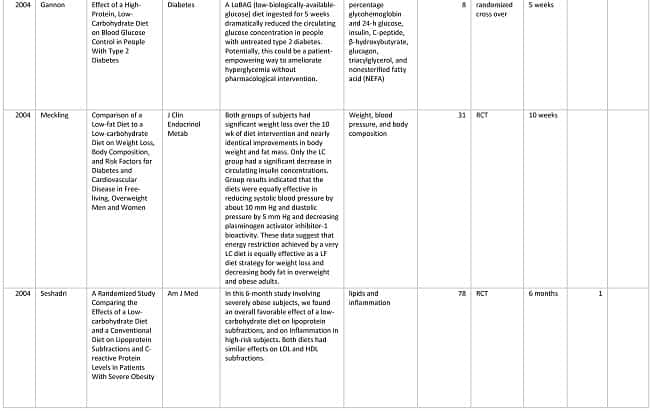
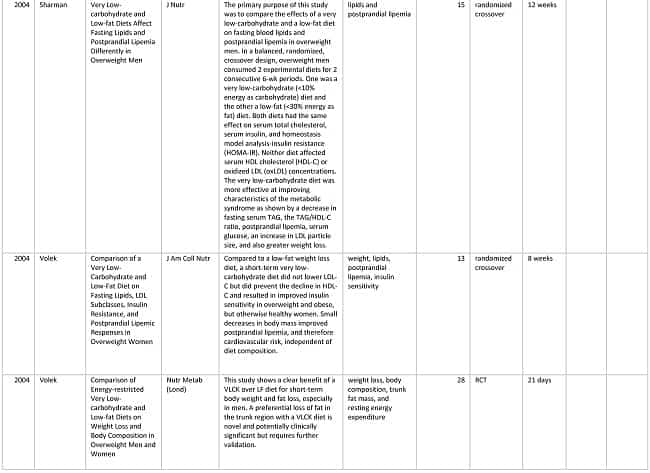
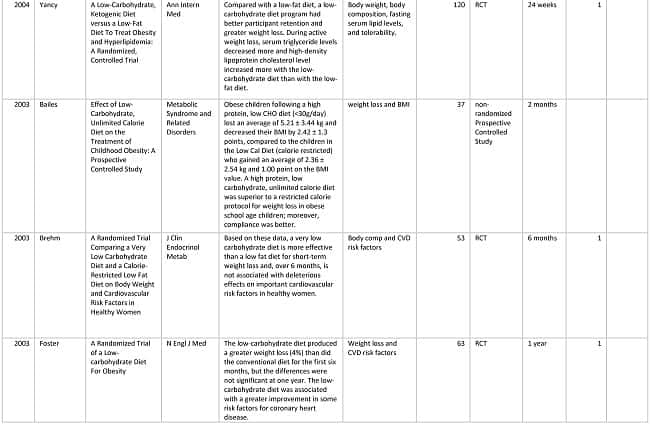
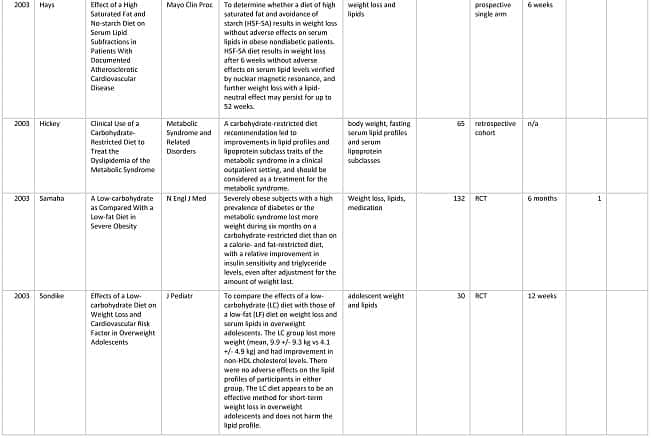
There are also other randomized controlled trials from 2004-2008 which demonstrate that a low carb diet improves blood cholesterol test results more than a low fat diet [10,11,12,13,14] – yet despite this, the belief that eating saturated fat increases blood cholesterol, persists.
Both the American and Canadian governments are in the process of revising their Dietary Guidelines and what is clear is that what is needed is an external, independent scientific review of the current evidence-base for the enduring false belief that dietary fat, especially saturated fat contributes to heart disease.
Have questions about how I can help you follow a low carb lifestyle?
Please send me a note using the “Contact Me” tab above and I will reply shortly.
To our good health!
Joy
You can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
References
- KEYS, A., Prediction and possible prevention of coronary disease. Am J Public Health Nations Health, 1953. 43(11): p. 1399-1407.
- Yerushalmy J, Hilleboe HE. Fat in the diet and mortality from heart disease. A methodologic note. NY State J Med 1957;57:2343—54
- Kromhout D, Keys A, Aravanis C, Buzina R et al, Food consumption patterns in the 1960s in seven countries. Am J Clin Nutr. 1989 May; 49(5):889-94.
- McGandy, RB, Hegsted DM, Stare,FJ. Dietary fats, carbohydrates and atherosclerotic vascular disease. New England Journal of Medicine. 1967 Aug 03; 277(5):242—47
- The National Diet-Heart Study Final Report.” Circulation, 1968; 37(3 suppl): I1-I26. Report of the Diet-Heart Review Panel of the National Heart Institute. Mass Field Trials and the Diet-Heart Question: Their Significance, Timeliness, Feasibility and Applicability. Dallas, Tex: American Heart Association; 1969, AHA Monograph no. 28.
- Introduction to the Dietary Goals for the United States — by Dr D.M. Hegsted. Professor of Nutrition, Harvard School of Public Health, Boston, MASS., page 17 of 130, https://naldc.nal.usda.gov/naldc/download.xhtml?id=1759572&content=PDF
- Volek JS, Fernandez ML, Feinman RD, et al. Dietary carbohydrate restriction induces a unique metabolic state positively affecting atherogenic dyslipidemia, fatty acid partitioning, and metabolic syndrome. Prog Lipid Res 2008;47:307—18
- Forsythe CE, Phinney SD, Fernandez ML, et al. Comparison of low fat and low carbohydrate diets on circulating fatty acid composition and markers of inflammation. Lipids 2008;43:65—77
- Tribble DL, Holl LG, Wood PD, et al. Variations in oxidative susceptibility among six low density lipoprotein subfractions of differing density and particle size. Atherosclerosis 1992;93:189—99
- Foster GD, Wyatt HR, Hill JO, et al. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med 2003;348:2082—90.
- Stern L, Iqbal N, Seshadri P, et al. The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: one-year follow-up of a randomized trial. Ann Intern Med 2004;140:778—85
- Gardner C, Kiazand A, Alhassan S, et al. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women. JAMA 2007;297:969—77
- Yancy WS Jr., Olsen MK, Guyton JR, et al. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: a randomized, controlled trial. Ann Intern Med 2004;140:769—77
- Shai I, Schwarzfuchs D, Henkin Y, et al. Dietary Intervention Randomized Controlled Trial (DIRECT) Group. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med 2008;359:229—41
- Dreon DM, Fernstrom HA, Campos H, et al. Change in dietary saturated fat intake is correlated with change in mass of large low-density-lipoprotein particles in men. Am J Clin Nutr 1998;67:828—36
Copyright ©2018 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.





















 In August 1967 the New England Journal of Medicine published the first review article written by Drs. Stare, Hegsted and McGandy titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which stated;
In August 1967 the New England Journal of Medicine published the first review article written by Drs. Stare, Hegsted and McGandy titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which stated;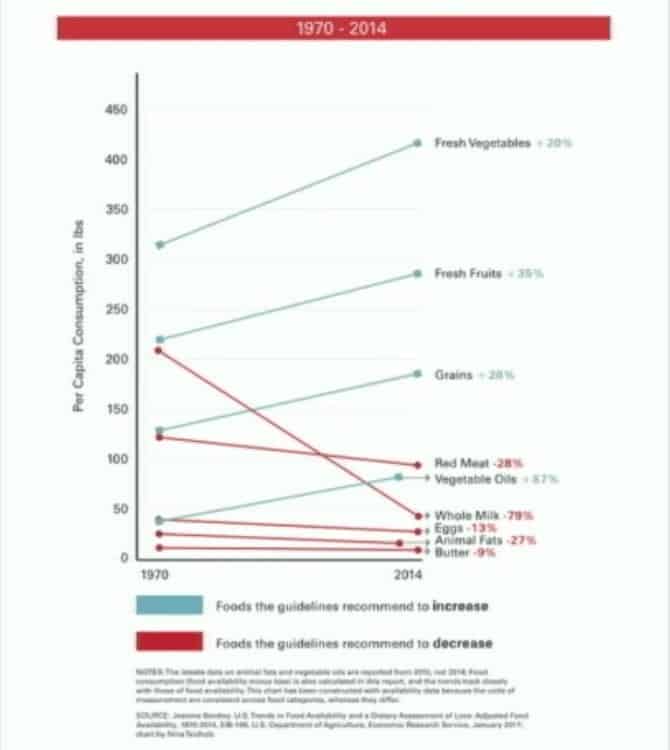




 To celebrate my one year anniversary, as a ‘present’ to myself, I bought a weight bench to use with my free weights and resistance bands, and have set it up in a corner of my room.
To celebrate my one year anniversary, as a ‘present’ to myself, I bought a weight bench to use with my free weights and resistance bands, and have set it up in a corner of my room. Are you at a fork in the road – having to choose between continuing to do the same things that haven’t worked previously or like me, ignoring it all and doing nothing?
Are you at a fork in the road – having to choose between continuing to do the same things that haven’t worked previously or like me, ignoring it all and doing nothing?







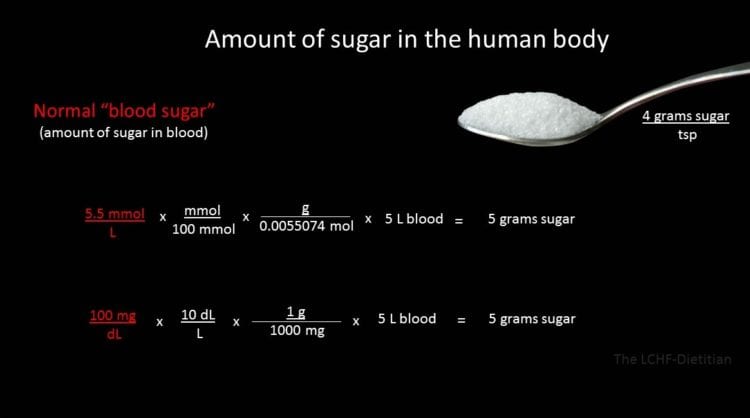
 glucose reading at 5:27 am and got a reading of 4.8 mmol/L (86 mg/dl) and thought “that can’t be!“, as I know that is a blood sugar reading that I only obtain after more than 18 hours of fasting.
glucose reading at 5:27 am and got a reading of 4.8 mmol/L (86 mg/dl) and thought “that can’t be!“, as I know that is a blood sugar reading that I only obtain after more than 18 hours of fasting. I got another test strip from the same vial (recently opened and not expired) and tested the same thumb in a location immediately beside where I had just tested and got a reading of 5.8 mmol/L (105 mg/dl) and thought “that seems more reasonable, but what’s with the meter?”.
I got another test strip from the same vial (recently opened and not expired) and tested the same thumb in a location immediately beside where I had just tested and got a reading of 5.8 mmol/L (105 mg/dl) and thought “that seems more reasonable, but what’s with the meter?”.
 As for me, I have gone back to using a glucometer that I had on hand (which also tests blood ketones), as it is one of the models that passed.
As for me, I have gone back to using a glucometer that I had on hand (which also tests blood ketones), as it is one of the models that passed.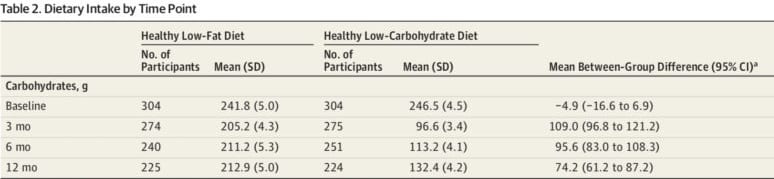




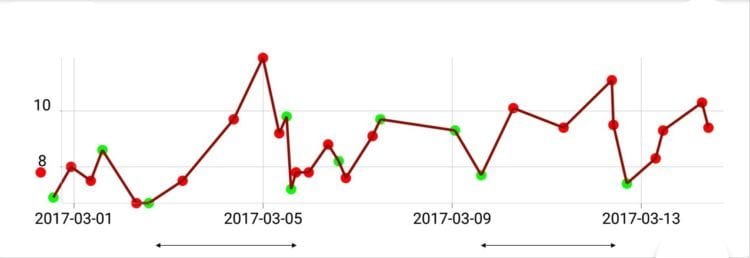
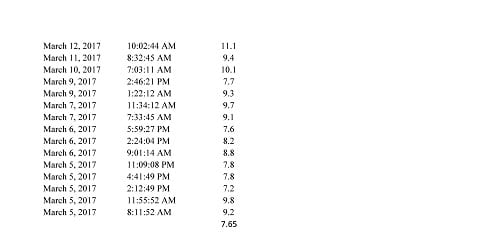
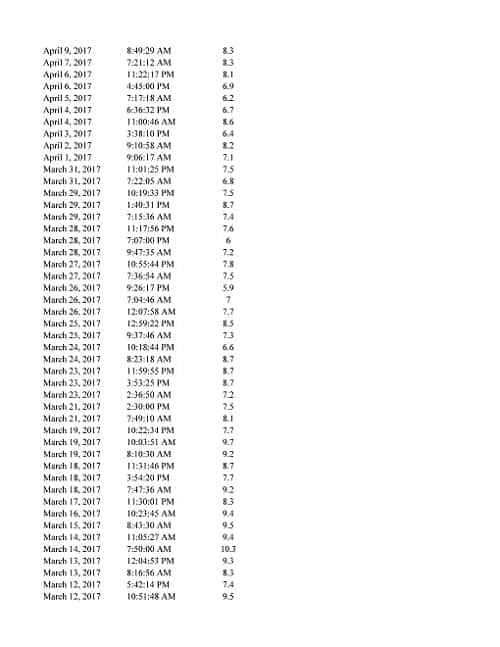
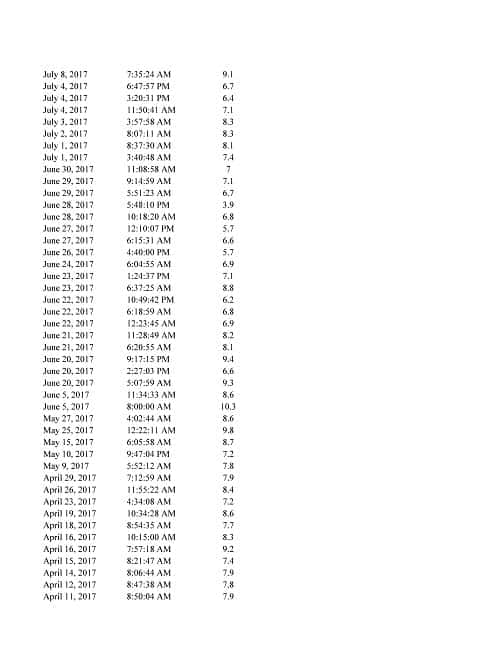
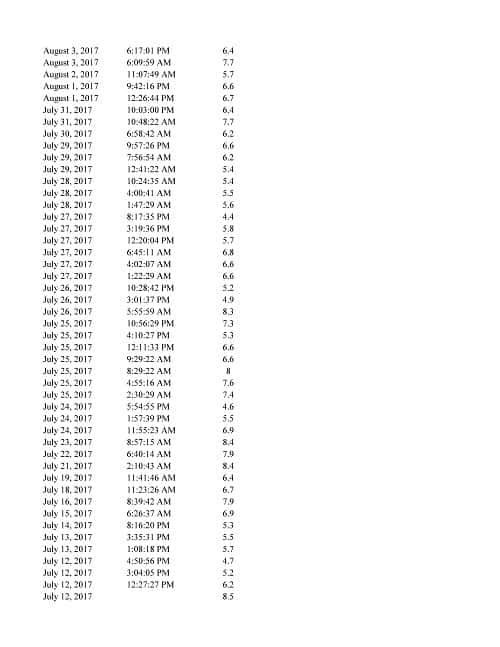
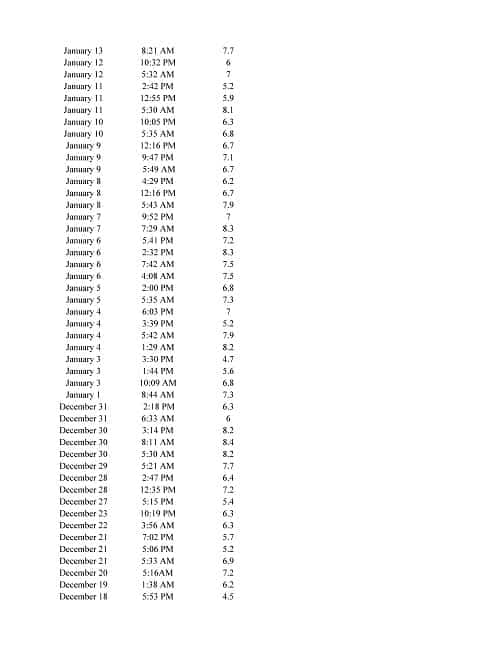
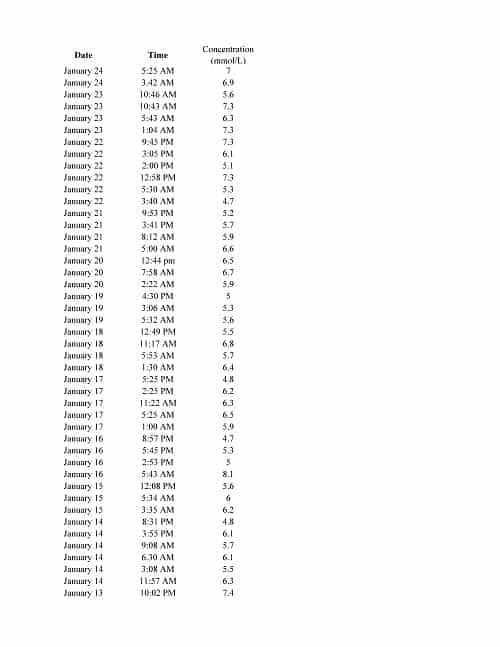
 As can be seen from the graph, my blood glucose was at lowest at 7.7 mmol/L (see photo to the left) and I had spikes well above 10 mmol/L, and I was averaging around 8.5 mmol/L over the course of the day – which is slightly higher than the average of those in the study.
As can be seen from the graph, my blood glucose was at lowest at 7.7 mmol/L (see photo to the left) and I had spikes well above 10 mmol/L, and I was averaging around 8.5 mmol/L over the course of the day – which is slightly higher than the average of those in the study.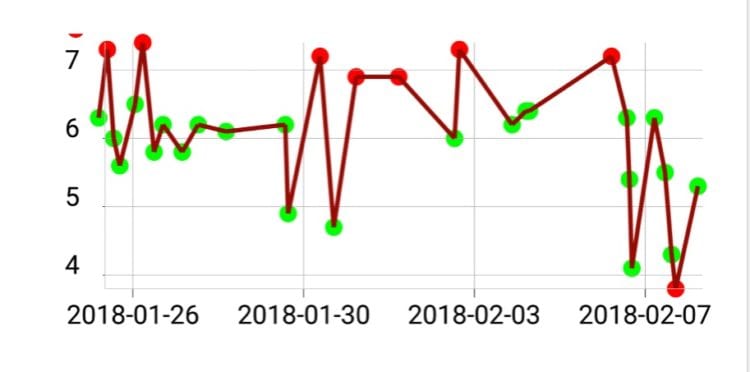
 Early this morning, my fasting blood glucose was 5.3 mmol/L (95 mg/dl) which is in the normal non-Diabetic range. This is a first! This was without taking Metformin.
Early this morning, my fasting blood glucose was 5.3 mmol/L (95 mg/dl) which is in the normal non-Diabetic range. This is a first! This was without taking Metformin.


















 My journey began on March 5, 2017 when I was a fat Dietitian with all the benchmark symptoms of Metabolic Syndrome including Type 2 Diabetes, high blood pressure, high LDL cholesterol and triglycerides, abdominal adiposity (i.e. “a belly”) and high BMI (high weight for height). Physically I was a mess but my biggest problem was that I was in denial. It had been months since I had monitored my own blood sugar or blood pressure even though I had been diagnosed with Type 2 Diabetes 10 years earlier. I knew better.
My journey began on March 5, 2017 when I was a fat Dietitian with all the benchmark symptoms of Metabolic Syndrome including Type 2 Diabetes, high blood pressure, high LDL cholesterol and triglycerides, abdominal adiposity (i.e. “a belly”) and high BMI (high weight for height). Physically I was a mess but my biggest problem was that I was in denial. It had been months since I had monitored my own blood sugar or blood pressure even though I had been diagnosed with Type 2 Diabetes 10 years earlier. I knew better.