There is a common, but mistaken belief that there is such as thing as “the keto diet” (singular) — which is high in fat of all types, including cream, butter, bacon, avocado and fatty cuts of meat. In fact, there are a wide range of “keto diets” (plural) — including several different therapeutic ones, as well as those that have been popularized the last several years for weight loss. This article will explains the range of ketogenic diets that are available, and what they are used for as well as the unintended consequence of believing that a “keto diet” has to be high in fat.
What is a Ketogenic Diet?
A ketogenic diet is one that induces and sustains a state of ketosis, which is a natural metabolic state where the body burns fat as its primary fuel, rather than carbohydrate.
There are a number of different therapeutic ketogenic diets, as well as a number of weight-loss ketogenic diets.
What makes any diet ketogenic is not how much fat it contains, but the amount of carbohydrate it contains.
This bears repeating.
A ketogenic diet is determined solely on the basis of how much carbohydrate it contains, and not on how much fat in contains.
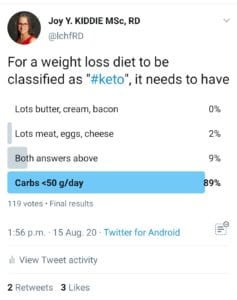
Ketogenic diets, which are also referred to in the literature as “very low carbohydrate diets” are where carbohydrate intake is limited to 20-50 g per day or 10% of total energy intake [1]. It is this low carbohydrate intake that results in the body using fat as its primary fuel, rather than carbohydrate and at this very low level of carbohydrate intake, blood ketone levels increase at or above 0.5 mmol/L, resulting in ketosis.
Ketosis is where the ketone betahydroxybutyrate (BHB) reaches levels between 0.5 – 3.0 mmol/L — and up to 4.0 mmol/L for therapeutic ketogenic diets used in the treatment of epilepsy, seizure disorder and glioblastoma.
Nutritional ketosis used predominantly for weight loss is usually set with BHB levels between 1.5-3.0 mmol/L [2].
Low carbohydrate diets are those where carbohydrate intake is limited to < 130 g per day or < 26% of total energy intake [1] and moderate carbohydrate diets are where carbohydrate intake is limited to 130—225 g per day or 26—45% of total energy intake [1].
Again, the amount of fat in the diet has nothing to do with a diet being ketogenic — only the amount of carbohydrate it contains.
Therapeutic Ketogenic Diets
First of all, what does “therapeutic” mean?
Something is therapeutic when it is used in the treatment of a disease. This may be a pharmaceutical drug or a diet. What makes a diet therapeutic is that it is used to treat a medical condition, or conditions.
A therapeutic diet may be prescribed by a physician, and implemented by a Dietitian or the physician themselves. When implemented by a Dietitian, a therapeutic diet is referred to as Medical Nutrition Therapy (MNT) [3].
The first therapeutic ketogenic diet was used in the 1920s by Dr. Russell Wilder, for the treatment of diabetes and later, for epilepsy.
Physicians at Harvard Medical School had begun experimenting with periods of extended fasting as a treatment, and discovered that seizures improved after 2-3 days. In 1921 , Dr. Russell Wilder[3] used a very high fat, low carbohydrate, and restricted protein diet in a series of patients with epilepsy, and found that it was as effective as fasting and had the advantage that it could be maintained for much longer a period of time than fasting.
The percentage of carbohydrate, fat and protein in what has since become called the “classic” Ketogenic Diet (KD) was worked out by Dr. M.G. Peterman in 1925 [4] and are the same as used today. In the classic KD, the total amount of calories are matched to the number of calories the person needs. Protein is usually determined as being 1 g of protein per kg body weight, 10-15 g of carbohydrate per day total, and the remainder of calories provided as fat. For very young children, the diet may be prescribed based on body weight (e.g. 75-100 calories for each kg (2.2 pounds) of body weight.
Since the 1920s, several other therapeutic ketogenic for the treatment of epilepsy and seizure disorder have been developed, including the Modified Ketogenic Diet (MKD) and the Modified Atkins Diet (MAD). These are all high fat diets, but differ in the amount of protein they contain. They are all very low carbohydrate diets, which is by definition what makes them ketogenic.
The classic Ketogenic Diet (KD) has a 4:1 ratio i.e. 4 parts of fat for every 1 part protein and carbs. In the classic Ketogenic Diet, 90% of calories come from fat, 6% from protein, and only 4% of calories come from carbohydrate.
The Modified Ketogenic Diet (MKD) has a 3:1 ratio i.e. 3 parts fat for every 1-part protein and carbohydrate. In a Modified Ketogenic Diet, 80-90% of calories come from fat, 12-15% of calories come from protein, and 5-6 % calories come from carbohydrate[5].
The Modified Atkins Diet (MAD) has a 2:1 ratio, with 2 parts fat for every 1-part protein and carbohydrate. In a Modified Atkins Diet, carbohydrates are restricted to <15 g / day for children, <20 g / day for adults. In a Modified Atkins Diet, 60% of calories come from fat, 30% of calories come from protein, and 10% of calories come from carbohydrate[5].
As well as their use in epilepsy and seizure disorder, any of the above therapeutic ketogenic diets may be prescribed for patients as adjunct treatment in glioblastoma, or as adjunct treatment in Alzheimer’s disease.
These high fat diets are not weight loss diets. These are therapeutic ketogenic diets used with the goal of producing high amounts of ketones (> 4.0 mmol/L / 40 mg/dl) for therapeutic reasons.
Other Types of Therapeutic Ketogenic Diets – for treatment of type 2 diabetes and obesity
In addition to the three types of therapeutic ketogenic diets above, ketogenic diets where carbohydrate is restricted to 50g of carbohydrates per day or less are considered Medical Nutrition Therapy (MNT) in the treatment of type 2 diabetes.
The American Diabetes Association has stated that reducing carb intake has the most evidence for improving blood sugar and has included the use of a very low carbohydrate (ketogenic) eating pattern for treating type 2 diabetes as listed in their 2019 Consensus Report and both the 2019 Standards of Medical Care in Diabetes (2019) and Standards of Medical Care in Diabetes (2020). In addition, Diabetes Canada released a Position Statement in April of this year outlining that a low carb and very low carb / keto (<50 g of carbohydrates per day) are both safe and effective treatment for adults with diabetes.
According to the American Diabetes Association, what makes a diet low carbohydrate (LC) or very low carbohydrate (VLC) / ketogenic is defined by the amount of carbohydrate contained in the diet, not the amount of fat. The American Diabetes Association’s Consensus Report defines low carb and very low carb as follows;
“In this review, a low carbohydrate (LC) eating patterns is defined as reducing carbohydrates to 26-45% of total calories [6].”
and
“In this review a very low carbohydrate (VLC) eating pattern is defined as reducing carbohydrate to <26% of total calories [6].”
Diabetes Canada also defines low carbohydrate and very low carbohydrate diets in terms of the amount of carbohydrate the diet contains. Low carbohydrate diets are defined as less than <130 g of carbohydrate per day or <45% energy as carbohydrate, and very low carbohydrate diets as <50 g of carbohydrate per day [7].
[August 8, 2020: You can read more about the use of a Very Low Carbohydrate Diet (VLCD) used as Medical Nutrition Therapy for type 2 diabetes in the following article, posted here.]
Weight-Loss “Keto” Diets
There are a wide range of weight-loss approaches that have a ketogenic (keto) component to them.
The 1997 Protein Power[8] published by Dr. Micheal Eades and his wife Dr. Mary Dan Eades is a low carb, high protein, moderate fat ketogenic diet. In fact, the authors warn in the book that eating a large number of calories as fat would make it impossible to lose weight, so this is not a high fat diet at all.
The New Atkins For a New You [9], was redesigned in 2010 by Dr. Eric Westman, Dr. Stephen Phinney MD PhD, and Dr. Jeff Volek RD PhD, and while considered a low carbohydrate high fat, moderate protein weight loss diet, it has 4 phases, with only the first phase being ketogenic (20-50 g carbs per day), but only for two weeks. This first stage is where the Modified Ketogenic Diet (MKD) used in epilepsy and seizure disorder came from — but as a weight-loss diet, the high fat stage in The New Atkins for a New You is very short lived. In phase two, more carbohydrate is added (nuts & seeds, berries, cherries and melon, cheese, dairy products, legumes (pulses), tomato juice and vegetable cocktail) and this level is maintained until close to goal weight when higher carbohydrate amounts are added in phase 3, then phase 4. It is only higher fat for the first two weeks.
Then there is the 2013 Real Meal Revolution [10] by Tim Noakes, Sally-Ann Creed, Jonno Proudfoot which is a handbook on the Banting lifestyle (which originated in the late 1800s), with foods broken down into green list, orange list and red list, with varying levels of carbohydrate intake.
Note: there is also the 2014 Bulletproof Diet by former Silicon-Valley biohacker, Dave Asprey but since he doesn’t have a clinical background, I have not included it. That said, the diet is very high fat and is where “bulletproof coffee” (with added butter and coconut oil) comes from.
In 2016, Dr. Jason Fung, a Toronto nephrologist (kidney specialist) wrote the Obesity Code [11] which promotes a high fat version of a very low carb / keto diet, which is used in conjunction with his 2016 book written with Jimmy Moore titled The Complete Guide to Fasting [12]. In 2020, Fung published Life in the Fasting Lane [13], written with Eve Meyer and Megan Remos which builds on his approach of using a low carb high fat diet along with intermittent fasting.
In 2014, the web site “Diet Doctor” was launched by Dr. Andreas Eenfeld. This was initially mostly with articles translated from his Swedish site and later added content from a variety of other people, including Dr. Jason Fung, Dr. Eric Westman and Dr. Ted Naiman. In 2017, Eenfeld wrote his own diet book titled Low Carb High Fat Food Revolution [14], which promoted a high fat version of a very low carb / ketogenic weight loss diet. Later, Dr. Eric Westman went on to found his own Adapt weight loss program which is a very low carb / keto, moderate protein, moderate fat approach and Dr. Ted Naiman went on to write his P:E Diet [15] which promotes a low carb, high protein, low fat approach.
Of ketogenic weight-loss diets outlined above, the two that promote a very high fat intake are Dr. Jason Fung’s approach, and the “Diet Doctor” approach. While both fat and protein result in satiety (not feeling hungry), fat has almost two and a half the caloric density as protein. In addition, fat can trigger the reward system of the brain in the same way carbs do, resulting in many over-eating fat, especially added fat. What many people fail to take into consideration is that both of these approaches also promote periods of intermittent fasting (IF) which as Diet Doctor teaches may be frequent periods of less than 24 hours, to longer fasting periods which may include 5:2 (5 days of normal diet, 2 days restricting total calories to 500 per day) or alternate day fasting, as well as two types of fasts that Dr. Fung promotes, including 36 hour fasts, and 42 hour fasts. If one is only eating ~1/3 of the time, is any weight loss really due to the high fat diet, or the fasting?
“In our clinic, we will often recommend 36-hours fasts 2-3 times per week for type 2 diabetes.” ~Dr. Jason Fung
[ADDED NOTE, August 24, 2020: a well-formulated ketogenic diet such as used by Virta Health (covered here and here) which is high in fat and moderate in protein and that consists of a diet of real, whole food is not the same as popularized “keto diets” high in fat and moderate protein, but that consist of lots of added fat, in both food and beverages. There is more to a well-designed ketogenic diet for remission of type 2 diabetes and obesity than macros, alone.
August 27, 2020: There is a fundamental difference between a well-designed ketogenic diet that is high in fat and that is comprised of real, whole food — and the popularized “keto diet”, which is all about added fat. It’s not about macros, but nutrients.]
Unintended Consequences of Believing That a High Fat Diet is THE “Keto Diet”
Over the last several years, about 1/3 of people that come to me do so after following one of these popular high fat “keto” diets. Most lost some weight initially and then stalled — and quite a few actually ended up gaining weight.
Whether following Dr. Fung’s approach or the Diet Doctor approach, people reported eating 75% fat, 15% protein and 10% carbohydrate — which is essentially a hybrid between the Modified Ketogenic Diet (MKD) and the Modified Atkins Diet (MAD) which as mentioned above are NOT weight loss diets — in fact, they were designed to not result in weight loss. These high fat, moderate protein diets are diets are solely intended to produce large amounts of ketones for therapeutic purposes.
It is no wonder high fat “keto” diets don’t deliver weight loss results. That’s not what they were designed to do!
Unless these high fat “keto” diets are combined with the frequent periods of <24 hours of fasting, >24 hour periods of fasting several times per week, weight loss is unlikely to occur — unless as byproduct of the higher satiety of the fat, and over all eating less food.
Losing Body Fat is Not About Eating Less Carbs and More Fat!
If we want to lose body fat, then eating food that is very high in dietary fat won’t accomplish that — UNLESS one is only eating every second or third day, which is what high fat “keto” diets promote. If we are eating a high fat diet and regularly fasting for extended periods of time, it is the fasting itself that underlies body fat loss and lower insulin, not all the added dietary fat.
Eating tons of bacon, butter, cream and avocado makes perfect sense in a therapeutic diet for epilepsy, seizure disorder or as an adjunct treatment in glioblastoma or Alzheimer’s disease, because the goal is to produce lots of ketones — but if one wants to lose weight without using frequent periods of fasting, then adding tons of fat to food makes no sense. We want to utilize our fat stores for energy, not burn dietary fat.
One can use any one of a number of low carbohydrate approaches to accomplish weight loss, as well as improve blood sugar — by focusing on eating nutrient dense foods with a high protein-to-energy ratio, and that are rich in micronutrients. Protein also increases satiety, helps build muscle and is much less calorically dense than fat [16].
Whether starting at a brief ketogenic level and working up (such as the method used by Protein Power, New Meal Revolution or Westman, Phinney and Volek’s approach in the New Atkins, or using an approach I often do which is to start people off at 130 g of carbohydrate per day, and lower carbohydrate as required to achieve clinical outcomes. In either approach, weight loss and lower insulin and glucose can be achieved without extended or frequent periods of fasting.
That doesn’t mean there aren’t benefits to doing short daily periods of fasting, such as from after dinner on one day until the first meal the following day — there are. It simply isn’t required for weight loss.
Final Thoughts…
There are several therapeutic ketogenic diets that can be used in epilepsy and seizure disorder as well as other conditions, and other types of therapeutic ketogenic diets that are considered Medical Nutrition Therapy (MNT) for the treatment of type 2 diabetes and obesity.
The idea that “a keto diet” has to be high in fat is a fallacy — one that has the unintended consequence of many people failing to lose weight (and often gaining weight) because they don’t realize that it needs to be combined with periods of intermittent fasting.
A weight-loss “keto diet” that is 75% fat, 15% protein and 10% carbs is only one type of ketogenic diet. It is by no means “THE keto diet!”. A diet that is low in carbohydrate and rich in nutrient-dense lean protein, as well as a wide range of vegetables and fruit is just as much a “keto diet” because it is low in carbohydrate — and one that can be used successfully to achieve weight loss, with no fasting required.
In short, there is no one-size-fits-all-low-carb or keto diet, but rather a range of low carb and keto diets that can be chosen from, based on each person’s personal preference, as well as their specific medical needs.
More Info?
If you would like more information about type of low carb or ketogenic diet that might be best suited to you, please send me a note using the Contact Me form on the tab above.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchfRD/
Instagram: https://www.instagram.com/lchf_rd
References
- Feinman RD, Pogozelski WK, Astrup A, Bernstein RK, Fine EJ,Westman EC, et al. Dietary Carbohydrate Restriction as the First Approach in Diabetes Management: critical review and evidence base. Nutrition. 2015;31(1):1—13
- Nasir H. Bhanpuri, Sarah J. Hallberg, Paul T. Williams et al, Cardiovascular disease risk factor responses to a type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: an open label, non-randomized, controlled study, Cardiovascular Diabetology, 2018, 17(56)
- U.S. Department of Health and Human Services: Final MNT regulations. . Federal Register, 1 November 2001.
- Peterman MG, The Ketogenic Diet, JAMA. 1928;90(18):1427—1429. doi:10.1001/jama.1928.02690450007003
- Kossoff EH, Doward JL. The Modified Atkins Diet. Epilepsia 2008; 49 (Suppl8): 37-41
- Evert, AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014
- Diabetes Canada, Diabetes Canada Position Statement on Low Carbohydrate
Diets for Adults with Diabetes: A Rapid Review Canadian Journal of Diabetes (2020), doi: https://doi.org/10.1016/j.jcjd.2020.04.001.
- Eades M, Dan Eades M (1997), Protein Power: The High-Protein/Low-Carbohydrate Way to Lose Weight, Feel Fit, and Boost Your Health–in Just Weeks! Bantam; New edition edition (1 December 1997)
- Westman E, Phinney SD, Volek J, (2010) The New Atkins for a New You – the Ultimate Diet for Shedding Weight and Feeling Great, Atria Books February 17, 2010)
- Noakes T, Creed S-A, Proudfoot J, et al, (2013)The Meal Real Revolution, Quivertree Publications
- Fung J (2016) Obesity Code, Greystone Books, Vancouver
- Fung J, Moore J (2016), The complete guide to fasting : heal your body through intermittent, alternate-day, and extended fasting, Victory Belt Publishing
- Fung J, Meyer E and Ramos M (2020), Life in the Fasting Lane: The Essential Guide to Making Intermittent Fasting Simple, Sustainable, and Enjoyable, Harper Wave
- Eenfeld A, Low Carb, High Fat Food Revolution: Advice and Recipes to Improve Your Health and Reduce Your Weight (2017), Skyhorse Publishers
- Naiman T, Shewfelt W, The PE Diet: Leverage your biology to achieve optimal health (2020)
- Paddon-Jones D, Westman E, Mattes RD et al, Protein, weight management, and satiety, The American Journal of Clinical Nutrition, Volume 87, Issue 5, May 2008, Pages 1558S—1561S, https://doi.org/10.1093/ajcn/87.5.1558S
Copyright ©2020 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.


 The Stages of Change are Precontemplation, Contemplation, Preparation, Action, Maintenance and Relapse.
The Stages of Change are Precontemplation, Contemplation, Preparation, Action, Maintenance and Relapse.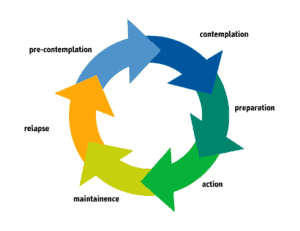







 I am from a family of people that always ‘battled with their weight’.
I am from a family of people that always ‘battled with their weight’. When I became overweight and then obese, and developed type 2 diabetes and high blood pressure, I justified that I was at high risk since both of my parents had the same. I realize now that the “high risk” was our shared diet and lifestyle, more than genetics. Our shared comorbidities were adopted.
When I became overweight and then obese, and developed type 2 diabetes and high blood pressure, I justified that I was at high risk since both of my parents had the same. I realize now that the “high risk” was our shared diet and lifestyle, more than genetics. Our shared comorbidities were adopted.










 I
I