
Therapeutic ketogenic diets such as the classic Ketogenic Diet (KD) or the Modified Ketogenic Diet (MKD) are used in the management of epilepsy or seizure disorder or as adjunct therapy in the treatment of glioblastoma and these diets have a purpose; to produce very high levels of ketones that are used by the body to minimize seizures, or to lower glucose availability to cancer cells. If one does not have a therapeutic need for very high levels of ketones, why eat a very high fat diet that produces lots of them? Why add lots of added fat to diet that is already high in fat? Likewise, if one is eating a high protein low fat diet like P:E in order to build muscle and lose body fat, what is the benefit to eating even more protein? Are there any risks or possible downsides to eating more protein in a high protein low fat diet, or more fat in a low carb high fat diet? How can a low carb high protein diet avoid the problem of excess fat or excess protein?
Eat Fat to Lose Fat?
Some people have come to believe that they need to eat more dietary fat in order to burn body fat, so they add copious amounts of fat to food in the form of heavy whipping cream, butter, fatty meats and to make sure, they supplement with “fat bombs”. If one is trying to lose body fat, then it makes no sense to add tons of dietary fat that will be used by the body for energy before using their own body fat stores. A very high fat version of a LCHF diet may have a role at the very beginning in order to help people make the transition from being predominantly glucose-burning to being fat-burning (referred to as becoming “fat adapted“), but there is no need to keep eating a very high fat diet (75% of energy as fat) once that has occurred. In fact, for many people, continuing to eat 75% fat “keto” diet after the initial adoption often (but not always) results in a stall in weight loss, and in some cases in weight gain — especially when not also doing extended periods of fasting. Fat is two and a half times as energy-dense as protein and carbohydrate, so unless one needs very high levels of ketones for therapeutic purposes and is not concerned about losing muscle mass from extended periods of fasting (more about that here), it makes no sense to keep eating lots of fat.
High Fat Diet Needed for Satiety?
Some people believe that eating high dietary fat on a low carbohydrate diet is needed to keep them from feeling hungry— and that it is this which results in them eating less. While fat does keep people from feeling hungry (i.e. produces increased ‘satiety’), it is not the best source of satiety. Protein is far better at producing satiety, and at less than half the calories of fat. According to a 2010 study titled Energy Density of Foods: Effect on Energy Intake [1];
”when the satiating effects of macronutrients on appetite and energy intake (EI) are compared as nutrients come in the diet (and fat contributes disproportionately to energy density (ED), Joule-for-Joule, protein is consistently (at doses above 1.2 to 1.4 MJ) more satiating than carbohydrate (CHO), which is more satiating than fat.
When energy density (ED) is controlled, protein is still far more satiating than fat or carbohydrate.”
Since protein produces more satiety than fat and has less than half the calories, it makes much more sense for someone seeking weight loss to eat more protein in the diet, and not add excess dietary fat.
Impact of High Fat on Blood Glucose Control
For blood glucose improvements, dietary fat has no impact on the body’s (endogenous) insulin levels, so adding dietary fat does not help lower circulating levels of insulin or blood glucose (blood sugar). It is only the “low carbohydrate” part of a low carb high fat (LCHF) diet that helps improve insulin levels, and in turn glucose levels and it is for this reason that a low carbohydrate diet (defined as <130 g of carbs per day) has been approved by the American Diabetes Association for both improved blood sugar control and weight loss [2] and is why the American Diabetes Association’s Consensus report of April 2019 also includes use of a very low carb (keto) diet of 20-50 g carbs per day [3]. for blood sugar management. Since it is only the low carbohydrate part of a low carb high fat (LCHF) diet that is important for glucose control, keeping carbohydrate low is the goal (not keeping fats high).
For people with pre-diabetes, type 2 diabetes or for those at increased risk due to past medical history or family risk factors, selecting the level of carbohydrate intake that is most appropriate for blood glucose control around prioritizing protein intake based on physiological need, is the first step and the remainder of the diet will be made up of various types of dietary fat. Since the level of fat intake will be above the “not more than 30% of calories from fat” that the USDA defines as a “low fat diet” [4], this diet pattern will still be considered a “high fat diet“.
Depending on whether fat or protein is higher, this type of meal pattern will be either a low carb high fat (LCHF) diet or a low carb high protein (LCHP) diet. More on this second one, below.
Determining Protein Needs without Exceeding the Safe Upper Limit
Protein needs are always calculated as grams of protein per kilogram of body weight of the person and not as a percentage of daily calories e.g. X % of daily energy as protein. This is to ensure adequacy and avoid the d excess.
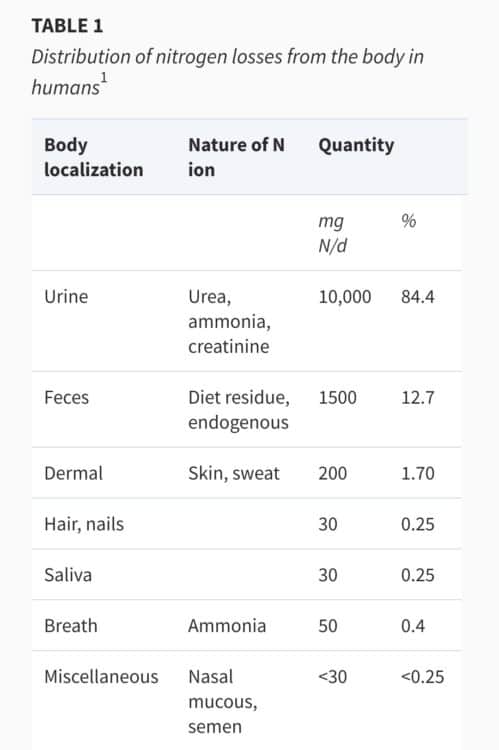
When protein is eaten, the body must get rid of the nitrogen by-product which is toxic to the body. As can be seen from the table below, the main way the body gets rid of this toxic nitrogen by-product is by turning it into ammonia, and then excreting it as urea in the urine.
Protein intake in high protein diets should not be set as a percentage of daily calories, but as a maximum of 3.2 g protein per kg body weight. This is because an intake of 40% of daily calories as protein for one person may be below the safe upper limit of 3.2 g protein per kg body weight, but for another 40% of calories as protein put them right at the upper limit (more in this article).
How Much Protein is Best?
I often hear the question, ”how much protein is best?” but that depends for whom. Different people have a different protein needs. A healthy man or woman seeking to build muscle has a different protein need than an older adult wanting to reduce the risk of sarcopenia (muscle loss), or someone wanting to prevent protein deficiency.
The amount of protein someone needs depends on many factors, including whether a person is growing, pregnant or lactating (breastfeeding), or has been sick or just had surgery. Even for those who aren’t in these special circumstances, protein needs may be calculated to prevent deficiency, to sustain exercise or to preserve muscle mass in older adults, and each of these calculations are different.
Basic Needs — the Recommended Daily Allowance (RDA) for Protein
The Recommended Daily Allowance (RDA) for any nutrient is the average daily dietary intake level that is sufficient to meet the needs of 97-98 % of healthy people. It is important to keep in mind that the RDA is not the optimal requirement, but the absolute minimum to prevent deficiency.
The RDA for protein for healthy adults is calculated at 0.8 g protein / kg of body weight [7]. A sedentary 70 kg / 154 pound man needs a minimum of 56 g of protein and a sedentary 60 kg / 132 pound woman needs a minimum of 48 g protein per day.
Protein Needs for Active Healthy Adults
For those who are physically active, the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[8] recommend a protein intake of 1.2—2.0 g protein / kg per day to optimize recovery from training, and to promote the growth and maintenance of lean body mass.
Protein Needs for Older Adults
There have been several position statements issued by those that work with an aging population indicating that protein intake between 1.0 and 1.5 g protein / kg per day may best meet the needs of adults during aging [9,10].
For the average, healthy 70 kg / 154 pound sedentary man this would be daily protein intake of 70 -105 g per day and for the average, healthy 60 kg / 132 pound sedentary woman this would be a protein intake of 60-90 g protein per day.
At present, there is very little data for defining the upper limit of protein beyond the urea cycle, which has been established to be safe at 3.0 g protein / kg body weight (tied to the maximum rate of urea production which is 3.2 g protein per kg body weight [6]), so the range of safe intake is defined as >0.8 g protein body/ kg body weight to >2.5 g protein/ kg body weight.

*in clinical practice, I have set a maximum of 2.5 g protein / kg IBW but in practice, Meal Plans have routinely been below 2.0 g protein / kg IBW.
Is “More” Better
There is a tendency for people to think that because a high fat diet is “good” — or a high protein diet is “good”, that “more is better”. This is a bit like thinking that since a certain amount of laundry detergent is “good”, that “more detergent is better”, but before adding “more”, a few questions need to be asked. For example, will the clothes come out any cleaner, or is there a possibility that “more” may cause the suds to overflow the machine? There is a benefit / risk to “more” that first needs to be considered.
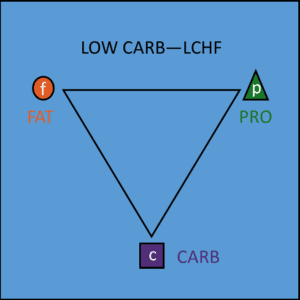 Considering the benefit / risk of more also needs to be considered when contemplating adding “more fat” in a low carb high fat (LCHF) diet (e.g. 75% fat, 15% protein, 10% carbs).
Considering the benefit / risk of more also needs to be considered when contemplating adding “more fat” in a low carb high fat (LCHF) diet (e.g. 75% fat, 15% protein, 10% carbs).
If one needs high ketones for therapeutic reasons, then “more fat” has a benefit — but if weight loss is the goal, then “more fat” may result in a weight stall, or possibly a weight gain. That isn’t a “risk” as one normally thinks of it, but it certainly isn’t a benefit.
“More” may be better, but not always.
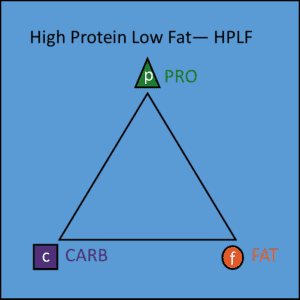 One also needs to consider the benefit / risk of adding “more protein” to a high protein, low fat (HPLF) diet, such as P:E (e.g. 40% protein, 30% carbs, 30% fat).
One also needs to consider the benefit / risk of adding “more protein” to a high protein, low fat (HPLF) diet, such as P:E (e.g. 40% protein, 30% carbs, 30% fat).
If one is eating a diet that provides 2.5 g protein / kg body weight is “good” in order to build up muscle or be a swimsuit model, one has to consider if it is really “better” to eat 3.3 g – 4.4 g protein per kg body weight (1.5 or 2 grams protein per pound).
Just because some “do” does not make it “better”. It has to also be safe.
One has to ask if there are clinical studies that indicate that eating this high amount of protein intake long term is safe, but at present there are not. All we have at present is the safe upper limit based on the rate of urea excretion of 3.2 g protein per kg body weight, so until it is known that “more” is better AND “safe”, staying within this safe upper limit is what is recommended.
Some will argue that since our ancient ancestors ate a largely meat diet that there is no limit on the amount of protein we can eat, however not all “meat” is protein, some is fat. In addition, it is known that our ancient ancestors also had carbohydrate in the diet as berries, above ground vegetables and tubers and recently it was discovered that~ 6,000 years ago, our ancient ancestors from present-day Kenya and Sudan were also eating milk products, which contains carbohydrate.
Dr. Loren Cordain, Professor from the Department of Health and Exercise Science at Colorado State University who is renowned for his work over the last two decades on the evolutionary and anthropological basis for diet estimates the protein intake of our ancient ancestors at 35% of total caloric intake [11].
A Low Carb High Protein (LCHP) Diet
A low carb high protein (LCHP) diet can be either low carbohydrate (<130g of carbs) or very low carbohydrate / ketogenic (20-50 g of carbs) and a low carbohydrate diet, is suitable for people with pre-diabetes or type 2 diabetes for improved glucose control and weight loss. A low carb high protein diet avoids the problem of excess fat or excess protein by prioritizing protein around individual need (outlined above), then limiting carbs to the level most suited to the individual for glycemic (blood sugar) control. The remainder of dietary intake is just enough fat to make everything taste good, and to provide essential fatty acids. The situation of either excess fat or excess protein is avoided.
A high protein low fat (HPLF) diet such as the P:E Diet (40% protein, 30% carbs, 30% fat) is very different. It is a moderate carbohydrate diet of ~130—177 g carbohydrate per day, and is not the most suitable for those already not tolerating higher amounts of carbohydrate intake, such as those with pre-diabetes or type 2 diabetes. It’s good for healthy individuals seeking to build muscle mass; provided dietary intake of protein does not exceed the maximum level of urea excretion.
Final Thoughts…
For those seeking to lose weight or normalize blood glucose levels, a low carbohydrate diet is accepted by both the American Diabetes Association and Diabetes Canada and considered both safe and effective, so either a low carb high fat or low carb high protein diet would be suitable. In either, the percentage of fat is considered “high”, because a “low fat diet” is anything at or below 30% of calories[4]. By definition, since either diet provides more than 30% of energy as fat , they are both considered “high fat” diets.
I think it is more reasonable to consider diets with fat intakes of 30-45% of daily calories as fat as moderate fat diets, and those above that level as “high fat” diets, but this is only my opinion.
Whether one sets fat intake at 50% or 75% of calories depends on an individual’s goals. If a person needs low levels of ketones for therapeutic reasons, or are engaging in regular periods of extended fasting and can handle the extra energy intake of a high fat diet, then for weight loss or blood sugar control, a low carb high fat diet might be a good choice.
For those who don’t have any specific need for ketones, or who practice only daily periods of intermittent fasting (12-16 hours), then for blood sugar control and weight loss, a low carb high protein diet may be a better option.
I have been providing a low carb high fat (LCHF) Meal Plans for the last 5 years and low carb high protein (LCHP) Meal Plans for the last 3 years and design Meal Plans for either.
“There is no one-sized-fits-all low carb or keto diet”.
More Info?
If you are interested in having me design a Meal Plan for you, then please have a look at the Complete Assessment Package under the Services tab (for those in Canada).
If you are outside of Canada and would like me to provide you with Nutrition Education for either low carb high fat or low carb high protein, then please have a look the Meal Plan Package under the Services tab.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchfRD/
Instagram: https://www.instagram.com/lchf_rd
References
- Stubbs J, Ferres S, Horgan G, Energy Density of Foods: Effects on Energy Intake, Critical Reviews in Food Science and Nutrition, 40:6, 481-515, 2010
- American Diabetes Association, Lifestyle Management Standards of Medical Care in Diabetes — 2019. Available at: http://care.diabetesjournals.org/content/42/Supplement_1. Accessed: Dec. 17, 2018.
- Evert AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014
- Institute of Medicine (US) Committee on Examination of Front-of-Package Nutrition Rating Systems and Symbols; Wartella EA, Lichtenstein AH, Boon CS, editors. Front-of-Package Nutrition Rating Systems and Symbols: Phase I Report. Washington (DC): National Academies Press (US); 2010. Appendix B, FDA Regulatory Requirements for Nutrient Content Claims. Available from: https://www.ncbi.nlm.nih.gov/books/NBK209851/
- TomeÌ D, Bos C, Dietary Protein and Nitrogen Utilization, The Journal of Nutrition, Volume 130, Issue 7, July 2000, Pages 1868S—1873S, https://doi.org/10.1093/jn/130.7.1868S
- Rudman D, DiFulco TJ, Galambos JT, Smith RB 3rd, Salam AA, Warren WD. Maximal rates of excretion and synthesis of urea in normal and cirrhotic subjects. J Clin Invest. 1973;52(9):2241-2249. doi:10.1172/JCI107410
- National Academies Press, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids (2005)
- Thomas DT, Erdman KA, Burke LM. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance [published correction appears in Med Sci Sports Exerc. 2017 Jan;49(1):222]. Med Sci Sports Exerc. 2016;48(3):543-568. doi:10.1249/MSS.0000000000000852
- Fielding RA, Vellas B, Evans WJ, Bhasin S, et al, Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011 May;12(4):249-56
- Bauer J1, Biolo G, Cederholm T, Cesari M, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013 Aug;14(8):542-59
- Cordain L, Miller JB, Eaton SB, Mann N, Holt SH, et al. (2000) Plant-animal subsistence ratios and macronutrient energy estimations in worldwide hunter-
gatherer diets. The American Journal of Clinical Nutrition 71(3): 682—692 - Bleasdale, M., Richter, K.K., Janzen, A. et al. Ancient proteins provide evidence of dairy consumption in eastern Africa. Nat Commun 12, 632 (2021). https://doi.org/10.1038/s41467-020-20682-3
Copyright ©2021 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.