
People still think that a “keto diet” is all about eating loads of fat, and while a Low Carb High Fat (LCHF) diet is certainly one way to do ‘keto’, it is by no means the only way — or is it even a single diet. There are therapeutic ketogenic diets for epilepsy and adjunct treatment (along with chemotherapy and radiation) for certain types of cancer, as well as for seeking to improve quality of life outcomes in certain neurological disorders, such as MS. There are also different types of “low carb” and “keto” diets that are used for weight loss and for improving metabolic heath — that range from ones that prioritize fat, to those that prioritize protein. This article outlines some of the key advantages and disadvantages of different types of low carb* and keto** diets that are used for weight loss and normalizing blood sugar.
As outlined here, *low carb is defined as < 130g carbohydrate / day, < 26% of total energy intake and very low carb / **keto diets are defined as 20—50g carbohydrate /day, < 10% total energy intake.
Humans can use protein, fat and carbohydrate for fuel, but our two main energy sources are fat and carbohydrate. While amino acids from the protein we eat can be used to make glucose to maintain blood sugar and to supply red blood cells when there is inadequate food intake, protein’s main role in the diet is NOT as a fuel source, but to provide amino acids (the building blocks of protein) for the body to make its own proteins. Protein is primarily there to provide structure and function, not energy.
Fat and carbohydrate are human’s two primary energy sources — and carbohydrate is entirely optional from a biological perspective.
Even the Dietary Reference Intakes support that carbohydrate in the diet is optional, provided we eat adequate amounts of protein and fat.
Protein and fat are not optional, carbohydrate is.
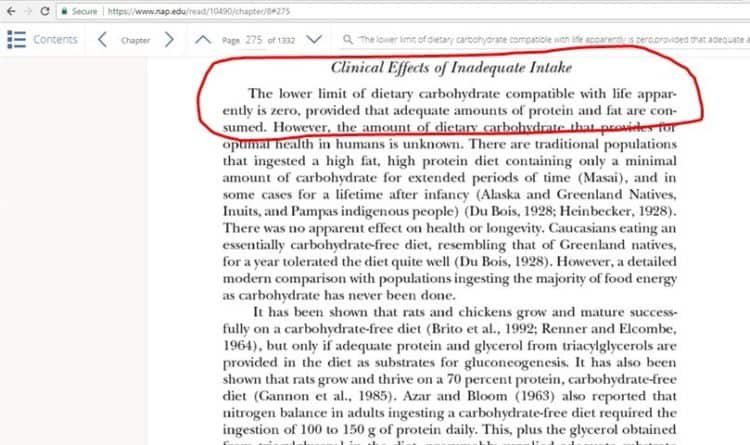
”The lower limit of dietary carbohydrate compatible with life apparently is zero, provided that adequate amounts of protein and fat are consumed.”
Our body has an absolute requirement for specific essential nutrients — and these are called “essential nutrients” because we must take them in through our diet because we can’t synthesize them.
As I wrote about back in 2017, there are 9 essential amino acids that must be supplied in the different kinds of protein that we eat, and include histidine, isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, valine and there are 2 essential fatty acids — linoleic (an omega 6 fat) and alpha-linolenic (an omega 3 fat) that also must be provided in the diet because that can’t be synthesized by the body.
There are also 13 essential vitamins (vitamin A, vitamin B1 (thiamine), B2 (riboflavin), B3 (niacin), B5 (pantothenic acid), B6 (pyrodoxine), B12 (cyanocobalamine), biotin, vitamin C (ascorbic acid), choline, vitamin D (cholecalciferol), vitamin E (tocopherol) and folate), and several essential minerals, including major minerals (calcium, phosphorus, potassium, sodium, chloride and magnesium) and minor minerals (chromium, cobalt, copper, fluorine, iodine, iron, manganese, molybdenum, selenium, silicon, sulfur and zinc).
Of the 3 macronutrients (protein, carbs and fat), protein and fat are not optional because they provide the essential amino acids and essential fats — and with them, many (but not all) of the essential vitamins and essential minerals. The remainder of the essential vitamins and minerals are provided by eating a wide range of vegetables and fruit.
Prioritizing Protein
Whether we eat a Low Carb High Fat (LCHF) diet, or Low Carb High Protein (LCHF) diet, we first need to make sure we are eating adequate amounts of high quality protein for our needs, and with high quality proteins come the essential fats.
 Think of protein as the foundation of a balance scale — providing the body with building blocks for structure and function — and the two arms of a balance scale as the two sources of fuel for energy: carbohydrate and fat.
Think of protein as the foundation of a balance scale — providing the body with building blocks for structure and function — and the two arms of a balance scale as the two sources of fuel for energy: carbohydrate and fat.
We need to have enough protein for our needs, but not so much as to exceed the body’s ability to get rid of the excess nitrogen in our urine (more about that here).
Basic protein requirements are set in the Recommended Daily Allowance (RDA) for protein, which is the level that is sufficient to meet the needs of 97-98 % of healthy people and to prevent deficiency. The RDA for protein for healthy adults is calculated at 0.8 g protein / kg of reference body weight (i.e. IBM) [1]. Remember, this is the bare minimum to prevent deficiency in most people.
For those who are physically active, the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[2] recommend a protein intake of 1.2—2.0 g protein / kg IBW per day to optimize recovery from training, and to promote the growth and maintenance of lean body mass.
Older people also need more protein in order to maintain muscle mass, and prevent sarcopenia (muscle loss associate with aging). There have been several position statements issued by those that work with an aging population indicating that protein intake between 1.0 and 1.5 g protein / kg IBW per day may best meet the needs of adults during aging [3,4].
The Need to “Trade Off” Protein for Ketones
If we need to supply our body with lots of ketones for therapeutic reasons — such as the management of seizure disorder, or as an adjunct treatment for certain types of cancer or neurological disorders, then there is the need to “trade off” supplying the body anything more than the bare minimum of protein, in order to provide it with the very high levels of fat needed to make high levels of ketones.
The classic Ketogenic Diet (KD) has a 4:1 ratio i.e. 4 parts of fat for every 1 part protein and carbs and the Modified Ketogenic Diet (MKD) has a 3:1 ratio i.e. 3 parts fat for every 1-part protein, but unless a person has a therapeutic need for high levels of ketones, then why eat super high levels of fat?
Higher Fat than Carbs – two very different approaches
![]() As outlined in the American Diabetes Association’s April 2019 Consensus Report, a low carb diet has “demonstrated the most evidence for improving glycemia (blood sugar) for individuals with diabetes“[6], so either a Low Carb High Fat diet or a Low Carb High Protein diet are excellent approaches for those with prediabetes or type 2 diabetes seeking to significantly improve their blood sugar, or to put type 2 diabetes into remission.
As outlined in the American Diabetes Association’s April 2019 Consensus Report, a low carb diet has “demonstrated the most evidence for improving glycemia (blood sugar) for individuals with diabetes“[6], so either a Low Carb High Fat diet or a Low Carb High Protein diet are excellent approaches for those with prediabetes or type 2 diabetes seeking to significantly improve their blood sugar, or to put type 2 diabetes into remission.
Popularized “Keto” Diet
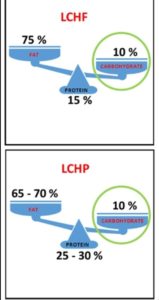
When most people think of a Low Carb High Fat (LCHF) diet, they think of the standard “keto diet” of 75% fat, 15% protein and 10% carbs, which is the popularized high fat approach of Dr. Jason Fung and the Diet Doctor website recommend. As will be outlined below, there are other Low Carb High Fat approaches.
If the goal is to lose weight however, it really doesn’t make a lot of sense to eat tons of fat which provides almost twice as much energy, as either protein or carbs — unless also doing regular periods of intermittent and extended fasting. While people do have success with this type of low carb high fat diet when used this way, this approach has drawbacks for some people.
Intermittent fasting for less than 24 hours has many benefits, but the problem with extended fasting for periods longer than 24 hours is there is a loss of lean body mass (muscle) that goes along with it — which is more of a concern for older adults who are already losing lean body mass, than for younger people.
According to a 1979 research article published in the American Journal of Clinical Nutrition [7], protein is lost during extended fasting beginning on day 1 and continues until it reaches at maximum on day 3, then slowly declines. These results are validated in other studies, including one from Owen and Cahill in 1969 [9,10].

This graph from Virta Health [10] based on the same research [7] shows the losses in grams of nitrogen per day, where each gram represents the loss of about 1 ounce of lean tissue.
 This graph also from Virta Health [9] and based on the same research shows the long-term loss of body nitrogen (protein) as % of pre-fasting value. While loss of protein slows somewhat after day 10, it continues right up to 60 days.
This graph also from Virta Health [9] and based on the same research shows the long-term loss of body nitrogen (protein) as % of pre-fasting value. While loss of protein slows somewhat after day 10, it continues right up to 60 days.
Based on this data, healthy overweight adults who fast for 10 days will lose 5 pounds of lean muscle [9].
According to a 1983 study by by Cahill, normal protein breakdown is ~75 g per day and while protein breakdown will eventually slow by ~25% when people are fasting long term in order to spare muscle, this is only as the ”final stage of adaptation” and only ”once ketoacid levels (ketones) reach a plateau and the brain is preferentially using ketoacids as fuel [10]”.
This time frame is consistent with the research above [9,10] showing that the slowing of muscle loss only occurs after 10 days of fasting, when ketones become the preferred fuel.
It is for this reason that I do not recommend fasting longer than 24 hours for older adults — especially post-menopausal women who are already at risk of sarcopenia (muscle loss), but daily periods of intermittent fasting (from the end of dinner until the first meal of the day, the following day) is recommended to help normalize blood sugar and circulating levels of insulin.
Another shortcoming with the popularized “keto” macros is that 15% protein may be insufficient for an older adult or for someone to sustain regular physical activity (more here).
For younger adults and those who are not trying to build muscle, this approach can be very helpful for losing weight and controlling blood sugar levels.
A “Well-Formulated” Ketogenic Diet
Another approach which falls in the Low Carb High Fat (LCHF) category are the recommendations of Dr. Stephen Phinney and Dr. Jeff Volek from their book The Art and Science of Low Carbohydrate Living — which recommends ~60-70% fat, 20%-up to 30% protein, and 10% carbohydrate [11].
This style of low carb high fat diet provides up to 30% protein, which is almost twice as much protein as the popularized keto’ diet, which is only 15% protein — and as outlined in an earlier article is insufficient for older adults, as well as people sustaining regular physical activity.
Low Carb High Protein
In a sense, a Low Carb High Protein (LCHP) diet which provides ~25-30% protein really falls at the higher end of the range of Dr. Stephen Phinney and Dr. Jeff Volek’s approach of 20% — up to 30% protein and provides a similar fat range of 65-70% fat, and 10% carbs.
As a “low carb diet” it offers all the benefits for lowering blood sugar, and as such is ideal for those seeking to put pre-diabetes or type 2 diabetes into remission.
It is also ideal for those seeking weight loss without periods of extended fating, as it does not have excessive fat, and provides sufficient protein for older adults and those who participate in regular physical activity.
Final Thoughts…
 Both a Low Carb High Fat diet and Low Carb High Protein diet are low carb — so both are great for controlling blood sugar.
Both a Low Carb High Fat diet and Low Carb High Protein diet are low carb — so both are great for controlling blood sugar.
A Low Carb High Protein diet has almost twice the protein as a Low Carb High Fat diet — so, great for older adults and those who exercise regularly.
Protein provides satiety (feeling full) for almost half the calories as fat –so, great for weight loss.
If there is no need for a person to have very high levels of ketones, than a person should select which low carb or keto diet they follow on the basis of first meeting their protein needs. Then they can select the amount of carbohydrate that best meets their blood glucose goals. Finally, they can add a little fat to make things taste good as their essential fats come with their protein.
More Info?
If you are interested in learning more about my services, please have a look at the Services tab. At the top are services provided as a Registered Dietitian to those in Canada, and at the bottom are Nutrition Education services provided to those outside of Canada.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchfRD/
Instagram: https://www.instagram.com/lchf_rd
References
- National Academies Press, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids (2005)
- Thomas DT, Erdman KA, Burke LM. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance [published correction appears in Med Sci Sports Exerc. 2017
- Fielding RA, Vellas B, Evans WJ, Bhasin S, et al, Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011 May;12(4):249-56
- Bauer J1, Biolo G, Cederholm T, Cesari M, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013 Aug;14(8):542-59
- Kossoff EH, Doward JL. The Modified Atkins Diet. Epilepsia 2008; 49 (Suppl8): 37-41
- Evert, AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With
Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014 - G B Forbes, E J Drenick, Loss of body nitrogen on fasting, The American Journal of Clinical Nutrition, Volume 32, Issue 8, August 1979, Pages 1570—1574, https://doi.org/10.1093/ajcn/32.8.1570
- Owen OE, Felig P, Morgan AP, Wahren J, Cahill GF Jr. Liver and kidney metabolism during prolonged starvation. J Clin Invest. 1969 Mar;48(3):574-83. doi: 10.1172/JCI106016. PMID: 5773093; PMCID: PMC535723.
- Phinney SD, Volek JS, To Fast of Not to Fast: what are the Risks of Fasting?, December 5, 2017, Virta Health, https://www.virtahealth.com/blog/science-of-intermittent-fasting
- Cahill GF Jr. President’s address. Starvation. Trans Am Clin Climatol Assoc. 1983;94:1-21.
- Volek JS, Phinney SD, The Art and Science of Low Carbohydrate Living: An Expert Guide, Beyond Obesity, 2011
Copyright ©2021 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.