
The human body is able to use carbohydrate, fat or protein to generate energy, however only carbohydrate and fat are major fuel sources. Protein’s role in the diet is mainly to provide amino acids needed by the body to make its own proteins, for structure and function.
During digestion, carbohydrate, fat and protein from food are broken down into their basic components — carbohydrates are broken into simple sugar and turned into glucose, proteins are broken down into amino acids, and fat is broken down into fatty acids and glycerol.
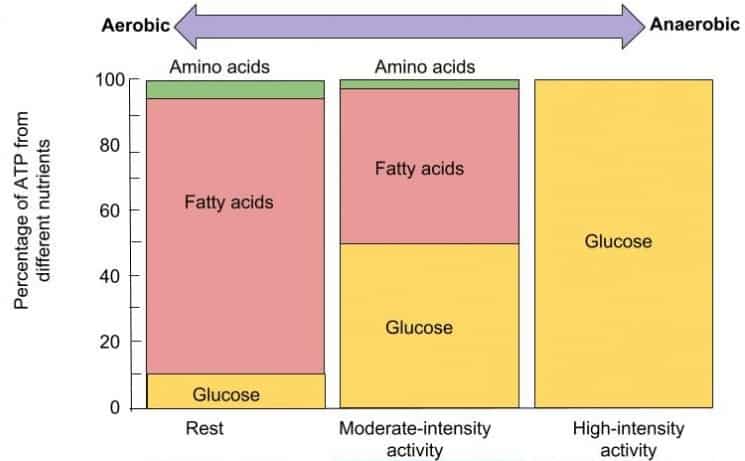
During moderate-intensity exercise, our body will use half fatty acids as fuel and half glucose. During high-intensity exercise our body will rely on glucose as fuel — both from the carbohydrates we ate, as well as generated by breaking down fat stores. It is only if we are not getting enough calories in our food or from our fat stores that protein will be used for energy[2] and burned as fuel. If more protein is eaten than is needed by the body, the excess will be broken down and stored as fat [2].
Determining Individual Macros
 In determining the amount of protein, fat and carbohydrate that each individual needs (i.e. “macros”), choosing the amount of protein we require comes first. The amount of carbohydrate and fat is chosen after that — based on the needs of the individual for blood sugar control and their metabolic health.
In determining the amount of protein, fat and carbohydrate that each individual needs (i.e. “macros”), choosing the amount of protein we require comes first. The amount of carbohydrate and fat is chosen after that — based on the needs of the individual for blood sugar control and their metabolic health.
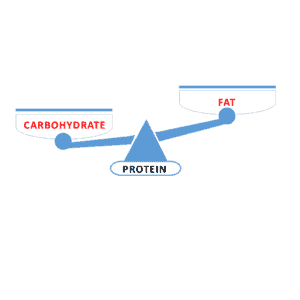
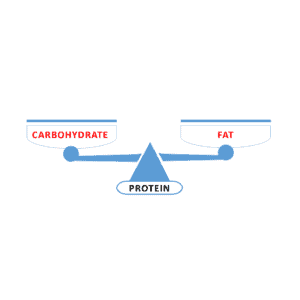
Since it is not a primary fuel source for the body, think of protein as the base of a balance scale — providing the body with building blocks for structure and function. The two arms of the balance are the two sources of fuel for energy: carbohydrate and fat.
How do we choose the amount of protein we need?
We need to have enough protein for our needs, but not so much as to either store the excess as fat — or worse, to exceed the ability of our body to get rid of the excess nitrogen-by-product in the urine. Since 84% of the nitrogen waste produced from protein intake is excreted as urea in the urine[3], the safe upper limit of protein intake is based on the maximum rate of urea production which is 3.2 g protein per kg of ideal body weight [4] i.e. lean body mass.
NOTE: this calculation is based on lean body mass (also known as Ideal Body Weight or Ideal Body Mass (IBW), not total body weight. Lean body mass is essentially one’s total body weight minus the amount of fat they have.
Lean body mass can be assessed using a DEXA scan, or estimated by using relative fat mass (RFM). The amount of fat someone has can be estimated from total body weight (taken on a scale), minus their estimated RFM as described in this article.
Once we know a person’s lean body mass, we can use the equation (3.21 g of protein / kg lean body mass) to determine the maximum amount of protein they can eat on an ongoing basis while being able to safely dispose of the ammonia via urea through urine.
Basic protein requirements are set in the Recommended Daily Allowance (RDA) for protein, which is the level that is sufficient to meet the needs of 97-98 % of healthy people and to prevent deficiency. The RDA for protein for healthy adults is calculated at 0.8 g protein / kg of reference body weight (i.e. IBM) [5]. Remember, this is the bare minimum to prevent deficiency in most people.
For those who are physically active, the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[6] recommend a protein intake of 1.2—2.0 g protein / kg IBW per day to optimize recovery from training, and to promote the growth and maintenance of lean body mass.
Older people also need more protein in order to maintain muscle mass, and prevent sarcopenia (muscle loss associate with aging). There have been several position statements issued by those that work with an aging population indicating that protein intake between 1.0 and 1.5 g protein / kg IBW per day may best meet the needs of adults during aging [7,8].
Balancing Carbohydrate and Fat as Fuel
There are 3 ways that carbohydrate and fat as fuel can be balanced — and which one is best for a specific individual depends on their protein needs (outlined above), as well as their metabolic health.
Higher Carbohydrate than Fat
 The standard American (and Canadian) diet recommended by national dietary guidelines aims for the majority of fuel (energy intake) to come from carbohydrate.
The standard American (and Canadian) diet recommended by national dietary guidelines aims for the majority of fuel (energy intake) to come from carbohydrate.
These diets are High Carb, Low Fat (HCLF) diets.
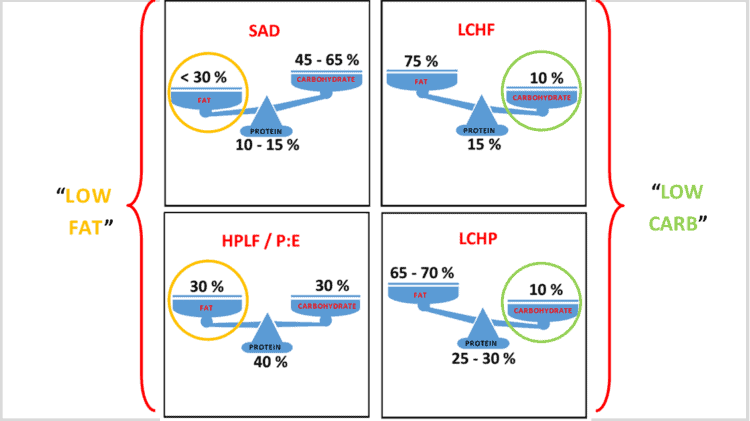
They are “high carb” because they provide >225g – 300 g carbohydrate / day, 45-65% of total energy intake.
They are “low fat” as they provide “not more than 30% of calories from fat [9].
For those who are metabolically healthy, a high carbohydrate diet where carbohydrate sources are unrefined whole grains (include the husk and the bran), as well as unprocessed starchy vegetables such as yam, peas and winter squash is certainly one option. The problem is that 88% of Americans are already metabolically unwell [10], with presumably a large percentage of Canadians as well (more about that here).
People who are already showing indications that they are not tolerating carbohydrate well; manifest either as high HOMA-IR, pre-diabetes or type 2 diabetes might do better to select another option for their main fuel source — especially given that the American Diabetes Association (ADA) consensus report on Diabetes and pre-diabetes published on April 2019 indicated that;
”Reducing overall carbohydrate intake for individuals with diabetes has demonstrated the most evidence for improving glycemia and may be applied in a variety of eating patterns that meet individual needs and preferences[11].”
Higher Fat than Carbohydrate
Low Carb, High Fat (LCHF) diets are one type of diet that provides more fuel (energy) from fat, than from carbohydrate. There is another type, outlined below.
These range from the popularized “keto diet” of Dr. Jason Fung and the Diet Doctor website which typically provide ~75% fat, 15% protein, ~10% carbohydrate — to the recommendations of Dr. Stephen Phinney and Dr. Jeff Volek from their book The Art and Science of Low Carbohydrate Living which recommends ~60-70% fat, 20%-up to 30% protein, and 10% carbohydrate [12].
These are considered “low carb” diets when they provide < 130g carbohydrate / day, < 26% of total energy intake and “very low carb” (ketogenic) diets when they provide 20—50g carbohydrate / day, < 10% total energy intake — based on the definition from Feinman et al [13] which defines very low carbohydrate, low carbohydrate, and moderate carbohydrate diets as follows:
1. very low carbohydrate diet: 20—50g carbohydrate /day, < 10% total energy intake
2. low carbohydrate diet: < 130g carbohydrate / day, < 26% of total energy intake
3. moderate carbohydrate diet: 130—225g carbohydrate / day, 26—45% of total energy intake
The same definitions of “low carbohydrate” and “very low carbohydrate” are also used in the clinical guidelines of the American Diabetes Association [11], as well as Diabetes Canada [15] where these are meal pattern options for those with diabetes and pre-diabetes to control blood sugar.
Balanced Fat and Carbs
This type of diet is a High Protein, Low Fat (HPLF) diet and the best-known is the P:E Diet of Dr. Ted Naiman.
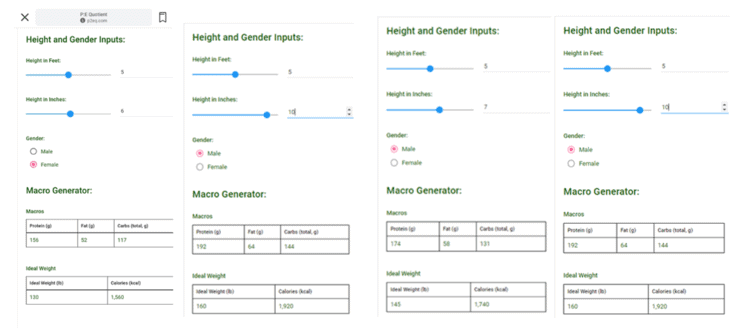
The P:E Diet is “high protein” diet – recommending 40% protein with equal amounts of fat (30%) and carbohydrate (30%) — as generated by the P:E ratio Macro Calculator (located at the bottom of www.p2eq.com);
The P:E diet is “low fat” as it provides “not more than 30% of calories from fat [9].
For the most part, the P:E diet is “moderate carb” — providing ~130—225g carbohydrate per day — although for some weights and heights, the carbohydrate content is slightly below the 130 g carbs / day cut-off for “low carb” (see examples from the P to E Macro Calculator, above).
While a high protein intake makes sense for those seeking to build and sculpt muscle, as outlined in this previous article setting the recommendation for protein at 40% of dietary intake (instead of as “g protein per kg body weight“) results in protein sometimes coming close to exceeding the excretion rate for urea of 3.2 g protein per kg reference body weight.
This could be avoided if the P:E Macro Calculator was set a maximum limit of protein of 3.0 g protein / per kg body weight.
Low Carbohydrate High Protein
A Low Carb High Protein (LCHP) diet provides ~25-30% protein, which is significantly higher than the 10-20% protein of the standard American (or Canadian diet), yet without the possibility of exceeding the urea excretion capacity of the kidney as protein intake is set to up to 2.5 grams protein per kg body weight (which is well below the maximum of 3.2 g protein / kg ideal body weight).
Having high protein, it offers more satiety at less than half the calories of fat [16] — which makes much more sense for someone seeking weight loss.
Like the Low Carb, High Fat diets of Dr. Jason Fung and Diet Doctor (~75% fat, 15% protein, ~10% carbohydrate) this diet is “high fat“, and provides 65-70% fat. In a sense, a Low Carb High Protein meal pattern reflects the higher end of the range of Dr. Stephen Phinney and Dr. Jeff Volek’s approach of ~60-70% fat, 20%-up to 30% protein, and 10% carbohydrate.
This meal patterns provides a wide range of fats from olive oil and avocado oil to (depending on the lipid profile of the person) butter and coconut oil. Most of the fat provided in the diet is not from added fat, but from fat that comes along with protein — such as the fat in meat, cheese, nuts or yogurt.
Most significantly, this meal pattern is “low carb” (< 130g carbohydrate / day) or “very low carb” / ketogenic — providing ~20—50g carbohydrate / day and as a low carb diet “has demonstrated the most evidence for improving glycemia” [11].
For those seeking fat loss but already having difficulty handling carbohydrate, a Low Carb High Protein (LCHP) meal pattern offers the “best of both worlds”.
It offers the benefits of being able to build new muscle, as well as lower the risk of muscle loss.
It also offers the higher satiety of high protein — without the possibility of exceeding the body’s ability to excrete ammonia in the urine.
…and it is “low carb” — providing the improved blood sugar control that “low carb” is known for.
Final Thoughts…
Humans only have two primary fuel sources, so meal patterns such as Low Carb High Fat, Low Carb High Protein and P:E (High Protein Low Fat) always come down to a choice between “low carb” or “low fat“.*
*theoretically, one could set all 3 macros at 33% each — making the meal pattern neither low fat or low carb — but to what end?
Whether low carb or low fat is the most suitable for someone depends on their protein needs and metabolic health.
I started out 5 years ago teaching low carb from a Low Carb High Fat (LCHF) perspective, and for the last 3 years have also provided a Low Carb High Protein (LCHP) meal pattern.
For those seeking to improve blood sugar or put type 2 diabetes into remission, either one of the low carb options work, however it has been my experience that peri- and post-menopausal women often do much better on the higher protein version of a low carb diet when it comes to weight loss.
Over the last few months, I have also been asked to provide metabolically healthy people with a P:E / HPLF Meal Plan — which I do, although I set an upper limit on protein intake to a maximum of 2.0 g protein per kg ideal body weight.
Different people have different goals and health needs, which is why I offer more than one type of meal pattern. While a P:E diet is just on the edge of “low carb” — it is very much “low carb” when compared with the Standard American (and Canadian) diet.
There is no one-sized-fits-all low carb or ketogenic diet.
More Info?
If you are interested in having me design a Meal Plan for you, then please have a look at the Complete Assessment Package under the Services tab (for those in Canada).
If you are outside of Canada and would like me to provide you with Nutrition Education for either low carb high fat or low carb high protein, then please have a look the Meal Plan Package under the Services tab.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchfRD/
Instagram: https://www.instagram.com/lchf_rd
References
- Fuel Sources. (2020, August 13). Retrieved May 24, 2021, from https://med.libretexts.org/@go/page/7071
- Youdim A, Merck Manual, Carbohydrates, Proteins and Fats, https://www.merckmanuals.com/en-ca/home/disorders-of-nutrition/overview-of-nutrition/carbohydrates-proteins-and-fats
- TomeÌ D, Bos C, Dietary Protein and Nitrogen Utilization, The Journal of Nutrition, Volume 130, Issue 7, July 2000, Pages 1868S—1873S, https://doi.org/10.1093/jn/130.7.1868S
- Rudman D, DiFulco TJ, Galambos JT, Smith RB 3rd, Salam AA, Warren WD. Maximal rates of excretion and synthesis of urea in normal and cirrhotic subjects. J Clin Invest. 1973;52(9):2241-2249. doi:10.1172/JCI107410
- National Academies Press, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids (2005)
- Thomas DT, Erdman KA, Burke LM. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance [published correction appears in Med Sci Sports Exerc. 2017
- Fielding RA, Vellas B, Evans WJ, Bhasin S, et al, Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011 May;12(4):249-56
- Bauer J1, Biolo G, Cederholm T, Cesari M, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013 Aug;14(8):542-59
- Institute of Medicine (US) Committee on Examination of Front-of-Package Nutrition Rating Systems and Symbols; Wartella EA, Lichtenstein AH, Boon CS, editors. Front-of-Package Nutrition Rating Systems and Symbols: Phase I Report. Washington (DC): National Academies Press (US); 2010. Appendix B, FDA Regulatory Requirements for Nutrient Content Claims. Available from: https://www.ncbi.nlm.nih.gov/books/NBK209851/
- Araíºjo J, Cai J, Stevens J. Prevalence of Optimal Metabolic Health in American Adults: National Health and Nutrition Examination Survey 2009—2016. Metabolic Syndrome and Related Disorders Vol 20, No. 20, pg 1-7, DOI: 10.1089/met.2018.0105
- Evert, AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014
- Volek JS, Phinney SD, The Art and Science of Low Carbohydrate Living: An Expert Guide, Beyond Obesity, 2011
- Feinman RD, Pogozelski WK, Astrup A, Bernstein RK, Fine EJ,Westman EC, et al. Dietary Carbohydrate Restriction as the First Approach in Diabetes Management: critical review and evidence base. Nutrition. 2015;31(1):1—13
- Diabetes Canada, Diabetes Canada Position Statement on Low Carbohydrate
Diets for Adults with Diabetes: A Rapid Review Canadian Journal of Diabetes (2020), doi: https://doi.org/10.1016/j.jcjd.2020.04.001 - Stubbs J, Ferres S, Horgan G, Energy Density of Foods: Effects on Energy Intake, Critical Reviews in Food Science and Nutrition, 40:6, 481-515, 2010
Copyright ©2021 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.