While there are many different types of low carbohydrate and “keto” diets circulating on the internet, how do the three most common compare in terms of protein intake, adequacy or excess, namely;
(a) the low carb high fat (LCHF) “keto” diet best known through Diet Doctor and Dr. Jason Fung,
(b) the higher protein, lower fat (nutritional ketosis) dietary approach used for weight loss by Drs. Phinney and Volek in their book The Art and Science of Low Carbohydrate Living
and
(c) the very high protein, low fat (HPLF) Protein to Energy (P:E) ratio diet of Dr. Ted Naiman.
For healthy people*, how do each of these diets compare? Is protein adequate compared to the RDA? Is protein enough to sustain someone who is physically active or enough for an older adult? Is protein within the safe upper limit or does it exceed the maximum level of amount of protein based on the disposal of ammonia in urea in the urine?
*response to different macro levels may be different in those with type 2 diabetes.
Note: this article is Part 2 of 2. Be sure to read the preceding article titled How Much Protein is Best Depends on Different People’s Needs.
Each of these diets will be evaluated in terms of:
- Is protein adequate based on the RDA?
- Is protein enough to sustain someone who is physically active?
- Is protein enough for an older adult?
- Is protein within the safe upper limit?
- Does protein exceed the maximum level of amount of
protein based on the disposal of ammonia in urea in the urine?
√ – meets the criteria
X – does not meet the criteria
A – Protein Intake in the High Fat “Keto Diet”
The well-known high fat “keto” diet that is 75% fat, 10% carbs and 15% protein is only one of many keto diets. The amount of protein is not based on body weight, but is a percentage of energy. A diet which is 75% fat means there is lots of added fat in the form of whipping cream, avocado, bacon and fatty meat in order to make up for the very low carbohydrate intake (10%) and only 15% of calories allotted to protein.
A 100 kg man (220 pounds) with an energy consumption of 2500 kcal/day would be eating 1875 calories / 208g as fat, 250 calories / 62g as carbs and 375 calories / 94g as protein.
A 60 kg woman (132 pounds) with an energy consumption of 2000 kcals/day would be eating 1500 calories / 166 g as fat, 150 calories / 37.5 g as carbs and 225 calories / 56g as protein.
Does this amount meet people’s needs?
For the 100 kg man;
√ Is protein adequate based on the RDA? His protein intake based on the RDA of 0.8 g protein / kg body weight [1] so his basic needs are only 80g, so this diet is adequate at 94 g. Remember, this is the minimum amount of protein needed to meet the needs of 97-98% of healthy individuals, not an optimal amount.
X Is protein enough to sustain someone who is physically active? Based on the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[2] which recommends and intake of 1.2—2.0 g protein / kg per day, his protein intake needs to be 120 g – 200 g per day to sustain physical activity, so is inadequate at 94g.
X Is protein enough for an older adult? Based on recent position papers [3,4] his protein intake needs to be between 1.0 and 1.5 g protein / kg per day, which is 100 – 150 g per day, and is inadequate at 94g.
√ Is protein within the safe upper limit? The highest end of the range of safe intake of protein is 2.5 g protein/ kg per day and at 94 g of protein, his intake is below 250 g protein per day based on his weight, so it is safe.
√ Does protein exceed the maximum level of amount of protein based on the disposal of ammonia in urea in the urine? A 100 kg man (220 pounds) with 20% body fat would have 80 kg lean mass and would have a maximum protein ceiling of ~256g/day (based on the maximum amount of ammonia disposal of 3.21 g of protein / kg of lean body mass). His intake is only 94 g or protein, so it is safe.
For the 60 kg woman;
√ Is protein adequate based on the RDA? Her protein intake based on the RDA of 0.8 g protein / kg body weight [1] needs to be only be 48g, so is adequate at 56 g to prevent deficiency.
X Is protein enough to sustain someone who is physically active? Based on the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[2] which recommends and intake of 1.2—2.0 g protein / kg per day, her protein intake would need to be 72 g – 120 g per day to sustain physical activity, so is inadequate at 56g.
X Is protein enough for an older adult? Based on recent position papers [3,4] her protein intake would need to be between 1.0 and 1.5 g protein / kg per day, which is 60 – 90 g protein per day, so is inadequate at 56 g.
√ Is protein within the safe upper limit? The highest end of the range of safe intake of protein is 2.5 g protein/ kg per day and at 56 g of protein, her intake is below 150g protein per day based on her weight, so it is safe.
√ Does protein exceed the maximum level of amount of protein based on the disposal of ammonia in urea in the urine? A 60 kg (132 pound) woman with 25% body fat, would have 45 kg of lean mass, and based on energy consumption of 2000 kcals/ day would have a maximum protein ceiling of 144 g/day. Her intake of 56 g of protein in safe.
B – The Higher Protein, Lower Fat Ketogenic Dietary approach
This approach used for weight loss by Drs. Phinney and Volek in their book The Art and Science of Low Carbohydrate Living works out to approximately 60-70% fat, 20% up to 30% protein and 10% carbohydrate (Nutritional Ketogenic), but the macros are determined based on ideal body weight, which is estimated by lean body mass.
From page 210 of their book [6];
”…our studies of muscle retention and function during carbohydrate restriction, we recommend daily protein intakes between 1.5 and 2.5 grams per day per kg of reference body weight [6].”
What would this amount of protein look like in terms of intake?
A man who is 5’9″³ (1.75 m) tall and weighs 100 kg ( 220 pounds) has an IBW (lean body mass) of 155 pounds (70 kg), so protein intake should be 105 g – 175.0 g protein.
A woman who is 5″² 4 “³(1.63 m) tall and weighs 60 kg (132 pounds) has an IBW (lean body mass) of 127 pounds (55 kg), so protein intake according to Phinney and Volek should be between 82.5 g – 137.5 g protein.
For the 100 kg man;
√ Is protein adequate based on the RDA? His protein intake based on the RDA of 0.8 g protein / kg body weight [1] would need only be 80g, so is adequate between 105 g – 175 g protein.
√ Is protein enough to sustain someone who is physically active? Based on the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[2] which recommends and intake of 1.2—2.0 g protein / kg per day, his protein intake would need to be 120 g – 200 g per day to sustain physical activity, so is adequate between 105 g – 175 g protein.
√ Is protein enough for an older adult? Based on recent position papers [3,4] his protein intake would need to be between 1.0 and 1.5 g protein / kg per day, which is 100 – 150 g per day, and is adequate between 105 g – 175 g protein.
√ Is protein within the safe upper limit? The highest end of the range of safe intake of protein is 2.5 g protein/ kg of total weight per day, so is safe at 2.5 g protein IBW (i.e. 70 kg / 155 pounds) which is total intake of 105 g – 175 g protein.
√ Does protein exceed the maximum level of amount of protein based on the disposal of ammonia in urea in the urine? A 100 kg man (220 pounds) with 20% body fat would have 80 kg lean mass, so would have a maximum protein ceiling of ~256g/day (based on the maximum amount of ammonia disposal of 3.21 g of protein / kg of lean body mass). His intake between 105 g – 175 g protein is safe.
For the 60 kg woman;
√ Is protein adequate based on the RDA? Her protein intake based on the RDA of 0.8 g protein / kg body weight [1] would need only be 48g, so is adequate at 82.5 g – 137.5 g protein. Remember, this is the minimum amount of protein needed to meet the needs of 97-98% of healthy individuals.
√ Is protein enough to sustain someone who is physically active? Based on the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[2] which recommends and intake of 1.2—2.0 g protein / kg per day, her protein intake would need to be 72 g – 120 g per day to sustain physical activity, so is adequate at 82.5 g – 137.5 g protein.
√ Is protein enough for an older adult? Based on recent position papers [3,4] her protein intake would need to be between 1.0 and 1.5 g protein / kg per day, which is 60 – 90 g per day, and is adequate at 82.5 g – 137.5 g protein.
√ Is protein within the safe upper limit? The highest end of the range of safe intake of protein is 2.5 g protein/ kg per day and at 82.5 g – 137.5 g protein her intake is below 150g protein per day based on her weight, so it is safe.
√ Does protein exceed the maximum level of amount of protein based on the disposal of ammonia in urea in the urine? A 60 kg (132 pound) woman with 25% body fat, would have 45 kg of lean mass, and based on energy consumption of 2000 kcals/ day would have a maximum protein ceiling of 144 g/day. Her intake of 82.5 g – 137.5 g protein is safe.
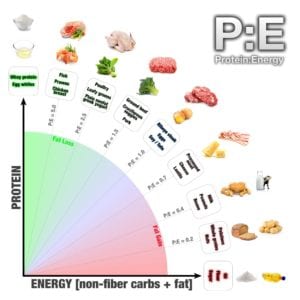
C – Very High Protein, Low Fat Protein to Energy (P:E) Ratio Diet
By definition, the P:E ratio diet (40% protein, 30% carbs, 30% fat) is a High Protein Low Fat diet, as fat is at or below the USDA low fat cutoff of 30% — based on the P:E ratio calculator located at www.p2eq.com.
It is largely a moderate carbohydrate approach (130-225g carbs per day), but for some weights and heights generates carbs of just under 130g / day, the cutoff for low carb.
Based on that calculator:
A man who is 5’9″³ (1.75 m) tall should weigh 155 pounds (70 kg). According to this calculator and assuming this man is metabolically healthy, he should should eat 1,860 kcals as 186 g protein (2.66 g pro/kg IBW), 62 g of fat and 140 g of total carbs.
A woman who is 5″² 4″³ (1.63 m) should weigh 120 pounds (55 kg). According to this calculator and assuming she is metabolically healthy, this hypothetical woman should eat 1,440 kcals per day as 144 g protein (2.67 g protein /kg IBW), 48 g of fat and 108 g of total carbs.
For the 100 kg man;
√ Is protein adequate based on the RDA? His protein intake based on the RDA of 0.8 g protein / kg body weight [1] would need only be 80g, so is more than adequate at 186g.
√ Is protein enough to sustain someone who is physically active? Based on the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[2] which recommends and intake of 1.2—2.0 g protein / kg per day, his protein intake would need to be 120 g – 200 g per day to sustain physical activity, so is more than adequate at 186g.
√ Is protein enough for an older adult? Based on recent position papers [3,4] his protein intake would need to be between 1.0 and 1.5 g protein / kg per day, which is 100 – 150 g per day, and is more than adequate at 186g.
√ Is protein within the safe upper limit? The highest end of the range of safe intake of protein is 2.5 g protein/ kg per day and at 186 g of protein, his intake is below 250g protein per day based on his weight, so it is safe.
√ Does protein exceed the maximum level of amount of protein based on the disposal of ammonia in urea in the urine? According to the online calculator, a man who is 5’9″³ (1.75 m) tall should weigh 155 pounds (70 kg), and eat 1,860 kcals as 186 g protein but in this case, he weighs 100 kg (220 pounds) and has 30% body fat. Safe intake is based on his LBM so the fact that he is overweight makes no difference. Based on the maximum amount of ammonia disposal of 3.21 g of protein / kg of lean body mass his maximum amount of protein would be 225 g / day, so 186 g protein is safe.
For the 60 kg woman;
√ Is protein adequate based on the RDA? Her protein intake based on the RDA of 0.8 g protein / kg body weight [1] would need only be 48g, so is more than adequate at 144 g.
√ Is protein enough to sustain someone who is physically active? Based on the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine[2] which recommends and intake of 1.2—2.0 g protein / kg per day, her protein intake would need to be 72 g – 120 g per day to sustain physical activity, so is more than adequate at 144 g.
√ Is protein enough for an older adult? Based on recent position papers [3,4] her protein intake would need to be between 1.0 and 1.5 g protein / kg per day, which is 60 – 90 g per day, and is more than adequate at 144 g.
√ Is protein within the safe upper limit? The highest end of the range of safe intake of protein is 2.5 g protein/ kg per day and at 144 g of protein, her intake is below 150g protein per day based on her weight, so it is safe.
√ / X? Does protein exceed the maximum level of amount of protein based on the disposal of ammonia in urea in the urine? According to the online calculator, a woman who is 5″² 4″³ (1.63 m) should weigh 120 pounds (55 kg). should eat 1,440 kcals per day as 144 g protein (576 kcal / 1440 kcals = 40% protein). Based on the maximum amount of ammonia disposal of 3.21 g of protein / kg of lean body mass [5], her maximum amount of protein is 144 g / day, so she is at the very high end of the safe range.
Note: When a high protein diets include supplementation with whey protein (such as the P:E ratio encourages by listing it as one of the best protein to energy sources) it is much easier to exceed the upper limit of protein and exceed the capacity of the body to excrete the ammonia as urea. It should be noted that this is much more difficult to do eating only real, whole food.
Final Thoughts…
Which low carbohydrate dietary approach is best for you will depend on your protein needs. If you want to make sure to have enough protein to be very active or to preserve muscle as an older adult, then the popularized high fat “keto” diet would not necessarily be the best approach.
If you don’t want to exceed the safe range of protein intake and the capacity of your body to get rid of ammonia, yet want to eat a very high protein, low fat diet, then be sure to do the calculations.
I think that the safest approach is the one Drs. Phinney and Volek recommend and which meet the needs of a wide range of people from the very active to older adults and with protein intakes that are well within the safe range of protein intake and a outlined in a recent article, Drs. Phinney and Volek along with Dr. Brittanie Volk updated their recommendations for protein in 2018 to be between 1.5 and 1.75 grams of protein per kg of reference body weight [7] from the earlier 1.5 and 2.5 grams per day per kg of reference body weight [6] — which puts protein recommendations well within the safe range, while meeting or exceeding the needs of a wide range of people.
More Info?
If you would like more information about my services then please have a look under the tab of that name or send me a note through the Contact Me form.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/lchfRD
Facebook: https://www.facebook.com/lchfRD/
Instagram: https://www.instagram.com/lchf_rd
References
- National Academies Press, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids (2005)
- Thomas DT, Erdman KA, Burke LM. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance [published correction appears in Med Sci Sports Exerc. 2017 Jan;49(1):222]. Med Sci Sports Exerc. 2016;48(3):543-568. doi:10.1249/MSS.0000000000000852
- Fielding RA, Vellas B, Evans WJ, Bhasin S, et al, Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011 May;12(4):249-56
- Bauer J1, Biolo G, Cederholm T, Cesari M, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013 Aug;14(8):542-59
- Rudman D, DiFulco TJ, Galambos JT, Smith RB 3rd, Salam AA, Warren WD. Maximal rates of excretion and synthesis of urea in normal and cirrhotic subjects. J Clin Invest. 1973;52(9):2241-2249. doi:10.1172/JCI107410
- Volek JS, Phinney SD, The Art and Science of Low Carbohydrate Living: An Expert Guide, Beyond Obesity, 2011
- Phinney SD, Volek JS, Volk B, How Much Protein Do You Need In Nutritional Ketosis? February 21, 2018, Virta Health, https://www.virtahealth.com/blog/how-much-protein-on-keto
Copyright ©2021 The LCHF Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.


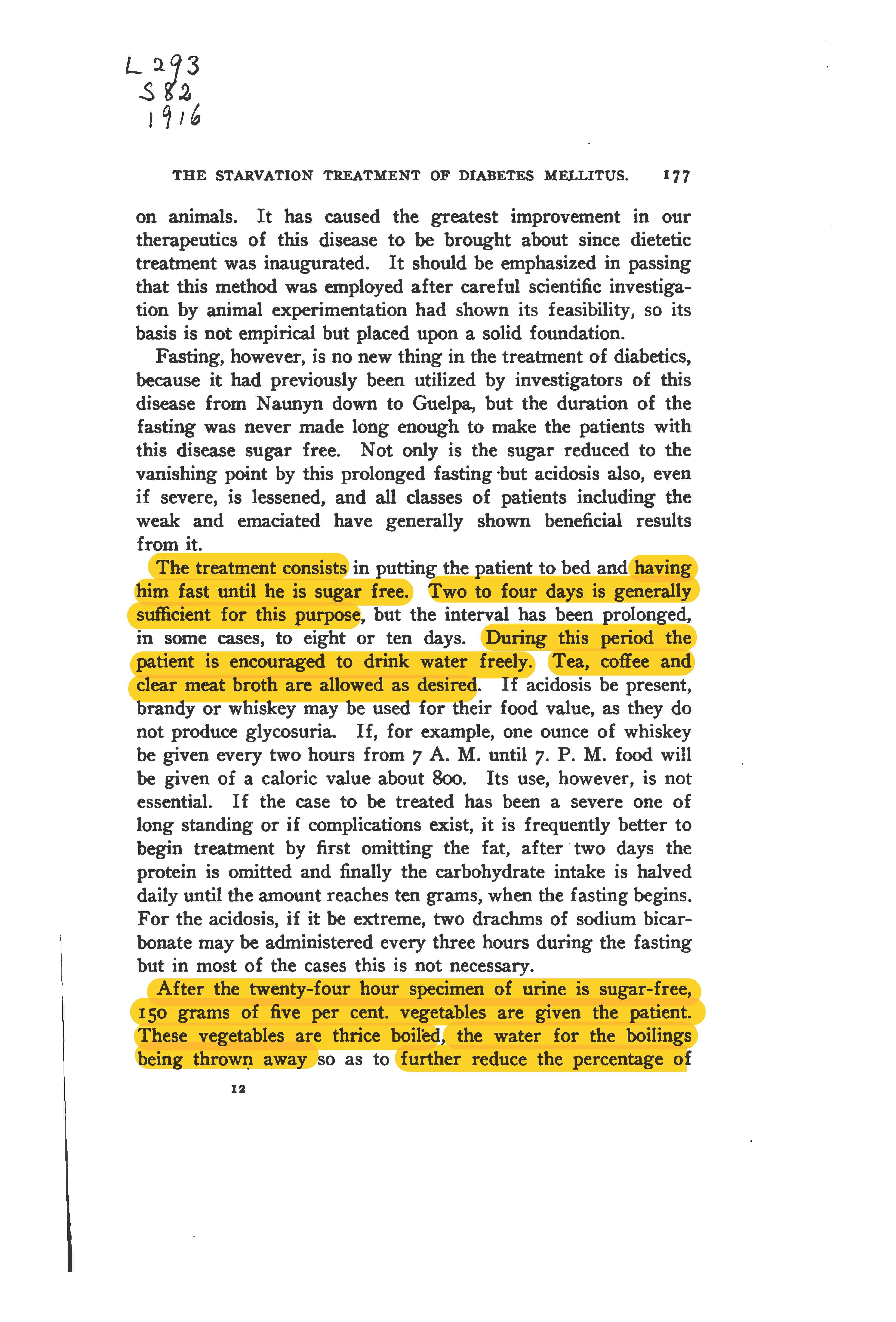
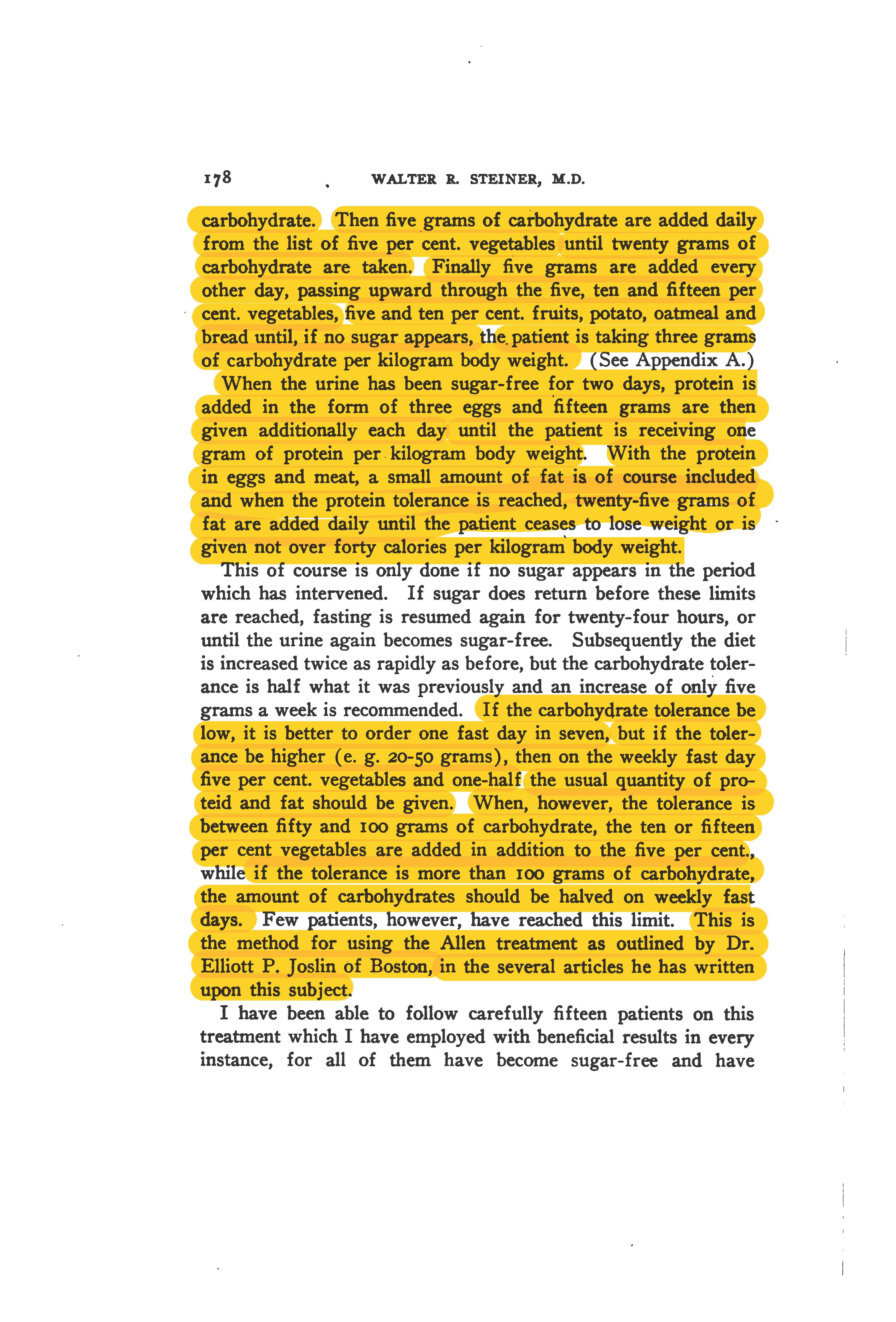
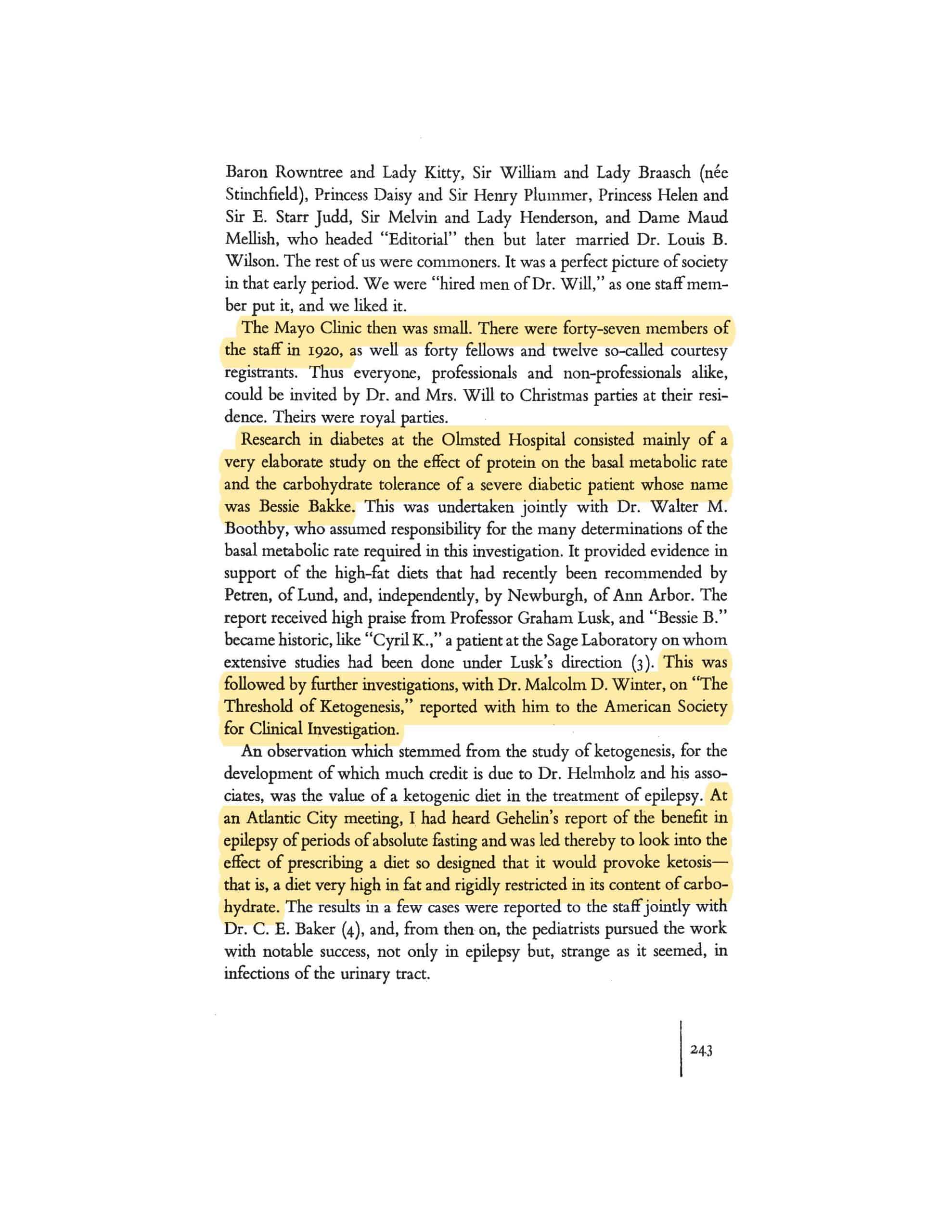
 A hundred years ago, Dr. Russell M. Wilder and two Dietitians from the Mayo Clinic wrote a 69-page book titled “A Primer for Diabetic Patients – A Brief Outline of The Principles of Diabetic Treatment, Sample Menus and Food Tables[1]” which outlined the treatment of diabetes using different levels of a low carbohydrate and very low carbohydrate (ketogenic) diet, as well as short periods (12-48 hours) of fasting.
A hundred years ago, Dr. Russell M. Wilder and two Dietitians from the Mayo Clinic wrote a 69-page book titled “A Primer for Diabetic Patients – A Brief Outline of The Principles of Diabetic Treatment, Sample Menus and Food Tables[1]” which outlined the treatment of diabetes using different levels of a low carbohydrate and very low carbohydrate (ketogenic) diet, as well as short periods (12-48 hours) of fasting.
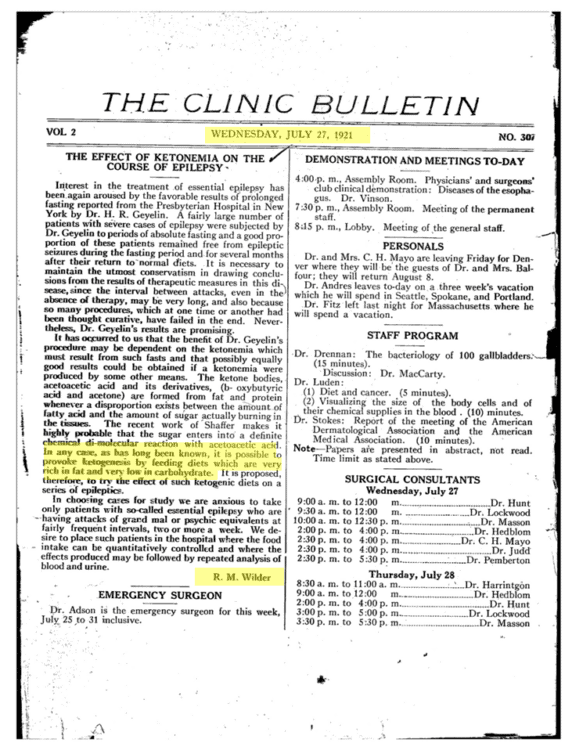
 “Insulin at that time cost five cents a unit in the market. However,
“Insulin at that time cost five cents a unit in the market. However,  In Wilder’s 1958 paper, he outlines how the
In Wilder’s 1958 paper, he outlines how the  “The actual procedure will vary with different patients, but, in general, foods of known composition in weighted amounts are fed, the total intake of carbohydrate, protein and fat being increased very gradually as high as possible without the return of sugar in the urine.”
“The actual procedure will vary with different patients, but, in general, foods of known composition in weighted amounts are fed, the total intake of carbohydrate, protein and fat being increased very gradually as high as possible without the return of sugar in the urine.”
 A
A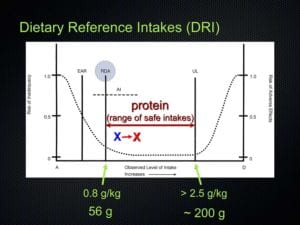

 We also know from a 2015 study on the effect of food order on the response of glucose and insulin, that
We also know from a 2015 study on the effect of food order on the response of glucose and insulin, that  The American Diabetes Association understands that a low carbohydrate diet ”limits sugar, cereals, pasta, bread, fruit & starchy vegetables” and “consist mostly of protein foods like meat and dairy, fatty foods like oil, nuts, seeds, avocado, and butter, and non-starchy vegetables” [2].
The American Diabetes Association understands that a low carbohydrate diet ”limits sugar, cereals, pasta, bread, fruit & starchy vegetables” and “consist mostly of protein foods like meat and dairy, fatty foods like oil, nuts, seeds, avocado, and butter, and non-starchy vegetables” [2].




 We didn’t expect to encounter snow when we set out up the trail, but there was plenty of it about half way up and it got heavier. It made things slippery. I hadn’t yet bought mud or ice ‘crampons’, but I soon realized I would need these next.
We didn’t expect to encounter snow when we set out up the trail, but there was plenty of it about half way up and it got heavier. It made things slippery. I hadn’t yet bought mud or ice ‘crampons’, but I soon realized I would need these next.




 This morning I decided to take pictures of what I look like currently, and have started on a new goal of re-attaining my previous weight by what would have been my father (of blessed memory)’s birthday.
This morning I decided to take pictures of what I look like currently, and have started on a new goal of re-attaining my previous weight by what would have been my father (of blessed memory)’s birthday.

 There are a number of websites that encourage people to use their tools to reach their weight loss goals faster.
There are a number of websites that encourage people to use their tools to reach their weight loss goals faster.
 When I cite references in my articles, it is to support the evidence for what I am writing about. As much as possible, I prefer to cite academic, peer-reviewed research papers — which means that not only are they written by experts in the field, the papers are first reviewed by other experts in the field (i.e. peer-reviewed) before the findings are published in a journal.
When I cite references in my articles, it is to support the evidence for what I am writing about. As much as possible, I prefer to cite academic, peer-reviewed research papers — which means that not only are they written by experts in the field, the papers are first reviewed by other experts in the field (i.e. peer-reviewed) before the findings are published in a journal.
 When she came to see me the first time, I was only one year into my own weight-loss and health-recovery “journey”, and was still very much overweight and metabolically unwell, but had come to understand from the scientific literature that a well-designed low carbohydrate diet was both safe and effective for weight loss, as well as for helping put some metabolic conditions into remission.
When she came to see me the first time, I was only one year into my own weight-loss and health-recovery “journey”, and was still very much overweight and metabolically unwell, but had come to understand from the scientific literature that a well-designed low carbohydrate diet was both safe and effective for weight loss, as well as for helping put some metabolic conditions into remission.  In April 2019, Karen private messaged me on social media and sent me a photo of herself, after she had lost 150 pounds. It was both delightful and very rewarding to receive this from a client and to see that she had continued to apply what she had learned, and was doing exactly what she set out to do. She gave me permission to share it on social media with only her first name and initial of her last name, which I did. All people knew is that this was what one client had accomplished in a year.
In April 2019, Karen private messaged me on social media and sent me a photo of herself, after she had lost 150 pounds. It was both delightful and very rewarding to receive this from a client and to see that she had continued to apply what she had learned, and was doing exactly what she set out to do. She gave me permission to share it on social media with only her first name and initial of her last name, which I did. All people knew is that this was what one client had accomplished in a year. Last week instead of private messaging me an update, Karen decided to post a compilation photo of herself under one I had posted of myself on Facebook. Even though I had not spoken to her in over a year, there was her picture for everyone, including me, to see! Wow!! Karen had lost more than 200 pounds, and had every reason to be proud of her accomplishment!
Last week instead of private messaging me an update, Karen decided to post a compilation photo of herself under one I had posted of myself on Facebook. Even though I had not spoken to her in over a year, there was her picture for everyone, including me, to see! Wow!! Karen had lost more than 200 pounds, and had every reason to be proud of her accomplishment!