This article is based on a lecture given by Gabor Erdosi, MSc, MBA— Food News Conference, May 19, 2018 — Prague, Czech Republic
Introduction — Gabor Erdosi, MSc, MBA is a Molecular Biologist from Debrecen, Hungary who is employed in the Food Industry but whose hobby is reading scientific publications and analyzing the available information. The talk that this article is based on was given at the Food News Conference, May 19, 2018 — Prague, Czech Republic and is the condensation of approximately 4 years worth of Gabor’s studying of the literature.
Gabor founded and heads up the Lower Insulin group on Facebook which is dedicated to discussing the scientific basis of the relationship between metabolic diseases and food and lifestyle factors. At present, the group has ~5300 members.
This new series titled The Perils of Food Processing reflects Gabor’s conviction that what’s of primary importance in the interaction between food and our physiology (GI tract) is the speed and location of food absorption in the digestive system. This article is arranged according to the same principle.
The reason I am writing this series of articles is because I believe what Gabor Erdosi has come to understand about the effects of food processing on the speed and location of food absorption — especially carbohydrate, and which affects the very nature of hunger and satiety is absolutely crucial to understanding the current epidemic of metabolic diseases we now face.
This first article provides an overview of the gastrointestinal system and the so-called “incretin hormones” and how the amount a food is cooked or ground impacts how quickly it is absorbed and the energy stored.
When talking about Food Processing, the issue arises as to how to properly define the concept of processing’.
How do we define ‘food processing’? Humans have been processing their food in one way or another for hundreds of thousands of years — be it cutting, cooking or grinding their food in some way. These are all forms of food processing.
In terms of the effect of Food Processing on human physiology, a few main questions that this series of articles will address, arise;
(i) are all forms of food processing created equal?
(ii) does the food processing of different macronutrients and foods have different results?
(iii) could these changes in food processing over the last few hundred years or so have anything to do with the epidemic of metabolic diseases that we now face?
1. Overview of Gastrointestinal Physiology
Before getting into the topic of the effect of different types of food processing on the speed and place of absorption, it’s necessary to provide an overview of the gastrointestinal physiology and how the digestive system works and what hormones are released in response to different nutrients.

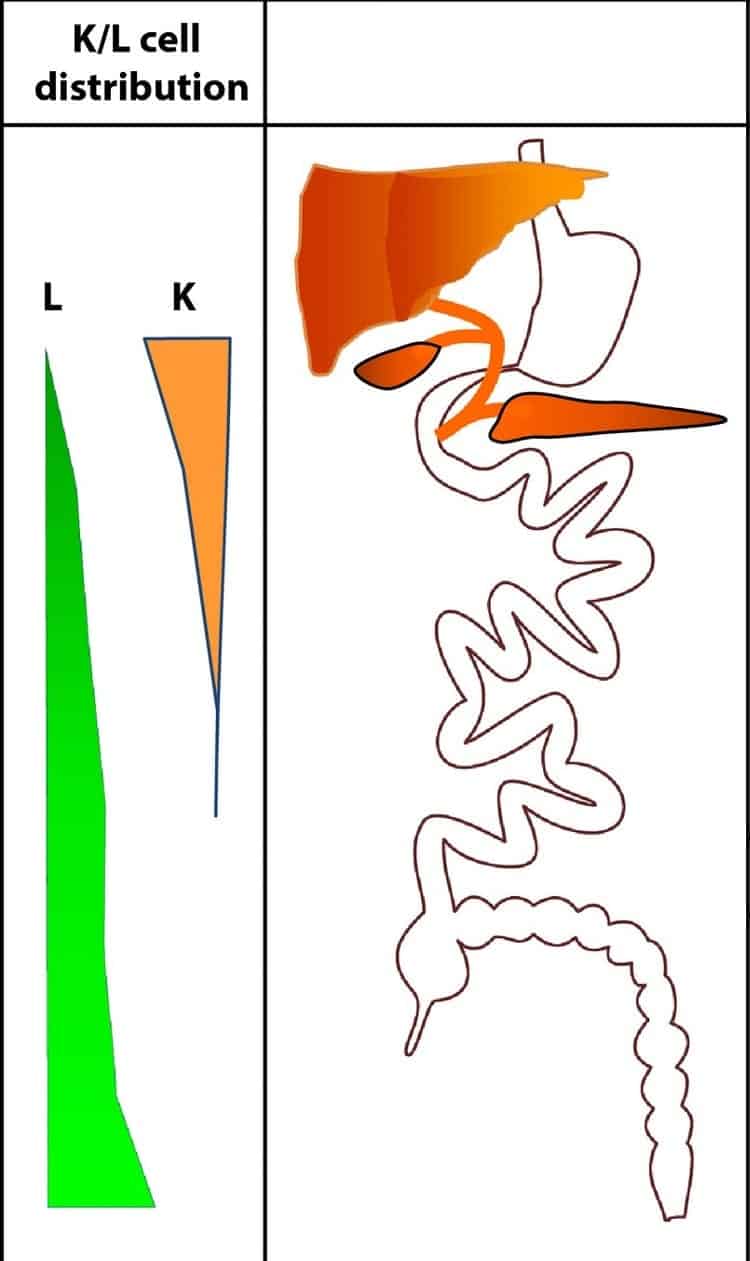
The important concept here is that we have ”sensor cells” (K-cells, L-cells) within our gastrointestinal tract and these cells release different hormones in response to different nutrients.
K-cells release an incretin hormone called GIP and the L-cells release an incretin hormone called GLP-1, as well as GLP-2, PYY and Oxyntomodulin (OXM).
What is important to note is that the distribution of these cells is not uniform.
The K-cells are more abundant in the upper part of the small intestine and other cells, the L-cells are more abundant in the lower part of the small intestine. This uneven distribution of these incretin-hormone-releasing sensor-cells has profound implications, as will be seen later.
2. Nutrient Sensing, the Incretin Effect and Hunger-Satiety Signalling in the Gut
Nutrient-Sensing
So, what happens when we eat foods that we have evolved to see for millennia? As the food goes through the small intestine, it triggers hormonal release from these incretin-hormone-releasing sensor-cells.
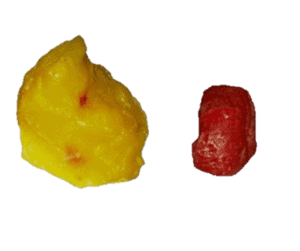
If you eat meat and berries, for example, which are foods we have evolved to see for hundreds of thousands of years, they have a fairly balanced stimulatory effect on these sensor cells. These incretin hormones will be released in a more or less balanced manner.
However, as will be shown later on, when we eat food products that we have not evolved to see — relatively new food products on an evolutionary scale, these patterns are completely disrupted.
There are several nutrient-sensing hormones in the small intestine, but the one to focus on with respect to the effect of food processing is SGLT1 – which is a glucose sensor. Both the K-cells and the L-cells contain this nutrient-sensing receptor, and most others, as well.
Keep in mind for the next articles that the distribution of these cells is uneven; with more in the K-cells higher up in the small intestine and increasing numbers further down in the L-cells.
The Incretin Effect
When we eat glucose, such as in an oral glucose tolerance test or when someone gets intravenous glucose in a hospital, the difference in the insulin response is called the ”incretin effect”.
As you can see from the diagram below, the response to an oral or intravenous glucose load is very large and can be 50-70% of the insulin response.

The majority of the insulin response is stimulated by these incretin hormones (GIP, GLP-1, etc.) secreted by the K-cells and L-cells and not directly via glucose.
The Physiological Effects of the Incretin Hormones
In addition to the insulin-stimulating effect, these incretin hormones have very different effects.
The K-cells, which are more abundant in the upper small intestine, secretes Glucose-dependent Insulinotropic Polypeptide (GIP) which acts on the pancreas — not only to result in insulin release, but also increase glucagon. At the level of the fat cells, the adipose tissue, it increases increases triglyceride storage, resulting in weight gain. In this way, GIP supports insulin’s effect on storing lipids. This is an anabolic-type of hormone and if it is very high, it can cause inflammation in adipose tissue.
The L-cells, which are more abundant in the lower small intestine, secrete Glucagon-like Peptide-1 (GLP-1) which also acts on the pancreas to increase insulin, but decreases glucagon. This GLP-1 at the level of the brain, acts to decrease appetite, increase satiety (feeling full) and decrease food intake.
- Hunger-Satiety Signalling in the Gut
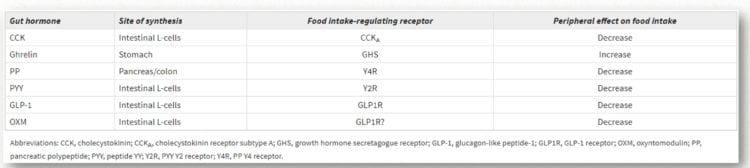
It is important to note that there is only one hormone that can increase hunger and that is ghrelin which is synthesized in the stomach.
All the other hormones, including CCK, PP, PYY, GLP-1 and OXM (Oxyntomodulin) decrease hunger. That is, all of these hormones promote satiety; the feeling of being full’. It is very important to note that four of these hormones, CCK, PYY, GLP-1 and OXM are all synthesized in the small intestine L-cells.
The above is the all the basic physiology that is needed to understand the effects of food processing on the speed and location of nutrient absorption, the nature of hunger and satiety and how the current epidemic in metabolic diseases we now face is a result of disregulation of this system.
3 a. The Effect of Cooking Foods on Body Weight
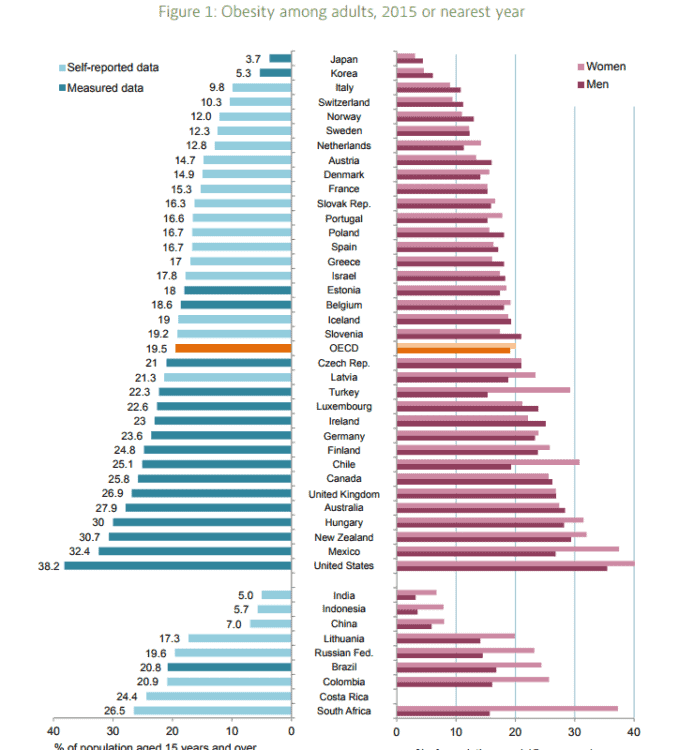
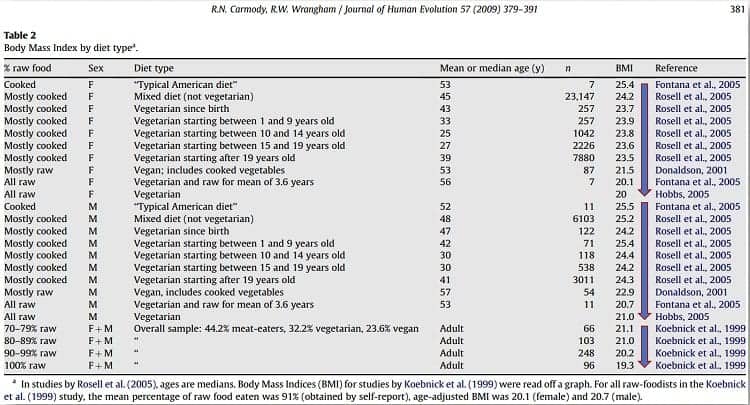
One of the most ancient forms of food processing is cooking, and there are studies which indicate that there is an association between how many raw foods people eat and their body weight. There is a generally tendency that the more raw foods a person eats, the lower their body weight. That does not mean that eating a vegetarian diet is more desirable, it is only to point out that with more and more processing — in this case, cooking, the higher body mass tends to be.
3b. The Effect of Cooking Foods on Nutrient Availability
Carbohydrate-rich Foods
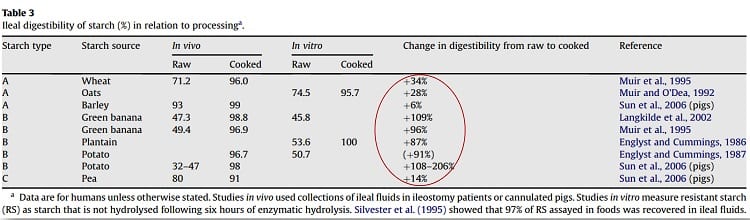
The relationship between cooking foods and body weight is particularly important with respect to carbohydrate-rich foods. For example, when grains are cooked they become much more digestible — meaning that more of the nutrients in the grain is available to be absorbed. In the case of potatoes, there is double or triple the amount of energy (calories) available to the body when they are cooked versus when they are raw. When a potato is cooked, the digestible starch increases 2-3 times, which means that these calories are now available to the body where they weren’t when they were raw.
Lipid and Protein-rich Foods
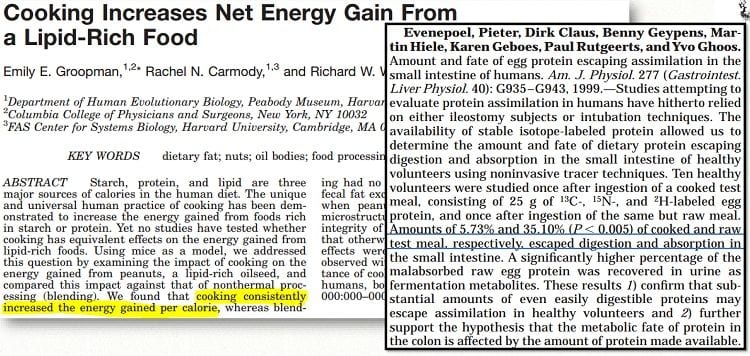
When foods that are high in lipids (fats) such as peanuts are cooked, the amount of energy the body is able to derive from the food, increases. As well, significantly more amino acids in protein-rich foods such as egg make it to the large intestine (where their nutrients are absorbed) when the protein-rich food is cooked.
3c. The Effect of Non-Thermal Food Processing on Nutrient Availability
Mechanical processing, such pounding food is also an ancient form of food processing which has an effect on how many nutrients are available to be digested. The nutrients available to the body when food is eaten raw and whole versus raw and pounded is significant, and this holds true whether the food is animal protein such as meat or a starchy vegetable such as sweet potato.
In a study with mice, one group of mice was fed meat either raw and whole or raw and pounded and then the group was crossed over to cooked and whole or cooked and pounded. The other group of mice was fed sweet potato eaten raw and whole or raw and pounded and then crossed over to cooked and whole or cooked and pounded.
When the meat or starchy vegetable (sweet potato) was eaten raw and whole, it was associated with lower body mass than the same foods eaten raw and pounded because the mice lost weight. As expected from what is known about the effect of cooking on nutrient availability (see above), when the mice ate the cooked meat or cooked sweet potatoes, they either didn’t lose as much weight (in the case of the meat) or actually gained weight (in the case of the sweet potato).
The conclusion of this study was worth noting;
”Our results indicate that human dieters who count calories and eat similar mixed diets but cook them to different extents would experience different weight gain outcomes at comparable levels of physical activity. This prediction is consistent with recent long-term data indicating that preparation-specific factors affect the relationship between caloric consumption and weight gain in humans.”
3 d. The Effect of Hydrolyzing Protein on Hormonal Response in the Small Intestine
Hydrolyzed protein, is essentially pre-digested protein and this process has an impact on which hormones are released in the small intestine when it is eaten.
In a 2010 study, comparing soy protein with soy protein hydrolysates and whey protein with whey protein hydrolysates, it was found that significantly more insulin compared to glucagon is released with the hydrolysates versus the intact protein. This means that the insulin to glucagon ratio is higher and insulin is the hormone which signals the body to store energy. A higher insulin to glucagon ratio means that the body is storing energy rather than responding to glucagon which signals the body to use glucose and fat for energy.
4 a. The Effect of Mechanical Processing on the Blood Glucose Response of a Carbohydrate Food
Grinding / Juicing Fruit
Mechanical processing of a food doesn’t change the amount of carbohydrate that is in it. That is, when we compare 60g of whole apple with 60 g of pureed apple or 60g of juiced apple, there is the same amount of carbohydrate each. When we compare the Glycemic Index of these three, the results are very similar so this isn’t very helpful to tell us about the blood glucose response to actually eating these different foods.
When these foods are eaten, the blood glucose response 90 minutes later, is significantly different.
Note: It’s not relevant to the outcome, but on this graph, slow and quick puree and juice as just differences in the amount of time it took for the liquid to be drunk.
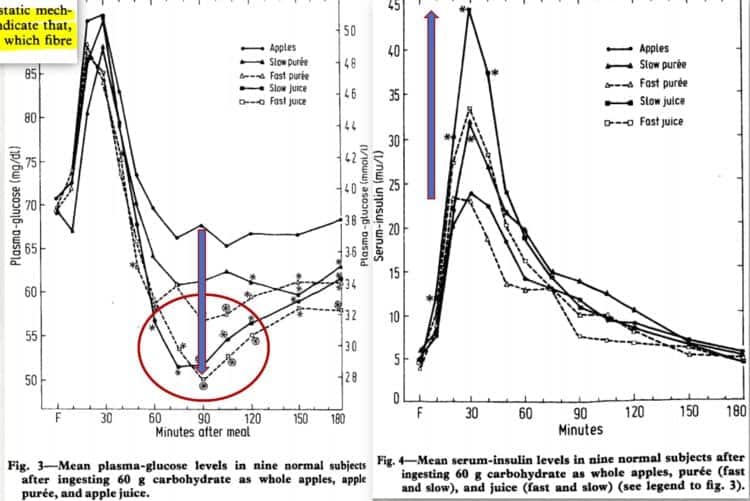
As can be seen by the graph on the right, in healthy individuals blood insulin level goes very high with the juiced apple and in response, blood glucose then goes very low, below baseline.
The response that we see with the juiced apple is typical of what is seen with ultra-processed carbohydrates.
Grinding Grains
Grinding grains is another type of ancient food processing which changes the hormonal response in the small intestine.
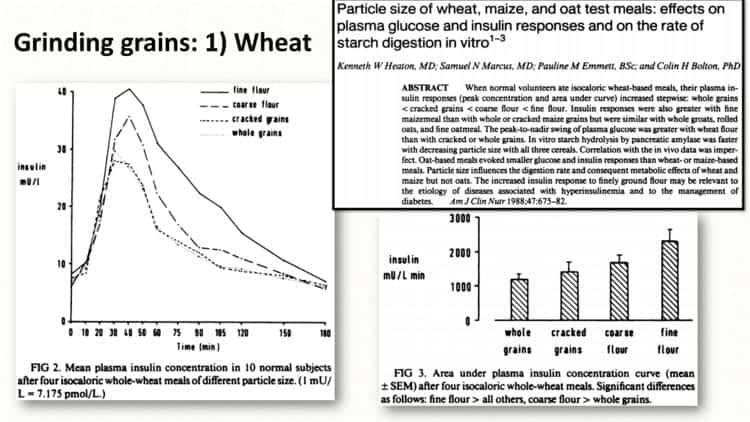
When healthy individuals eat grain-based meals, the plasma insulin response increases the smaller the particle size of the grain. That is, a specific amount of whole grain releases less insulin than the same amount of cracked grains, which is less than the same amount of course flour. The highest amount of insulin is released in response to eating the same amount of fine flour.
What was true for wheat in this study was true for rice as well and what was of interest, is there wasn’t a big difference between the insulin response with brown rice versus white rice.
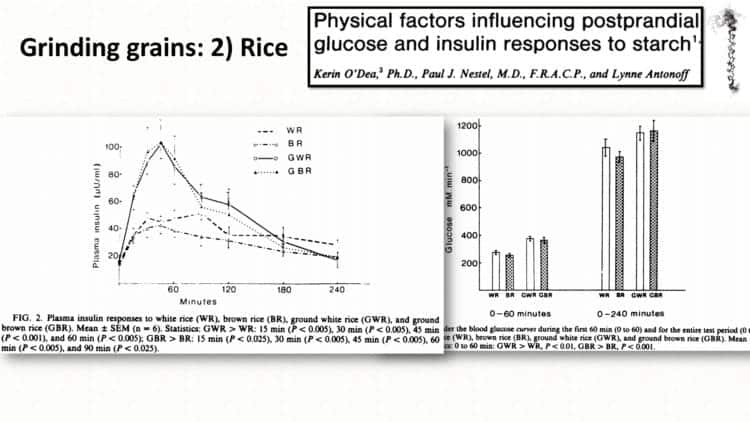
There is no difference in the Glycemic Index or Glycemic Load of whole wheat versus ground wheat or whole rice versus ground rice, but there is a huge difference in the insulin response with difference types of mechanical processing.
It’s also important to note that the amount of fiber that was in the grain did not make a difference in the amount of insulin released, only the amount of mechanical processing of the grain. So, eating brown rice versus white rice won’t change the amount of insulin that is released – and insulin is a hormone that signals the body to store energy (calories).
In this next study, the same response that we saw with the pureed and juiced apples (above) is also seen with finely ground wheat bread. We see plasma glucose rise rapidly and then it drops below baseline at 120 minutes (circled).
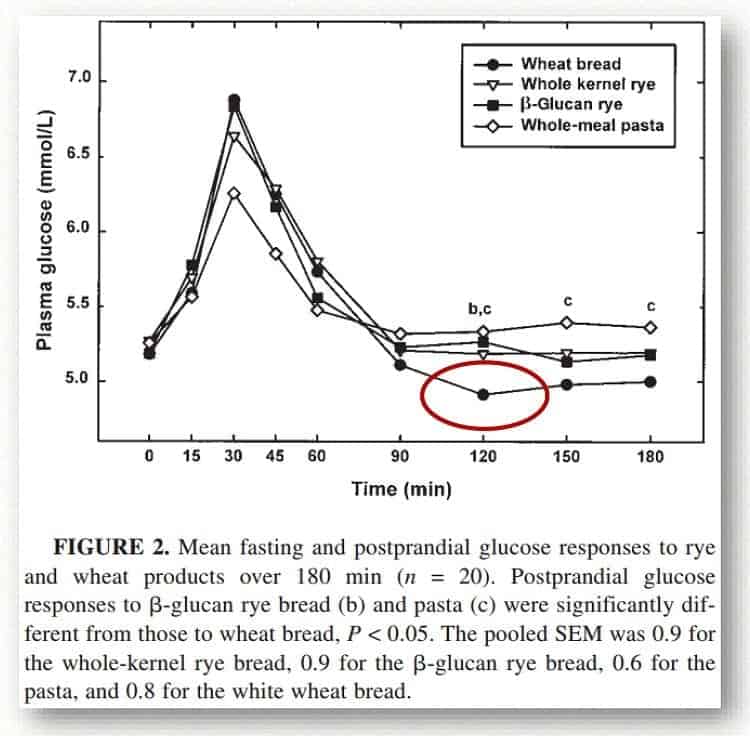
We know that the difference wasn’t due to the amount of fiber, because in this study they added back the fiber and it didn’t make a difference.
The difference had to do with the amount of disruption to the structure of the grain. So, eating whole wheat bread versus eating white bread — which is just adding the fiber that was taken out back won’t help much in terms of the insulin response.
The disruption of the structure of the grain had very adverse effects on the hormonal response; both the insulin response and GIP response, which can be seen in the next graph;
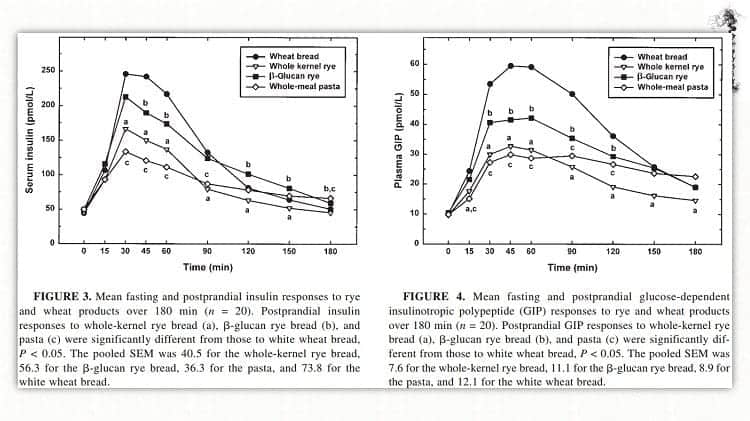
The bread made with flour resulted in a much larger insulin response and plasma GIP response than those made with whole kernel grains
Recall from the first article in this series, that GIP is released from the K-cells, which are dominant in the upper part of the small intestine. Bread made from ground flour results in a much greater and earlier hormonal response than bread made from whole grains.
The same researchers did another study a year later, this time with wheat bread, rye bread with the endosperm, traditional rye bread and high-fiber rye bread. As can be seen from these graphs (whether wheat or rye bread), it is the structural difference of the bread that explains the insulin response after a meal, not the total amount of fiber.
Note: Gabor Erdosi made a table comparing the Area Under the Curve (AUC) of the hormonal response of GIP (from the K-cells in the upper part of the small intestine) and GIP-1 (from the L-cells in the lower part of the small intestines) for the different breads which was very telling.
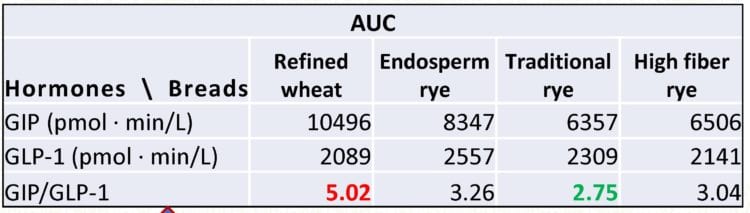
As can be seen from this table, there was almost double the GIP/GLP-1 ratio in the refined wheat bread (5.02) than the traditional rye bread (2.75) and this difference was largely due to significantly more GIP being released from the K-cells high up in the small intestine with the refined wheat bread than with the traditional rye bread.
It wasn’t due to fiber, because there was less GIP released with the traditional rye bread than even with the high fiber rye bread.
4 b. In-Vitro Hydrolysis of Starch Highly Correlates to Starch Digestion in the Small Intestine
This study shows a striking ability to predict how starch is hydrolyzed (broken down) in the small intestine with how it is broken down in a petri-dish in a lab using alpha-amylase. A perfect correlation would be = 1 and in this case it is 0.95.
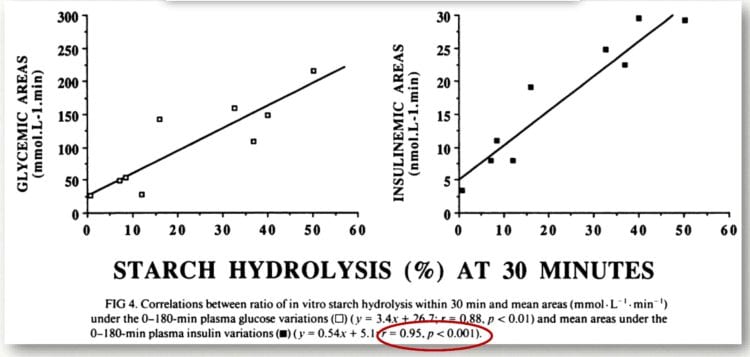
As can be seen from these graphs, the glycemic response (blood sugar response) and the insulin response in the body can be accurately predicted using this method.
In this article we considered the effect of various kinds of food processing’ on the speed and location of food absorption of individual macronutrients (such as protein, fat and carbohydrate), but we rarely eat meals that are only carbohydrate, or only protein or only fat.
How does the presence of protein and fat-rich foods influence the hormonal response in the small intestine and how do these affect the hormonal response to carbohydrate? How does fiber content or addition of fiber affect the hormonal response, or does it? These will be the topic of the next article where we’ll look at the hormonal response of the body to mixed meals (meals with different combinations of fat, protein and carbohydrate.
Perhaps you wonder what all this information means for you.
Maybe, like many you’ve become metabolically unwell with Type 2 Diabetes or high blood pressure or high cholesterol despite eating a diet rich in whole wheat bread, whole grain rice and lots of cooked vegetables and are beginning to realize that how your food is processed is as important a factor as the nutrients it contains in it’s unprocessed form.
I can help.
Feel free to send me a note using the “Contact Me” form located on the tab above to find out information about the services I offer, both in-person in my office or via Distance Consultation (using telephone or Skype).
To your good health!
Joy
You can follow me at:
![]() https://www.facebook.com/lchfRD/
https://www.facebook.com/lchfRD/
Gabor’s full lecture can be watched here:
References
- Gribble, Fiona M., and Frank Reimann. ”Enteroendocrine Cells: Chemosensors in the Intestinal Epithelium.” Annual Review of Physiology 78, no. 1 (2016): 277—99.
- Reimann, Frank, and Fiona M Gribble. ”Mechanisms Underlying Glucose-Dependent Insulinotropic Polypeptide and Glucagon-like Peptide-1 Secretion.” Journal of Diabetes Investigation 7 (2016): 13—19.
- Nauck, Michael A., and Juris J. Meier. ”Incretin Hormones: Their Role in Health and Disease.” Diabetes, Obesity and Metabolism 20 (2018): 5—21.
- Perry, B., and Y. Wang. ”Appetite Regulation and Weight Control: The Role of Gut Hormones.” Nutrition & Diabetes 2, no. 1 (January 2012): e26.
- Groopman, Emily E., Rachel N. Carmody, and Richard W. Wrangham. ”Cooking Increases Net Energy Gain from a Lipid-Rich Food.” American Journal of Physical Anthropology 156, no. 1 (2015): 11—18.
- Evenepoel, Pieter, Dirk Claus, Benny Geypens, Martin Hiele, Karen Geboes, Paul Rutgeerts, and Yvo Ghoos. ”Amount and Fate of Egg Protein Escaping Assimilation in the Small Intestine of Humans.”
- American Journal of Physiology-Gastrointestinal and Liver Physiology 277, no. 5 (November 1999): G935—43.
- Carmody, R. N., G. S. Weintraub, and R. W. Wrangham. ”Energetic Consequences of Thermal and Nonthermal Food Processing.” Proceedings of the National Academy of Sciences 108, no. 48 (2011):
19199—203. - Morifuji, Masashi, Mihoko Ishizaka, Seigo Baba, Kumiko Fukuda, Hitoshi Matsumoto, Jinichiro Koga, Minoru Kanegae, and Mitsuru Higuchi. ”Comparison of Different Sources and Degrees of Hydrolysis of
Dietary Protein: Effect on Plasma Amino Acids, Dipeptides, and Insulin Responses in Human Subjects.” Journal of Agricultural and Food Chemistry 58, no. 15 (August 11, 2010): 8788—97. - Haber, G.B., K.W. Heaton, D. Murphy, and L.F. Burroughs. ”Depletion and Disruption of Dietary Fiber” The Lancet 310, no. 8040 (1977): 679—82.
- Heaton, K.W., S.N. Marcus, P.M. Emmett, and C.H. Bolton. ”Particle Size of Wheat, Maize, and Oat Test Meals: Effects on Plasma Glucose and Insulin Responses and on the Rate of Starch Digestion in Vitro” 47,no. 4 (1988): 675—82.
- O’Dea, K., Nestel, P.J., and Antonoff, L. ”Physical Factors Influencing Postprandial Glucose and Insulin Responses to Starch” 33, no. 4 (April 1, 1980): 760—65.
- Juntunen, Katri S., Leo K. Niskanen, Kirsi H. Liukkonen, Kaisa S. Poutanen, Jens J. Holst, and Hannu M. Mykkí¤nen. ”Postprandial Glucose, Insulin, and Incretin Responses to Grain Products in Healthy Subjects.”The American Journal of Clinical Nutrition 75, no. 2 (2002): 254—262.
- Juntunen, K.S., D.E. Laaksonen, Leo K Niskanen Karin Autio Jens J Holst, Kari E Savolainen, Kirsi-Helena Liukkonen, Kaisa S Poutanen, and Mykkí¤nen, H.M. ”Structural Differences between Rye and Wheat Breadsbut Not Total Fiber Content May Explain the Lower Postprandial Insulin Response to Rye Bread” 78, no. 5(2003): 957—64.
- Bornet, F R, A M Fontvieille, S Rizkalla, P Colonna, A Blayo, C Mercier, and G Slama. ”Insulin and Glycemic Responses in Healthy Humans to Native Starches Processed in Different Ways: Correlation with in Vitro Alpha-Amylase Hydrolysis.” The American Journal of Clinical Nutrition 50, no. 2 (1989): 315—23.
Copyright ©2018 The LCHF-Dietitian (a division of BetterByDesign Nutrition Ltd.)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.









 As mentioned in the
As mentioned in the 


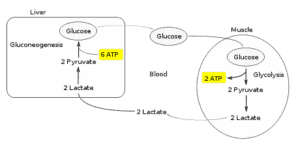 When I am doing High Intensity Training (lifting weights very slowly until muscle failure) my body first uses up all the glycogen stored in those muscles.
When I am doing High Intensity Training (lifting weights very slowly until muscle failure) my body first uses up all the glycogen stored in those muscles.




 Making it before dinner was easier than I imagined, or easier than I remembered it as a younger woman. I preheated the oven to high and began to roll out the dough between pieces of waxed paper and placed them each in large Pyrex (glass) pie plates.
Making it before dinner was easier than I imagined, or easier than I remembered it as a younger woman. I preheated the oven to high and began to roll out the dough between pieces of waxed paper and placed them each in large Pyrex (glass) pie plates.