Joy Y Kiddie MSc., RD - I'm a Registered Dietitian in private practice in British Columbia, Canada that provides low carb and ketogenic services in-person in my Coquitlam office, as well as by Distance Consultation (using Skype / telephone).
INTRO: “Before” and “after” photos are often the source of encouragement, as I progress on my journey. This “before and since” photo serves as some Monday-morning motivation.
Yesterday, after ten days on crutches and a brace due to a torn MCL tendon, I had finally progressed to a cane and just had to get out for a bit. With a break in the rain, one of my sons and I headed for Indian Arm, an ocean inset nearby. It was mild and humid and I really didn’t want to wear a long sleeve jacket, so I reached for a down-filled vest that I bought a number of years ago that never zipped or snapped up, and headed out. When we arrived, there was a breeze off the salt water and instinctively, I zipped up the vest and snapped the outer snaps. Only in hindsight did I realize this was the first time I ever did that – and with a little room to spare.
We walked (actually, I hobbled on my cane) along the coast path and down to the pier and took in the fresh air and beautiful view. As we were leaving, I remembered the photo that was taken of me 2 1/2 years ago on the same pier, around the time I first learned about eating low carb high fat (LCHF) and asked my son to snap a photo of me on my phone, so I could compare them. In both photos, I was dressed in comfortable clothes, with no makeup and my hair however it was.
When we returned home, I dug out the old photo and here they are, side by side. Even with my puffy down-filled vest and knee brace, the difference is noticeable, even though it has only been 6 months that I have been “practicing what I preach” and eating low carb, myself. Since I am very much ‘in progress’ with my weight loss and achieving my health goals, I refer to this as before and since rather than before and after.
Me – summer 2015 (left), me fall 2017 (right)
It will be interesting to take an updated photo this time next year to see the progress.
Encouragement in our health journeys come in many forms; a number on the scale, new lab results, readings on a glucometer, or photos over time.
Today I celebrate this mid-point progress in this Dietitian’s Journey and I encourage you to celebrate yours!
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
In December 2008, the American Diabetes Association (ADA) issued its Clinical Practice Recommendations which included the option for Diabetics to follow low-carbohydrate diets as a weight-loss option. While this is obviously not ‘news’, it is important to note that the Canadian Diabetes Association – now called Diabetes Canada, does not as yet make the same recommendation.
Why is that?
Is there something inherently different about Diabetics in Canada than Diabetics in the United States?
For the last 9 years the American Diabetes Association has given people the option of following what they call a “moderate” carbohydrate diet by (a) omitting some of the carb-containing foods on their standard meal plan or (b) substituting them for much lower carb alternatives. They also (c) provide Americans with the option of following a low carb diet for weight loss.
Let’s take a look at the American dietary recommendations compared with the Canadian ones.
Dietary Recommendations of the American Diabetes Association
On their web page, the American Diabetes Association states that their standard Meal Plans that are “moderate” in carbohydrates provide ~45% of calories from carbs, but they add;
Your healthcare provider may ask you to limit carbohydrate more than our meal plan suggests. This means you should cut back on the carbohydrate foods that you eat throughout the day. To keep your calorie intake about the same, substitute sources of lean protein or healthy fats for those higher carbohydrate foods.
Then they give some examples of how people can lower carbohydrate intake by making some adjustments to the posted meal plan, such as;
omitting the slice of whole wheat toast at breakfast
replacing the whole wheat wrap for a lettuce wrap at lunch
skipping the serving of brown rice at dinner and adding another non-starchy vegetable instead.
For the last 9 years (2008), Diabetics in the US have also been given the option by the American Diabetes Association to follow a low carb diet in order to lose weight. The 2008 Summary of Revisions for the Clinical Practice Recommendations was changed to include the following;
The ”Medical Nutrition Therapy” section has been revised; updates to this section include the following revised recommendations for weight loss:
For weight loss, either low-carbohydrate or low-fat calorie-restricted diets may be effective in the short-term (up to 1 year).
For patients on low-carbohydrate diets, monitor lipid profiles, renal function and protein intake (in those with nephropathy), and adjust hypoglycemic therapy as needed.
What the last sentence means is that doctors should monitor thecholesterol and triglyceride levels of their patients on low-carb diets and adjust the dosage of the medication prescribed to control blood sugar levels.
As has been the experience of physicians that prescribe a low carb high fat diet to their patients, as blood sugar levels drop – they need to reduce their patient’s medications dosages and in time, these medications are often discontinued entirely.
What are the dietary recommendations given to Diabetics in Canada?
“Choose starchy foods such as whole grain breads and cereals, rice, noodles, or potatoes at every meal. Starchy foods are broken down into glucose, which your body needs for energy.”
The sample meal plan for small appetites on the Diabetes Canada website recommends that people consume 193 g of carbohydrates per day which is approximately 13 servings* of carb-containing food per day (* based on the Diabetic exchanges, where 1 serving is 15 g of carbohydrate).
Diabetic Sample Meal Plan (for small appetites) from Diabetes Canada
The Diabetic Sample Meal Plan for larger appetites is the same as above, but also includes an afternoon snack with a medium apple or small banana (+ 25 g carbohydrates), plus a medium pear at supper (+29 g carbohydrates) and another glass of milk with the above evening snack (+12 g carbohydrates), amounting to 259 g of carbohydrates per day, which is almost 17 servings* of carb containing foods.
Diabetics in Canada are advised to eat 45 — 60 g of carbs at each of 3 meals, plus 15 — 30 grams of carbs at each of 1-2 snacks.
This is a lot of carbohydrate for someone whose body isn’t handling carbohydrates well.
The Diabetes Canada webpage, under Healthy Living Resources, there is a section titled Diet and Nutrition. Under this are the organizations recommendations concerning Carbohydrates. They encourage carbohydrate counting which “focuses on foods that contain carbohydrate as these raise your blood glucose (sugar) the most.”
They encourage Canadian Diabetics to “follow these steps to count carbohydrates and help manage your blood glucose levels”.
What are those steps?
Step 1: Make healthy food choices
Step 2: Focus on carbohydrate
Step 3: Set carbohydrate goals
Step 4: Determine carbohydrate content
Step 5: Monitor effect on blood glucose level
Diabetes Canada recommends that Diabetics eat ~ 1/2 of their calories as carbohydrate while at the same time advising people that “foods that contain carbohydrate … raise your blood glucose (sugar) the most”.
So, when Diabetics eat the large percentage of their diet as carbs and their blood sugar is raised, what should they do?
Well, the Diabetes Canada webpage goes onto explain under Step 5 that they should “monitor the effect (of carbohydrates) on blood glucose level and
Work with your healthcare team to correct blood glucose levels that are too high or too low.
I had to read this several times to make sure I wasn’t misreading it.
Diabetics in Canada are being told;
carbs raise their blood sugar the most
that they are to take in ~1/2 of their calories as carbs
when their blood sugars get too high, they need to have their medication adjusted to handle the load.
Could this be why Diabetes is said to be “a chronic, progressive disease”?
Change in the American Diabetes Association Postion
In 2007, a year before the revised recommendations came out approving either a low-carb diet or a low calorie restricted diet, the American Diabetes Association recommendations stated that ‘low carb diets were not recommended for the treatment of overweight or obesity—even in the short term, because their long-term effects were unknown and they did not seem to provide better maintenance of weight loss than low-fat diets over the long term’.
However, in a press release with the release of the 2008 recommendations the American Diabetes Association reversed its position saying;
”there is now evidence that the most important determinant of weight loss is not the composition of the diet, but whether the person can stick with it, and that some individuals are more likely to adhere to a low carbohydrate diet while others may find a low fat calorie-restricted diet easier to follow.”
Furthermore, in the same press release, the American Diabetes Association President of Health Care & Education at the time, Registered Dietitian Ann Albright, PhD, RD, said;
”We’re not endorsing either of these weight-loss plans over any other method of losing weight.”
Albright added that it was ‘more important that people with Diabetes choose a weight-loss plan that works for them and that their healthcare team supports their efforts and monitors their health accordingly‘.
Canadian Recommendations
The Canadian Clinical Practice Guidelines recommends that people with Diabetes receive nutrition counselling from a Registered Dietitian. They recommend that those who are overweight or obese reduce caloric intake to achieve and maintain a healthier body weight and state that it is consistency in carbohydrate intake and in spacing and eating regular meals that may help control blood glucose levels and weight.
People with diabetes should receive nutrition counselling by a registered dietitian.
Reduced caloric intake to achieve and maintain a healthier body weight should be a treatment goal for people with diabetes who are overweight or obese.
The macronutrient distribution is flexible within recommended ranges and will depend on individual treatment goals and preferences.
Replacing high glycemic index carbohydrates with low glycemic index carbohydrates in mixed meals has a clinically significant benefit for glycemic control in people with type 1 and type 2 diabetes.
Intensive lifestyle interventions in people with type 2 diabetes can produce improvements in weight management, fitness, glycemic control and cardiovascular risk factors.
A variety of dietary patterns and specific foods have been shown to be of benefit in people with type 2 diabetes.
Consistency in carbohydrate intake and in spacing and regularity in meal consumption may help control blood glucose and weight.
Final Thoughts…
Why are Diabetics in the US recommended to lose weight by following either a low-carb diet or a low calorie restricted diet, yet Diabetics in Canada are recommended to eat 13-17 servings of carb-containing foods per day, with 45 — 60 g of carbs at each of 3 meals, plus 15 — 30 grams of carbs at each of 1-2 snacks? That’s a good question.
Many physicians report that Diabetics following LCHF diets have their medications reduced and in many cases discontinued entirely. As a Dietitian this seems preferable as a first approach, than recommending that Diabetics eat half of their calories as carbs, which would necessitate having their medication adjusted upwards when their blood sugars get too high, and having people’s Diabetes continue to worsen in time.
Why should Canadians with Diabetes not be provided with choice?
All illustrations and text content contained on this web page are the intellectual property of The Low Carb High Fat Dietitian (a division of BetterByDesign Nutrition Ltd.).
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
American Diabetes Association, Adjusting the Meal Plan, http://www.diabetes.org/mfa-recipes/2017-07-adjusting-the-meal-plan.html
Dairman T., Diabetes Self-Management, ADA’s New Guidelines OK Low-Carb Diets for Weight Loss, 2008 Jan 7, www.diabetesselfmanagement.com/blog/adas-new-guidelines-ok-low-carb-diets-for-weight-loss/
Dworatzek PD, Arcudi K, Gougeon R, Husein N, Sievenpiper JL, Williams SL. Nutrition Therapy, Canadian Diabetes Association Clinical Practice Guidelines Expert Committee, http://guidelines.diabetes.ca/browse/chapter11
Summary of Revisions for the 2008 Clinical Practice Recommendations, Diabetes Care 2008 Jan; 31(Supplement 1): S3-S4.
This recipe is posted as a courtesy to those following a variety of low-carb and ketogenic diets (not necessarily Meal Plans designed by me). This recipe may or may not be appropriate for you.
August 4 2019 update: a smaller version of this as a Marble New York Cheesecake is available here.
Some people think of Dietitians as the healthcare professional that is going to take all the fun out of life. We’re going to advise you to eat carrots, when everyone else is eating cheesecake. That is not how I practice. Even when I taught a higher carb style of eating, I always believed there were “everyday foods” and “sometimes foods” and never believed in forbidding any food (unless serious food allergies were involved). For me it’s always been about how much and how often we eat something.
If you’ve been following my blogs for a while, you know that I don’t believe in eating unlimited amounts of any type of foods or restricting any food groups. Yes, I recommend people eat carbs in vegetables, nuts and seeds, certain dairy and some fruit and legumes, if tolerated. I encourage eating a wide range of healthy fat, including that found in the protein sources, animal proteins, and plant-based fats such as olive oil, avocado oil, and coconut oil.
But what about sweets? Where do they fit in?
I do think there are times where celebrating a special occasion warrants making something special that contains carbs, fat and protein beyond what we usually eat. I am not the Grinch of holidays or celebrations!
I encourage people to plan for eating the treats by knowing the macronutrient content in it (amount of protein, fat and carbs in grams) and subtracting that from their Meal Plan ahead of time. This rarely necessitates people eating more than they usually do because the foods themselves, if well planned, can take the place of a meal. If it means that someone eats “Pumpkin Pie without the Pie” (crust-less low carb pumpkin custard) instead of supper, so be it! The net carbs from the pumpkin itself minus the fiber aren’t that high, and the eggs and cream inside the custard filling serve as the protein source for the meal, and the rest is fat. So? What’s wrong with that?
Tonight is one of those occasions that a special treat was warranted. One of my sons has been wanting New York style cheesecake since he began eating low carb high healthy fat with me, 7 months ago and today I baked him one! It is creamy and rich with all the mouth-feel one expects from New York Cheesecake from the cream cheese, egg and egg yolks. It has real Swiss dark chocolate and homemade vanilla extract, made from real vanilla beans soaked in Russian vodka. It has a little hint of sweet, because after all, it is for a special occasion! Should he choose to (or rather if he were even able to) he could eat the entire 8 1/2″ cheese cake and not exceed his daily carbs! I can assure you, he will try! And who could blame him?
Low Carb New York Style Cheesecake
Ingredients
Five 250 g (8 oz) pkgs cream cheese, room temperature
1 1/2 cup monk fruit erythritol granulated sweetener
1/4 tsp salt
1/2 tsp real vanilla
5 lg eggs, plus two egg yolks, room temperature
200 gm (3.5 oz.) 85% cocoa Swiss dark chocolate, melted in a double boiler
Instructions
Preheat the oven to 500 F.
Prepare an 8 1/2 or 9″ spring-form pan by lining with parchment paper and spraying well with an oil spray.
In the bowl of a stand mixer using the flat paddle or by hand, beat the cream cheese until very well blended and add the eggs one at a time, continuing to blend. Add the egg yolks, then the salt, granulated erythritol, and real vanilla.
Remove the bowl from the stand mixer and fold in the melted, cooled chocolate.
Bake at 500°F for 12 minutes, then lower the heat to 200° F and make for another 45 minutes.
(UPDATE December 2020) I now bake it at 350°F for 55 minutes then turn off the oven and let it cool inside, so it doesn’t crack. I find the texture much better this way.)
Turn off the heat of the oven and open the door, but leave the cheesecake inside for 30 minutes until partially cooled.
Then move it to a draught-free location to completely cool.
Enjoy!
Based on 1/12 of the cheesecake, the macronutrient content is as follows;
Carbohydrates: 1 g
Protein: 17 g
Fat: 46 g
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
It’s been 7 months since I’ve been seriously adhering to a low carb high heathy fat (LCHF) lifestyle, but like anybody else it’s easy for me to get frustrated when I don’t reach goals as quickly as I would like. I have to stop and remind myself that I didn’t become obese and Diabetic overnight and it’s going to take time to reverse these symptoms. These updates help me take stock of my progress, because after all it’s about progress, not perfection.
Joy – class 2 obesity
At my highest weight, my Body Mass Index (BMI) put me well into the Class 2 Obesity category. I felt terrible, looked terrible and was desperately unhealthy. Losing weight seemed impossible – or if not impossible, too difficult.
September 20 2015
This is what I looked like 2 1/2 years ago, when I first heard about following a low carb high healthy fat lifestyle from a retired physician-friend. At this point, I had already lost about 25 pounds by cutting portion sizes and exercising, but my weight was always fluctuating by 10 or 12 pounds and with it, my blood sugar, cholesterol and blood pressure. I was in denial about how very unwell I had become.
The sudden death of two girlfriends my own age was certainly a ‘wake up call’, but it was my blood pressure that had become dangerously high that was the final impetus for me to change. I knew that if I did nothing, I was at very high risk of having a stroke or heart attack. My choice was (1) to go on medication for high blood sugar, high cholesterol and high blood pressure or (b) change the way I ate. It was, as they say, a “no brainer”.
March 5, 2017 was the day I made the decision to change and there has been no looking back.
Change only happens when the pain of staying the same is greater than the pain of changing.
March 16 2017 – the beginning of the journey
This is what I looked like when I started. Based on my BMI, I was well into the Class I Obesity category.
My blood pressure ranged between Stage 2 Hypertension and Stage 1 Hypertension – dangerously high.
My morning fasting blood sugar was averaging ± 12 mmol/L (216 mg/dl) and my HbA1C was likely ~ 9.5%.
My triglycerides were high and my LDL cholesterol (“bad cholesterol”) was well above what it should have been for someone who was Type 2 Diabetic and had family risk factors.
I was determined to reverse the symptoms of Diabetes, high triglycerides and high blood pressure by changing how I ate.
Progress, not perfection
Blood Glucose
When I began this journey at the beginning of March, my fasting blood glucose was averaging 12 mmol/L . My HbA1C was likely ~9.5%. Four months into eating low carb high fat, my fasting blood sugar was averaging 8.5 mmol/L and my HbA1C was 7.5% – still above the ≤ 7.0% therapeutic target for those with Type 2 Diabetes.
This week, 3 months later, my HbA1C reached the ≤7.0% therapeutic target for those with Type 2 Diabetes, but that is still not good enough. My goal is to get it at or below 6.0 % – below the Diabetic cutoff range. My challenge remains that my blood sugar is frequently high in the morning when I am fasted, yet is significantly lower in the late afternoon when I have been intermittent fasting for the same length of time. I continue to suspect that cortisol remains a factor as cortisol production naturally begins to climb around midnight and reaches and is highest level between 6 am to 8 am.
This higher blood sugar in the morning is something called “Dawn Phenomenon” which I had for a good 5 years before becoming Type 2 Diabetic. When I track my blood sugar from 10 pm until 8 am, it starts going up in the wee hours of the morning and keep rising until 6:30 or 7 am so it’s evident that my fasting blood sugar is rising with the daily fluctuations in cortisol. When I am intermittent fasting for the same amount of time during the day, my fasting blood glucose is always < 5.0 mmol/L and many times less than 4.0 mmol/L – which is usually my signal to eat something. Under the effect of cortisol combined with my liver still being insulin resistant, the glucose has no where to go and just sits in my blood.
I am going to try to get back to incorporating some form of daily activity to lower stress, which kind of fell off the radar and add some short duration, high-strength / high muscle-use exercise such as squats which can help move blood glucose into the muscle.
Blood Pressure
I continue on my low very low dose of Ramipril (Altace) and my blood pressure is averaging 127/74 mmHg. When I stop the meds for a day or two to measure my blood pressure, it is still averaging 145/82 mmHg which is still too high to discontinue the medication, but it is far better than the 160/90 mmHg that it was 3 months ago.
Weight and Body Measurements
LEFT: March 16 2017, RIGHT: October 11 2017
I’ve lost 20 lbs so far but its the change in my body and face shape that is most noticible!
In terms of “inches”, I’ve lost;
1″ off my upper arms
2.5″ off my neck (which really shows!)
1″ off my thighs
4 1/2″ off my waist (which feels amazing!)
Facial lines are more visible, but when I look in the mirror I actually recognize the face looking back.
I am now below the high end of the overweight category based on BMI and am continuing to lose weight steadily.
At the beginning of this journey, I planned to lose ~30 lbs, but I realize that to attain an ideal waist circumference that is 1/2 my height, I likely have another 30 pounds to lose now which means I am not quite half-way there, but I am making progress!
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
For the umpteenth time in as many weeks, I had a client tell me that they were told that “low carb eating is not sustainable” – and this was in the same breath as the decision to increase the second of two medications they are prescribed for Type 2 Diabetes.
What frustrates me is that their physician did not even want this person to try a lower carbohydrate approach.
The client was reminded soberly that “Diabetes is a chronic progressive disease” and that it is “expected” that over time the dosage of both of those medications will increase until they can’t be any more, and that they will eventually be insulin-dependent. I think that for many, this becomes a self-fulfilling statement and believing it to be ‘inevitable’, people are resigned that there is ‘nothing they can do’.
But is this true? Does it have to be a chronic, progressive disease?
Medical professionals across Canada, the United States, Australia and Europe have clinical experience demonstrating that the symptoms of Type 2 Diabetes can be put into remission and that most are able to the majority of their patients off many, if not all of their medications by following a low carbohydrate diet.
What about the claim that “low carb eating is not sustainable“?
Certainly, people who adopt a low carb lifestyle eat differently than they did before – but so do people who choose to be vegetarians. How often are those who choose not to eat meat for ethical or moral reasons told that “a vegetarian diet is not sustainable“? I don’t know of any.
Following a low carb lifestyle is no more or less sustainable than choosing not to eat meat.
For heaven’s sake, for the last 40 years people have been advised to eat a low-fat diet and I don’t recall anyone being told that “a low fat diet is not sustainable“.
I like to think of adopting a low carb lifestyle in terms of someone who has been diagnosed with a food allergy or food intolerance. Someone who’s been diagnosed as Celiac is intolerant to gluten and they make the choice to avoid gluten for health reasons. People with nut allergies also face food restrictions that guide their choices. Do we ever hear Celiacs being told that “eating a gluten restricted diet is not sustainable” or that “eating a nut-free diet is not sustainable“?
No.
People are advised by their doctors, or who have consulted with their doctors to follow these dietary restrictions for health reasons should not view this style of eating as any more or less restrictive or limiting than any other dietary restriction made for heath reasons.
Many people who adopt a low carb lifestyle do so to reduce the risks associated with health conditions such as Type 2 Diabetes, high blood pressure and high triglycerides / cholesterol. People who have seen friends or family members live through or die from complications from these conditions are likely to be highly motivated to make dietary changes and to stick with them. As with any other dietary restriction, a low carb lifestyle is a dietary choice and the willingness to continue with it is tied to the strength of the motivation to make that dietary change in the first place.
Note: The American Diabetes Association gives Type 2 Diabetics the option of following either a moderate low carb diet (130g carbohydrate) or a low calorie calorie restricted diet for up to a year, for weight loss. At the present time, Diabetes Canada does not yet approve this approach.
Once people start eating lower carb, how much better they feel provides the self-motivating to continue! They report that they are no longer driven by food cravings, that they sleep better, have more energy and mental clarity and focus. Many people with joint stiffness and pain find it improves considerably and of course, they lose weight naturally and almost effortlessly, without being hungry.
There is such a sharp contrast between how they feel after adopting a low carb lifestyle to how they felt before, that this serves to reinforce their initial reason for adopting this change. Why would they want to go back to feeling overstuffed, lethargic, hungry and tired? So they continue in their lower carb lifestyle.
What if when a person is faced with the preconceived conclusion that “low carb eating is not sustainable” they responded by suggesting adopting it for 3 months and re-running the blood work, alongwith the commitment to monitor their own blood glucose levels and blood pressure daily, and returning immediately if there are any issues? People could get “buy in” from their doctors in order to improve their own health using dietary changes – in much the same manner as dietary changes are used to manage other conditions. This is what I ask my clients to do before they begin a low carb diet; to discuss the approach with their doctors beforehand and have them follow them over time.
Maybe to change the ‘status quo’ is simply a matter of each of us advocating for change in managing our own “chronic, progressive diseases” – especially those that need not be either chronic, nor progressive.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
In both a recent A Dietitian’s Journey entry (Food as Medicine – dramatically lower blood sugar) and an academic article (Food as Medicine to Lower Blood Glucose – scientific support), I discussed the use of- and scientific basis for consuming beverages containing apple cider vinegar, ginger, turmeric root, and kombuchain lowering blood sugar levels. In this post, I provide the recipe for “ACV Gingeraid” along with the different variations mentioned in the above-mentioned articles.
These beverages are most effective in lowering blood glucose when drunk immediately after a meal containing carbohydrates and nightly, before bed.
NOTE: Given the possibility of these ordinary foods resulting in a dramatic drop in blood sugar, if you are taking any medication, especially for controlling high blood sugar, check with your doctor before adding any of these foods to your diet.
ACV Gingeraid – basic recipe
1 litre water, carbonated (or use Club Soda/Seltzer)
2 tsp apple cider vinegar, unpasteurized, unfiltered
1 tsp ginger root, washed, peeled, freshly grated
In a 1 litre of carbonated water (Club Soda/Seltzer), add 2 tsp of unpasteurized, unfiltered apple cider vinegar such as Braggs®. Allen’s® also makes one, but read the labels carefully, as their regular apple cider vinegar is pasteurized and hence does not contain the “mother”, or culture. Using a very fine grater, grate a 1″ x 1″ knob of washed and peeled ginger root and add it to the acidulated water. Cover tightly and chill if desired, before drinking or drink at room temperature.
Turmeric ACV Gingeraid
1 litre water, carbonated (or use Club Soda/Seltzer)
2 tsp apple cider vinegar, unpasteurized, unfiltered
1 tsp ginger root, washed, peeled, freshly grated
1/2 tsp turmeric root, peeled, freshly grated
1/8 tsp black pepper corns, freshly ground
In a 1 litre of carbonated water (Club Soda/Seltzer), add 2 tsp of unpasteurized, unfiltered apple cider vinegar such as Braggs® or Allen’s® unpasteurized. Using a very fine grater, grate a 1″ x 1″ knob of washed and peeled ginger root and add it to the acidulated water. Using a polyethylene kitchen glove or plastic sandwich bag on the hand holding the turmeric root, on the same grater, grate a 1/2″ by 1/2″ piece of turmeric root and add it to the Gingeraid. Add a few grindings of freshly ground black pepper (increases bioavailability of turmeric, due to it containing piperine). Cover tightly and chill if desired, before drinking or drink at room temperature.
Kombucha – ACV Gingeraid
1/2 litre water, carbonated (or use Club Soda/Seltzer)
1/2 liter Kombucha
2 tsp apple cider vinegar, unpasteurized, unfiltered
1 tsp ginger root, washed, peeled, freshly grated
In a 1 litre bottle suitable for carbonated drinks, add the carbonated water (Club Soda/Seltzer) and Kombucha (any flavour). Be sure to choose brands with as few carbohydrates as possible, or brew your own using a low sugar recipe.
To this mixture, add 2 tsp of unpasteurized, unfiltered apple cider vinegar such as Braggs® or Allen’s® unpasteurized.
Using a very fine grater, grate a 1″ x 1″ knob of washed and peeled ginger root and add it to the acidulated water.
Cover tightly and chill if desired, before drinking or drink at room temperature.
By changing the fruit that the second fermentation of Kombucha is made with, the flavour changes substantially. The fructose in the fruit is largely consumed by the acetic acid bacteria during the second fermentation.
Turmeric Kombucha – ACV Gingeraid
1/2 litre water, carbonated (or use Club Soda/Seltzer)
1/2 liter Kombucha
2 tsp apple cider vinegar, unpasteurized, unfiltered
1 tsp ginger root, washed, peeled, freshly grated
1/2 tsp turmeric root, peeled, freshly grated
1/8 tsp black pepper corns, freshly ground
In a 1 litre bottle suitable for carbonated drinks, add the carbonated water (Club Soda/Seltzer) and Kombucha (any flavour). Be sure to choose brands with as few carbohydrates as possible, or brew your own using a low sugar recipe.
To this mixture, add 2 tsp of unpasteurized, unfiltered apple cider vinegar such as Braggs® or Allen’s® unpasteurized.
Using a very fine grater, grate a 1″ x 1″ knob of washed and peeled ginger root and add it to the acidulated water. Using a polyethylene kitchen glove or plastic sandwich bag on the hand holding the turmeric root, on the same grater, grate a 1/2″ by 1/2″ piece of turmeric root and add it to the Gingeraid. Add a few grindings of freshly ground black pepper (for the piperine, see above)
Cover tightly and chill if desired, before drinking or drink at room temperature.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
In two recent A Dietitian’s Journey posts, I wrote about the positive impact certain foods, such as apple cider vinegar, ginger and turmeric root have had on my blood sugar levels and more recently, about kombucha and kimchi. In this article I touch on the science to support the use of these foods to lower blood glucose levels.
Apple Cider Vinegar
Apple cider vinegar has long been popular as a folk remedy for high blood sugar and a 1988 study demonstrated that vinegar lowered both blood glucose levels and insulin following the eating of complex carbohydrates (starch) and simple carbohydrates (sucrose). It is now known that vinegar acts by a similar mechanism as the Diabetes medication Metformin® and increases fat burning, increases glucose movement into cells and increases insulin sensitivity. This may account for the effectiveness of vinegar in lowering blood glucose that has been know historically and has now been demonstrated in human clinical trials.
2004 study
A 2004 study, looked at the effectiveness of apple cider vinegar in reducing blood glucose levels after a meal (postprandial) as well as insulin levels in subjects with varying degrees of insulin resistance. The small study included both non-Diabetic subjects and those with Type 2 Diabetes. The non-Diabetic subjects were either insulin sensitive (n=8) or insulin resistant (n = 11) and there were 10 subjects with Type 2 Diabetes.
Fasting subjects were randomly assigned to either drink (1) 20 g apple cider vinegar with 40 g water and 1 tsp saccharine to sweeten it or (2) a placebo (water) drink. After a week of testing, subjects switched groups, so if they previously drank the placebo, they now took the apple cider vinegar.
After a 2-minute delay, subjects ate a white bagel, butter and orange juice (87 g total carbohydrates) and blood samples measuring blood glucose and insulin levels were taken 30 minutes and 60 minutes after eating the test meal.
As would be anticipated, fasting blood glucose was higher in ∼55% of subjects with Type 2 Diabetes compared with the non-Diabetic insulin sensitive and non-Diabeticinsulin resistant groups and fasting insulin was 95—115% higher in both the subjects with Type 2 Diabetes and the non-Diabeticinsulin resistant group
Compared with the placebo, the insulin resistant subjects that drank the apple cider vinegar had 34% higher whole-body insulin sensitivity 60 minutes after the high carbohydrate test meal and the subjects with Type 2 Diabetes had 19% higher whole-body insulin sensitivity.
This study demonstrated that apple cider vinegar taken before a meal containing carbohydrate can significantly improve insulin sensitivity in insulin-resistant subjects – both those with Type 2 Diabetes and those with ‘pre-Diabetes’ (i.e. insulin resistant, non-Diabetic).
2015 study
A 2015 study looked at the effect of vinegar on glucose metabolism in muscle, as it is considered the most important tissue for insulin-stimulated glucose disposal.
Subjects with Type 2 Diabetes drank either (1) 30″‰mL vinegar (6% acetic acid) and 20″‰mL water or (2) a placebo drink (water) before a mixed meal of bread, cheese, turkey ham, orange juice, butter and a cereal bar (with a total of 75″‰g carbohydrates, 26″‰g protein and 17″‰g fat).
Blood glucose, and insulin levels were measured in the subject’s forearm at 30 minutes and 60 minutes before the meal and 300″‰min after the meal was eaten and compared to placebo, vinegar increased forearm glucose uptake and decreased plasma glucose and decreased plasma insulin.
Researchers concluded that vinegar’s effect on carbohydrate metabolism may be partly accounted for by an increase in glucose uptake, demonstrating an improvement in insulin action in skeletal muscle.
NOTE: The amount of apple cider vinegar taken before meals in these two studies were 1.5 Tbsp. (20 mL) or 2 Tbsp. (30 mL).
Mechanism of Action
When taken with or just before meals, it is believed that vinegar slows gastric emptying, delays the uptake of glucose and slows the rise in blood sugar following a meal (2 hours postprandial).
Vinegar also stimulates an enzyme called AMP-activated protein kinase (AMPK) that increases fat oxidation, improves glucose uptake and insulin sensitivity and lowers glucose production (gluconeogenesis) in the liver. This is similar to how the diabetic medication Metformin works (see Zhou et al, 2001).
NOTE: This article is not proposing that foods such as vinegar are substitutes for medication prescribed by a doctor.
Activation of AMPK by vinegar has been demonstrated in the liver of vinegar fed rats and in human endothelial cells in vitro (see Kondo et al 2009, Sakakibara et al 2006, 2010, Li et al 2013) and this may account for the effectiveness of vinegar in lowering blood glucose that has been demonstrated in the human clinical trials, above.
Taking vinegar at meals has also been reported to significantly lower the glucose response after a meal (postprandial) – presumably by slowing the absorption of starch or polysaccharides (see Johnson 2009, 2010, Ostman et al 2005).
Ginger
Ginger was shown to have blood glucose lowering activity in a 2004 study that found that pre-meal treatment with ginger lowered induced high blood glucose levels (hyperglycemia).
A 2015 study evaluated the effects of a ginger powder supplement on fasting blood glucose levels and hemoglobin A1c (HbA1c) in Type 2 Diabetics. To be included, subjects needed to have been diagnosed as T2D for at least 2 years, have a HbA1c level of 6-8%, as well as taking no antioxidant supplements for at least 3 months prior to the study, and no smoking and drinking. Subjects that took insulin before or during the study were excluded, as were those that had a change in the type or dose of medication, changes in diet or any illnesses during the study.
The fifty subjects of both genders were divided randomly into and experimental and control group, with 25 subjects in each and received either a ginger-containing capsule or a placebo capsule twice a day for 12 weeks. All subjects took their usual medications for T2D and were stable on their dose.
Of 50 patients that began the study, 41 subjects completed the study (22 in the ginger group and 19 in the control group).
Fasting blood glucose levels after the intervention study were 19.4% lower in the ginger supplemented group than in the placebo group and HbA1C was .77% lower in the ginger supplemented group than in the placebo group. It was concluded that a study with more subjects and a longer study period were needed for a better observation of the effects of ginger in improving blood glucose in those with Type 2 Diabetes.
Turmeric Root
Turmeric root (Curcuma longa) is a rhizome of the ginger family that gives curry powder (which is a mixture of several spices) its characteristic yellow colour. Turmeric has been used in both Ayurvedic and traditional Chinese medicine to lower blood sugar levels. The active component of turmeric, is curcumin.
An extensive literature review of studies on curcumin was conducted and published in 2013 with more than 200 publications retrieved using the search term ”curcumin and diabetes” from the MEDLINE database, with the earliest being a case study from 1972 and curcumin has since been extensively studied in animal models of Diabetes and in a few clinical trials with subjects with Type 2 Diabetes. The conclusion of the literature review was that there is ample evidence in the scientific literature regarding the use of curcumin as a potential treatment for Diabetes as well as its associated complications.
Note: when using turmeric, be sure to add a few grinds of black pepper as it increases the bioavailability of the curcumin by ~2000 times.
Fermented Foods – Kombucha, Kimchi and Jun
Kimchi
Fermented foods, such as kombucha and kimchi are popular as probiotics for enhancing the microbiota of our intestine. Research in the field has focused on what role this complex bacterial community plays in health and disease in people, and how we can alter the microbiota through the foods and beverages we consume. The benefit of eating foods and drinking beverages with these probiotics has been demonstrated in studies and include improvement of constipation, diarrhea, irritable bowel syndrome (IBS), intestinal inflammatory conditions such as Crohn’s and colitis, as well as an improvement in immune function.
homemade kimchi
Lactic acid bacteria are the most widely used strains used to ferment foods; from sauerkraut, kosher dill pickles to kimchi, a staple of the Korean diet. For lactic acid bacteria to benefit the microbiota of the human intestines however, they first must be able to survive the hostile environment of digestion, which include extreme acidity, and digestive enzymes, and bile acids – not to mention low oxygen availability, and regulated temperature. It has been demonstrated in studies that they do.
2014 meta-analysis
A meta-analysis published in 2014 examined the effect of probiotics on glucose metabolism in patients with Type 2 Diabetes Mellitus of randomised-controlled studies where fasting blood glucose, glycosylated hemoglobin (HbA1c), insulin concentration or homeostasis model assessment of insulin resistance (HOMA-IR) changes were reported for the intervention and control groups.
Seven trials met the search criteria and results indicated that probiotic consumption significantly changed fasting plasma glucose by -0.9 mmol/L (-15.92 mg/dL). The duration of intervention for ≥8 weeks resulted in a significant reduction in fasting blood glucose of 1.2 mmol/dL (-20.34 mg/dl). HbA1C was significantly reduced by -0.54% compared with control groups. The results also showed that probiotic therapy significantly decreased homeostasis model assessment of insulin resistance (HOMA-IR) by -1.08 and insulin concentration by -1.35 mIU/L.
This meta-analysis suggests that eating or drinking foods containing probiotics may improve glucose metabolism with a potentially greater effect when the duration of intervention is ≥8 weeks, or multiple species of probiotics are consumed.
2016 meta-analysis
A meta-analysis published in 2016 examined the effect of probiotics on glucose and glycemic factors in Type 2 Diabetes of randomised-controlled studies published in English between January 2000 to June 2015. The main outcomes of interest were mean changes in glucose, HbA1c, insulin and homoeostasis model assessment-estimated insulin resistance (HOMA-IR).
A total of 11 studies with 614 subjects were included. It was found that there was a statistically significant difference between the probiotic consuming groups and the placebo-controlled groups on the reduction of blood glucose of -0.52 mmol/L (10 mg/dl).
Analysis identified that probiotics significantly reduced fasting blood glucose, HbA1c, insulin and HOMA-IR in participants with Type 2 Dabetes.
Kombucha and Jun
Raspberry kombucha
Kombucha is a beverage made by fermenting black tea and sugar with some “starter” from a previous batch, called the ‘mother’ or ‘SCOBY’ (symbiotic culture of bacteria and yeast). This is sometimes referred to as the ‘tea mushroom’ or ‘tea fungus’.
After ~ a week or 10 days, a second fermentation takes place with approximately 1 part fruit to about 10 parts fermented tea. This remains in sealed containers where it yields a lightly carbonated, mildly acidic and fruity flavoured beverage, which is the final product. In the photo to the left, this is my first batch.
Left: Kombucha (first fermentation) Right: Jun (first fermentation)
Green tea and honey can also be used to make a fermented product using a very similar process, but using a different kind of SCOBY (one that is adapted to metabolize these substrates) and the resulting product is called Jun.
The taste of jun is considerably different than kombucha, as is the alcohol content. Kombucha is typically ~1.50% alcohol whereas Jun ranges from 3-7% alcohol.
With some investigation, I was able to determine that kombucha is essentially a symbiotic growth of acetic acid bacteria and osmophilic (water-loving) yeasts in a cellulose mat that the culture makes.
The main bacteria are (1) Acetobacter –acetic acid bacteria that are able to convert the ethanol (alcohol) that is initially produced in the fermentation process to acetic acid, in the presence of oxygen and (2) Gluconobacter – acetic acid bacteria that prefer sugar-rich environments.
This is the same species that converts the ethanol (alcohol) in apple cider, to apple cider vinegar. Hence, it seems reasonable to surmise that it is the acetic acid content of kombucha and jun, which give it its characteristic tart taste, that also provide the same glucose lowering effect as apple cider vinegar.
Some final thoughts…
Given that there is scientific evidence that apple cider vinegar, ginger root, turmeric root, kimchi, kombucha & jun play a role in lowering blood glucose and other markers, these foods should be considered – along with a low carbohydrate diet and intermittent fasting (extending the time between meals) when addressing the problem of high blood glucose levels resulting from insulin resistance.
Food, and the temporary absence of it, as medicine.
NOTE: These foods should not be consumed without first consulting with your doctor, especially if you are on medication for Type 2 Diabetes as they can have a potent blood effect on blood sugar levels.
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
Akhani SP, Vishwakarma SL, Goyal RK. Anti-diabetic activity of Zingiber officinale in Streptozotocin-induced type I diabetic rats. J. Pharm. Pharmacol. 2004;6:101—105.
Ebihara K, Nakajima A: Effect of acetic acid and vinegar on blood glucose and insulin responses to orally administered sucrose and starch. Agric Biol Chem 52:1311—1312, 1988
Jayabalan R, MalbaÅ¡a R, LonÄar ES, et al: A Review on Kombucha Tea—Microbiology, Composition, Fermentation, Beneficial Effects, Toxicity, and Tea Fungus. Comprehensive Reviews in Food Science and Food Safety 13(4): 1541-4337
Johnston CS, Kim C, Buller AJ, Vinegar Improves Insulin Sensitivity to a High-Carbohydrate Meal in Subjects With Insulin Resistance or Type 2 Diabetes, Diabetes Care 2004 Jan; 27(1): 281-282.
Johnston CS, White AM, Kent SM. Preliminary evidence that regular vinegar ingestion favorably influences hemoglobin A1c values in individuals with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2009 May; 84(2):e15-7
Johnston CS, Steplewska I, Long CA, Harris LN, Ryals RH. Examination of the antiglycemic properties of vinegar in healthy adults. Ann Nutr Metab. 2010; 56(1):74-9.
Khandouzi N, Shidfar F, Rajab A, Rahideh T, Hosseini P, Mir Taheri M. The Effects of Ginger on Fasting Blood Sugar, Hemoglobin A1c, Apolipoprotein B, Apolipoprotein A-I and Malondialdehyde in Type 2 Diabetic Patients. Iranian Journal of Pharmaceutical Research”¯: IJPR. 2015;14(1):131-140.
Kondo T, Kishi M, Fushimi T, Kaga T (2009b) Acetic acid upregulates the expression of genes for fatty acid oxidation enzymes in liver to suppress body fat accumulation. J Agric Food Chem 57(13):5982—5986
Kim NH, et al. (2008). Lipid profile lowering effect of Soypro fermented with lactic acid bacteria isolated from kimchi in high-fat diet-induced obese rats. BioFactors 33(1):49-60. PMID 19276536
Li X, Chen H, Guan Y, Li X, Lei L, Liu J, Yin L, Liu G, Wang Z. Acetic acid activates the AMP-activated protein kinase signaling pathway to regulate lipid metabolism in bovine hepatocytes.
PLoS One. 2013; 8(7):e67880.
Mitrou P, Petsiou E, Papakonstantinou E, et al. Vinegar Consumption Increases Insulin-Stimulated Glucose Uptake by the Forearm Muscle in Humans with Type 2 Diabetes. Journal of Diabetes Research. 2015;2015:175204. doi:10.1155/2015/175204.
Ostman E, Granfeldt Y, Persson L, Bjí¶rck I. Vinegar supplementation lowers glucose and insulin responses and increases satiety after a bread meal in healthy subjects. Eur J Clin Nutr. 2005 Sep; 59(9):983-8.
Sakakibara S, Yamauchi T, Oshima Y, Tsukamoto Y, Kadowaki T, Acetic acid activates hepatic AMPK and reduces hyperglycemia in diabetic KK-A(y) mice. Biochem Biophys Res Commun. 2006 Jun 2; 344(2):597-604.
Shang Q, Wu Y, Fei X, Effect of probiotics on glucose metabolism in patients with Type 2 Diabetes Mellitus: A meta-analysis of randomized
controlled trials. Medicina 52 (2016) 28-34. doi:10.1016/j.medici.2015.11.008
Sun J, Buys NJ, Glucose- and glycaemic factor-lowering effects of probiotics on diabetes: a meta-analysis of randomised placebo-controlled trials. British Journal of Nutrition, 2016; 115(7):1167-1177
Yusoff et al, Aqueous Extract of Nypa fruticans Wurmb. Vinegar Alleviates Postprandial Hyperglycemia in Normoglycemic Rats, Nutrients 2015, 7(8), 7012-7026
Zhang D, Fu M, Gao S-H, Liu J-L. Curcumin and Diabetes: A Systematic Review. Evidence-based Complementary and Alternative Medicine”¯: eCAM. 2013;2013:636053. doi:10.1155/2013/636053.
Zhou et al, Role of AMP-activated Protein Kinase in Mechanism of Metformin action. Journal of Clinical Investigation 2001 Oct 15; 108(8): 1167—1174
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
I once believed that Type 2 Diabetes was a chronic, progressive disease because that’s what I was told, but I am seeing for myself that a reversal of symptoms is possible.
Today, after more than 10 years as someone with Type 2 Diabetes, I had an almost normal Fasting Blood Glucose reading of 5.8 mmol/L (105 mg/dl) – when just 6 months ago, my average fasting blood glucose was between 10 – 11 mmol/L (180 – 198 mg/ml).
Fasting Blood Glucose – September 27 2017
Just 2 months ago, after eating a low carb high fat diet with no more than 50 g of carbs per day, my Fasting Blood Sugar was averaging 7.5-7.8 mmol/L (135-141 mg/dl) and at the lab on July 25, 2017, my blood sugar was still way too high, at 8.0 mmol/L (144 mg/dl) – see below.
Fasting Blood Glucose, July 25, 2017
It was at that time that I decided to lower the amount of carbs I ate and to delay the time between meals (something referred to as intermittent fasting) as these are well-documented to help lower insulin resistance, and in turn, blood glucose. It isn’t “fasting” in the classic sense and there are many things that can be consumed during this period, that don’t affect blood glucose levels or cause a release of insulin. For me, I ate a full supper every weekday and then didn’t eat until supper the next day, although I would have any one of a number of things that don’t impact insulin or blood sugar in between, if I wanted to.
Was I hungry?
Oddly, no!
I’d have a coffee in the morning (my usual cappuccino made with diluted cream, as opposed to milk as it has no carbs) and since there aren’t any carbs in it, it’s something I can enjoy when I am “fasting”…just like “bone broth”.
A month later, on August 22nd, for the first time, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl).
This was definite progress!
To put that in context for someone without Diabetes, blood glucose taken two hours after meals should be less than 7.8 mmol/L (140 mg/dl) – so my blood sugar after supper was not only in the non-Diabetic range, it was much better than that!
The problem was, my fasting blood glucose still remained high.
I carried on with delaying the time between meals (“intermittent fasting”) during the weekdays and ate what the number of meals I wanted on weekends, keeping my carbs at a low level, and monitoring my blood glucose every two hours or so. This is the level I discovered that I do best at.
As mentioned in a previous blog, I added a no-carb beverage before bed that Imade with club soda (seltzer), apple cider vinegar and grated ginger root (and sometimes added grated turmeric root) and started seeing my fasting blood sugars come down. I dubbed it “Gingeraid”.
The last three weeks I have been playing around with drinking Kombucha during the day (which is a fermented tea beverage that is mildly acidic) and as I found out, the acid in Kombucha is acetic acid – just like apple cider vinegar.
I was noticing a marked improvement in my fasting blood sugars!
I’ve since done some poking around in the scientific literature and have discovered that Kombucha and other fermented foods such as sauerkraut or kimchi (cabbage fermented with ginger, green onion and chili – a Korean staple ) have been documented to have a marked effect on fasting blood glucose.
BINGO!
Most mornings the last few weeks, I’ve had a fasting blood glucose is ~6.2-6.5 mmol/L (112-117 mg/dl)
Today was a first, almost normal fasting blood glucose of 5.8 mmol/L (105 mg/dl).
I did a “happy dance”!
I will write and article documenting some of the scientific evidence that fermented products such as Kombucha, kimchi and apple cider vinegar lower blood sugar but suffice to say, in the meantime I will keep eating the same lower level of carbs and monitoring my blood sugar, continuing to delay the time between meals a few days per week (supper to supper, but eating food if hungry or if my blood sugar is low), drinking Kombucha during the day (I love it diluted 50-50 with Gingeraid), and will drink 1/2 to one litre of Gingeraid before bed.
I once believed that Type 2 Diabetes was a chronic, progressive disease because that’s what I was told by my endocrinologist and by the nurses I saw at the Diabetes Clinic, but I am seeing for myself what many clinicians and researchers have discovered – that achieving remission is possible!
Am I “cured”?
No.
But if I end up without any of the symptoms of the disease, does it matter?
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Like most young adults, my three sons hate when photos are taken of them, however when we gather for a holiday each year in the spring and fall, they indulge me in a group photo. This has provided me with visual documentation of my progress these past two and a half years, since I first learned about a Low Carb High Fat (LCHF) style of eating. These cell phone pictures certainly aren’t the best quality photos, but they serve the purpose.
The first photo from the left with me in the plum shirt, was taken April 2015, around the time a retired-physician friend first told me about the work of Dr. Jason Fung, a nephrologist in Toronto that teaches his patients a LCHF-diet, along with intermittent fasting (IF) to reverse the symptoms of Diabetes and obesity.
The second where I am wearing a scarf was taken in September 2015, shortly after I began eating a liberal lower carb diet, but was not following a ketogenic lifestyle or intermittent fasting. I was not eating as large amounts of carbohydrate as I had been, and guess I was probably eating ~ 130 g carbs per day.
Two and a half years of change – from April 2015 – Sept 2017
The third photo, the one in the middle, was taken exactly a year ago in September 2016. I had lost some weight, but as you can see, the crocheted cardigan I was wearing was stretched skin-tight over a striped camisole.
Quite by accident, in the fourth photo taken in April 2017, it turned out that I wore the exact same outfit as I did in the previous September. This photo was taken only a month after I had begun following a LCHF lifestyle seriously at the beginning of March (6 months ago). I wore the crocheted cardigan open, and one can see that while I lost a lot of weight on my face and neck, my abdominal circumference had decreased to a lesser degree.
Two days ago, I deliberately wore the same cardigan and skirt that I had randomly ended up wearing in the previous two photos – with the identical camisole in a different colour, underneath. What can be seen in this last photo (September 2017) is that my face and neck have continued to slim, but what can’t be seen is the huge amount of space under the crocheted cardigan. So here is a photo of that space:
The significant abdominal weight loss (~4.5″) in one year
Through the large spaces in crochet pattern of the cardigan, one can see the outline of the bottom of my skirt and my pink sandals. There is 4″ of space all around! The significant changes in weight, abdominal fat, and overall much lower blood sugar at all times of the day has occurred since I first lowered my daily carb intake from ~50 g per day in March to ~35 g per day in July – and began seriously intermittent fasting a few days per week, from supper to supper (except for coffee in the morning).
While I still have another ~25 pounds to go to reach what I believe will put me at a waist circumference of 1/2 my height, I am definitely “getting there”. The progress is slow, yes, but consistent. My lab tests and daily glucose readings reflect the change. These photos serve as more evidence.
This weekend, for the first time, I forgot to take my “baby dose” of Ramipril one night and decided to measure my blood pressure at several points the next day, to see whether it was coming down compared to 3 months ago when I began temporarily taking it, by choice. My systolic blood pressure without medication was 15 mmHg lower than it was three months ago and my diastolic blood pressure is ~5 mmHg lower. I’m going to continue taking this medication until my blood pressure is ideal without it, but it is encouraging that I am much closer to that goal.
I am sharing these photos to encourage others that for me, following a low carb high fat lifestyle has made a huge difference – and the more seriously I limited the amount of carbs I ate, the more significant my changes have been. Had eating 50 g of carbs per day produced the results I sought with respect to my insulin resistance and weight loss, I would have stayed at that level, but it became evident that I don’t process carbs at all well. For me, it was necessary to lower the amount of carbs I ate, but it is certainly worth it. There are days, such as holidays that I choose to eat more than 35 g of carbs per day but I choose to avoid going higher than 50 g per day.
I consider my intolerance to carbohydrates to be no different than if I was wheat intolerant or lactose intolerant. Some people who are lactose intolerant, for example can consume some lactose and their bodies can digest it. Others lack the ability to digest significantly smaller amounts of lactose and necessarily limit it in order to feel well. The inability of my body to process carbohydrates is no different.
Everyone is different in terms of the amount and even the types of carbohydrates their bodies can process without impacting their insulin levels, blood pressure, lipids or weight, which is why there is no one-size-fits-all “low carb diet”. What is ideal for someone else will be different than what’s ideal for me. My role as a Dietitian is to work with clients and their physicians to help determine what level of carbohydrate intake works best for them – in order to lower insulin resistance (and in turn blood glucose), lower high triglycerides and cholesterol, as well as blood pressure. Weight loss is a natural byproduct of addressing these.
Want to know how I can help you?
Please send me a note using the “Contact Us” form on this web page.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
I often get asked what I recommend people do when it is a special occasion, or a holiday. Are we allowed a “cheat day”. This is how I answer the question.
It may seem like a strange thing for a Dietitian to say, but when it comes to weight loss, or targeting lower blood sugars, or pressure or cholesterol, I don’t believe in “diets”. The way I look at it is, if people go on a diet, then at some point, they go off of it. I prefer to think of what we eat in terms of “everyday foods” and “sometimes foods”.
Eating a low carb high fat (LCHF) diet is a choice, just like becoming a vegetarian. People become vegetarian for different reasons; sometimes it is for religion reasons or ethical reasons and sometimes it is for the perceived health benefits. It’s the same with the reason people start eating LCHF. For some, it is to lower insulin resistance, for others it’s to address high blood sugar or to lose weight. Some decide to eat this way because it was the diet of our ancient ancestors. Since the reasons people start eating LCHF are different, the reasons people might give to eat a high carbohydrate food also differ.
As far as an idea of a “cheat day”, I don’t find the idea of being “allowed” or “not allowed” foods, helpful. It implies that there are rules that we are somehow ‘breaking’ – and this comes with baggage all its own. Restricting calories or restricting food and weighing and measuring every bite that we put in our mouths is not a paradigm that has served most people well – and this type of obsession and attention to “how much” can, in theory, feed a predisposition to disordered eating.
I encourage people to learn to follow a LCHF style of eating and to become adapted to burning fat, rather than just carbohydrate. Then I advise them to eat when they are hungry and stop eating when they are no longer hungry. It sounds simple, but there is some physiology behind it. Without constantly high insulin levels driving food craving, eating a diet rich in healthy fats enables people to stop eating when they are no longer hungry.
Eating or not eating high carbohydrate foods comes with an opportunity cost. The questions I encourage people to ask themselves is “what will the results or conssequences be if I eat the specific food(s) I have in mind, and in what quantities?”
“What will the consequences be if I eat 2 oz of this saffron-raisin egg bread? Or 4 oz? Or more?
For example, if a person that normally eats ~100g of carbohydrate a day wants to eat a few slices of pizza, the physiological consequences will be different than a woman that normally eats 35g of carbohydrate, or a man that normally eats 50g of carbs per day. If either of them is insulin resistant or Diabetic, it will certainly impact their blood sugars (the symptom), but how long will it have an effect on their insulin levels? That is the more important question.
“What will my blood sugars be tomorrow, if I eat 1/2 cup of this noodle pudding with dried fruit?”
For people who are in ketosis, eating foods very high in carbohydrates will cause that to cease for a time, and it might take several days of eating LCHF again until they are again in fat-burning mode. Likely there will be a few days of being hungry through the day. Are they okay with this?
I want people to have a healthy relationship with food – and that means that they can eat anything – but how much and how often?
The last time I made this bread for company, I gave them the remaining loaves to take home. I ate a small amount and really enjoyed it.
Everyday (i.e. “everyday foods”), I choose to eat LCHF, but sometimes (i.e. “sometimes foods”) I will take a taste of something yummy – and I encourage my clients to feel free to do so too. A bite of an ice cream or cake, in the grand scheme of things, won’t make a huge difference, in fact, I calculate the number of carbs that are in the food I am considering, and decide beforehand, if it is worth it for me.
Tonight I will be having my family over for a special dinner and I have decided in advance that I will have 2 oz of the bread, a spoonful of the noodle pudding and a 2″ x 1″ piece of the honey cake. Sure I can have more, if I wanted, but I’ve come to realize that whether I eat 2 oz of the saffron honey egg bread or 10 oz of it, it will taste exactly the same! Why eat more? I’ve never been a big fan of the noodle dish, so a small taste is fine with me, and the honey cake is only made once a year on this occasion, and it’s my mother’s recipe from 1954, so yes I am going to eat a bigger piece and enjoy every bite. So what am I going to eat?
Roasted chicken with saffron, honey and hazelnuts
Chicken! …and some red butter lettuce salad with raspberries on top and drowned in olive oil. Oh! And an apple slice, dipped in honey, for a sweet year.
Eating LCHF is a choice, and a lifestyle and as such, we can choose to eat other things. How much, how often and which things is up to us. If our goal is to lower our insulin levels, we will know (or need to learn) how much of something won’t have a large, lasting impact.
Note: I am a “sample-set of 1” – meaning that how I implement a low carb diet may differ from others who follow a similar lifestyle. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Several years ago, I began to ask myself how it is that 2/3 of men and ~1/2 of women in Canada are either overweight or obese. In the early 1970s, only ~8% of men and ~12% of women were obese and now almost 22% of men and 19% of women are obese- even though statistics show we are eating much less fat, drinking way less pop and eating more fish than ever before. I wondered if the increase in overweight and obesity might be related to the changes in the Dietary Recommendations that began in 1977 and which encourage us to eat 45-65% of daily calories as carbohydrate and to limit all kinds of fat to 20-35%.
In early 2015, after scouring the scientific literature and reading about the clinical use of a Low Carb High Fat (LCHF) diet, I came to the understanding that those who are insulin resistant or have Type 2 Diabetes or have other indicators that they are not tolerating large amounts of carbohydrate well could improve their symptoms significantly by following a lower carb style of eating, with the oversight of their doctors. Such an adjustment in lifestyle seemed like a small price to pay for the potential of significantly improving – and in some cases reversing symptoms of these conditions, especially when compared with the reality that at best these symptoms will stay the same and very likely will get worse over time.
Many scientific studies as well as physician’s clinical experience indicate that a lower carb style of eating combined with extending the time between meals lowers insulin resistance (which is the underlying cause of high blood sugar). When insulin levels are lowered, blood pressure comes down and triglycerides and some other lipid ratios normalize.
Physicians across Canada, the US, the UK and Australia that prescribe a LCHF Diet to their patients have found that they experience a significant improvement in the symptoms of insulin resistance, Type 2 Diabetes, high blood pressure, high triglycerides and that a natural reversal of many symptoms is possible. Such improvements often enable these doctors to reduce- and sometimes discontinue medications that were previously prescribed to their patients for these conditions. While the American Diabetes Association enables Type 2 Diabetics to choose to follow either a moderate low carb diet (130g carbohydrate) or a low fat calorie restricted diet for up to a year for weight loss, as of yet this approach is not approved by Diabetes Canada.
A low carb diet isn’t new. In fact this was the standard recommendation prior to the discovery of insulin.
It seems to me that a lower carbohydrate intake resulting in improved symptoms and lab results as overseen by one’s own doctor is preferable to living with chronic disease symptoms and taking increasing numbers of medications in an effort to manage symptoms, but each person needs to evaluate the alternative and make their own choice.
For those who want to aim to improve or reverse the symptoms of these chronic diseases, I offer services as the LCHF-Dietitian.
Janssen I, The Public Health Burden of Obesity in Canada, Canadian Journal of Diabetes, 37 (2013), pg. 90-96
from the Public Health Collaborative, Summary Table of Randomized-Controlled Trials Comparing Low Carb to Low-Fat Diets – https://phcuk.org/:
[1] A Randomized Trial Comparing a Very Low Carbohydrate Diet and a Calorie-Restricted Low Fat Diet on
Body Weight and Cardiovascular Risk Factors in Healthy Women. Brehm et al.
http://press.endocrine.org/doi/full/10.1210/jc.2002-021480
[2] A Randomized Trial of a Low-Carbohydrate Diet for Obesity. Foster et al.
http://www.nejm.org/doi/full/10.1056/NEJMoa022207
[3] A Low-Carbohydrate as Compared with a Low-Fat Diet in Severe Obesity. Samaha et al.
http://www.nejm.org/doi/full/10.1056/NEJMoa022637
[4] Effects of a low-carbohydrate diet on weight loss and cardiovascular risk factor in overweight adolescents.
Sondike et al. http://www.sciencedirect.com/science/article/pii/S0022347602402065
[5] The National Cholesterol Education Program Diet vs a Diet Lower in Carbohydrates and Higher in Protein
and Monounsaturated Fat A Randomized Trial. Aude et al. http://archinte.jamanetwork.com/article.aspx?
articleid=217514
[6] A Low-Carbohydrate, Ketogenic Diet versus a Low-Fat Diet To Treat Obesity and Hyperlipidemia: A
Randomized, Controlled Trial. Yancy et al. http://annals.org/article.aspx?articleid=717451
[7] Comparison of energy-restricted very low-carbohydrate and low-fat diets on weight loss and body
composition in overweight men and women. Volek et al.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC538279/
[8] Comparison of a Low-Fat Diet to a Low-Carbohydrate Diet on Weight Loss, Body Composition, and Risk
Factors for Diabetes and Cardiovascular Disease in Free-Living, Overweight Men and Women. Meckling et
al. http://press.endocrine.org/doi/full/10.1210/jc.2003-031606
[9] Lack of suppression of circulating free fatty acids and hypercholesterolemia during weight loss on a highfat,
low-carbohydrate diet. Hernandez et al. http://ajcn.nutrition.org/content/91/3/578.long
[10] Perceived Hunger Is Lower and Weight Loss Is Greater in Overweight Premenopausal Women
Consuming a Low-Carbohydrate/High-Protein vs High-Carbohydrate/Low-Fat Diet. Nickols-Richardson et al.
http://www.sciencedirect.com/science/article/pii/S000282230501151X/
[11] Short-term effects of severe dietary carbohydrate-restriction advice in Type 2 diabetes—a randomized
controlled trial. Daly et al. http://onlinelibrary.wiley.com/doi/10.1111/j.1464-5491.2005.01760.x/abstract
[12] Separate effects of reduced carbohydrate intake and weight loss on atherogenic dyslipidemia. Krauss et
al. http://ajcn.nutrition.org/content/83/5/1025.full
[13] Comparison of the Atkins, Zone, Ornish, and LEARN Diets for Change in Weight and Related Risk
Factors Among Overweight Premenopausal Women The A TO Z Weight Loss Study: A Randomized Trial.
Gardner et al. http://jama.jamanetwork.com/article.aspx?articleid=205916
[14] Low- and high-carbohydrate weight-loss diets have similar effects on mood but not cognitive
performance. Halyburton et al. http://ajcn.nutrition.org/content/86/3/580.long
[15] A low-carbohydrate diet is more effective in reducing body weight than healthy eating in both diabetic
and non-diabetic subjects. Dyson et al. http://onlinelibrary.wiley.com/doi/10.1111/j.1464-
5491.2007.02290.x/full
[16] The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in
type 2 diabetes mellitus. Westman et al. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2633336/
[17] Weight Loss with a Low-Carbohydrate, Mediterranean, or Low-Fat Diet. Shai et al.
http://www.nejm.org/doi/full/10.1056/NEJMoa0708681
[18] Effects of weight loss from a very-low-carbohydrate diet on endothelial function and markers of
cardiovascular disease risk in subjects with abdominal obesity. Keogh et al.
http://ajcn.nutrition.org/content/87/3/567.long
www.PublicHealthCollaboration.org
[19] Metabolic Effects of Weight Loss on a Very-Low-Carbohydrate Diet Compared With an Isocaloric HighCarbohydrate
Diet in Abdominally Obese Subjects. Tay et al.
http://www.sciencedirect.com/science/article/pii/S0735109707032597
[20] Carbohydrate Restriction has a More Favorable Impact on the Metabolic Syndrome than a Low Fat Diet.
Volek et al. http://link.springer.com/article/10.1007/s11745-008-3274-2
[21] Long-term effects of a very-low-carbohydrate weight loss diet compared with an isocaloric low-fat diet
after 12 mo. Brinkworth et al. http://ajcn.nutrition.org/content/90/1/23.long
[22] Efficacy and Safety of a High Protein, Low Carbohydrate Diet for Weight Loss in Severely Obese
Adolescents. Krebs et al. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2892194/
[23] In type 2 diabetes, randomisation to advice to follow a low-carbohydrate diet transiently improves
glycaemic control compared with advice to follow a low-fat diet producing a similar weight loss. Guldbrand et
al. http://link.springer.com/article/10.1007/s00125-012-2567-4/fulltext.html
[24] A Randomized Pilot Trial of a Moderate Carbohydrate Diet Compared to a Very Low Carbohydrate Diet
in Overweight or Obese Individuals with Type 2 Diabetes Mellitus or Prediabetes. Saslow et al.
http://www.plosone.org/article/info:doi/10.1371/journal.pone.0091027
[25] Effects of Low-Carbohydrate and Low-Fat Diets: A Randomized Trial. Bazzano et al.
http://annals.org/article.aspx?articleid=1900694
[26] The Role of Energy Expenditure in the Differential Weight Loss in Obese Women on Low-Fat and Low Carbohydrate
Diets. Brehm et al. http://press.endocrine.org/doi/full/10.1210/jc.2004-1540
[27] Effects of a Low Carbohydrate Weight Loss Diet on Exercise Capacity and Tolerance in Obese Subjects.
Brinkworth et al. http://onlinelibrary.wiley.com/doi/10.1038/oby.2009.134/full
[28] Comparative Study of the Effects of a 1-Year Dietary Intervention of a Low-Carbohydrate Diet Versus a
Low-Fat Diet on Weight and Glycemic Control in Type 2 Diabetes. Davis et al.
http://care.diabetesjournals.org/content/32/7/1147
[29] Weight and Metabolic Outcomes After 2 Years on a Low-Carbohydrate Versus Low-Fat Diet: A
Randomized Trial. Foster et al. http://annals.org/article.aspx?articleid=745937
[30] Effects of a Low-intensity Intervention That Prescribed a Low-carbohydrate vs. a Low-fat Diet in Obese,
Diabetic Participants. Iqbal et al. http://onlinelibrary.wiley.com/doi/10.1038/oby.2009.460/full
[31] Consuming a hypocaloric high fat low carbohydrate diet for 12″…weeks lowers C-reactive protein, and
raises serum adiponectin and high density lipoprotein-cholesterol in obese subjects. Ruth et al.
http://www.metabolismjournal.com/article/S0026-0495(13)00223-0/abstract
[32] Comparison of isocaloric very low carbohydrate/high saturated fat and high carbohydrate/low saturated
fat diets on body composition and cardiovascular risk. Noakes et al.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1368980/
[33] Long-term Effects of a Very Low-Carbohydrate Diet and a Low-Fat Diet on Mood and Cognitive
Function. Brinkworth et al. http://archinte.jamanetwork.com/article.aspx?articleid=1108558
[34] The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: one-year
follow-up of a randomized trial. Stern et al. http://www.ncbi.nlm.nih.gov/pubmed/15148064
[35] A Randomized Trial of a Low-Carbohydrate Diet vs Orlistat Plus a Low-Fat Diet for Weight Loss. Yancy
et al. 2010. http://www.ncbi.nlm.nih.gov/pubmed/20101008
[36] A randomized controlled trial of low carbohydrate and low fat/high fiber diets for weight loss. Baron et al.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1646726/
[37] A very low-carbohydrate, low-saturated fat diet for type 2 diabetes management: a randomized trial. Tay
et al. http://www.ncbi.nlm.nih.gov/pubmed/25071075
[38] Randomised controlled trial of four commercial weight loss programmes in the UK: initial findings from
the BBC ”diet trials”. Truby et al. http://www.bmj.com/content/332/7553/1309
www.PublicHealthCollaboration.org
[39] Comparison of the Atkins, Ornish, Weight Watchers, and Zone Diets for Weight Loss and Heart Disease
Risk Reduction:A Randomized Trial. Dansinger et al. http://jama.jamanetwork.com/article.aspx?
articleid=200094
[40] Very Low-Carbohydrate and Low-Fat Diets Affect Fasting Lipids and Postprandial Lipemia Differently in
Overweight Men. Sharman et al. http://jn.nutrition.org/content/134/4/880.long
[41] Comparison of high-fat and high-protein diets with a high-carbohydrate diet in insulin-resistant obese
women. McAuley et al. http://link.springer.com/article/10.1007/s00125-004-1603-4/fulltext.html
[42] Diet-Induced Weight Loss Is Associated with Decreases in Plasma Serum Amyloid A and C-Reactive
Protein Independent of Dietary Macronutrient Composition in Obese Subjects. O’Brien et al.
http://press.endocrine.org/doi/10.1210/jc.2004-1011
[43] Advice to follow a low-carbohydrate diet has a favourable impact on low-grade inflammation in type 2
diabetes compared with advice to follow a low-fat diet. Jonasson et al.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4025600/
[44] A non-calorie-restricted low-carbohydrate diet is effective as an alternative therapy for patients with type
2 diabetes. Yamada et al. http://www.ncbi.nlm.nih.gov/pubmed/24390522
[45] Low-Fat Versus Low-Carbohydrate Weight Reduction Diets Effects on Weight Loss, Insulin Resistance,
and Cardiovascular Risk: A Randomized Control Trial. Bradley et al.
http://diabetes.diabetesjournals.org/content/58/12/2741.long
[46] Weight loss with high and low carbohydrate 1200 kcal diets in free living women. Lean et al.
http://www.nature.com/ejcn/journal/v51/n4/abs/1600391a.html
[47] Evaluation of weight loss and adipocytokines levels after two hypocaloric diets with different
macronutrient distribution in obese subjects with rs9939609 gene variant. De Luis et al.
http://onlinelibrary.wiley.com/doi/10.1002/dmrr.2323/abstract
[48] Enhanced weight loss with protein-enriched meal replacements in subjects with the metabolic syndrome.
Flechtner-Mors et al. http://onlinelibrary.wiley.com/doi/10.1002/dmrr.1097/abstract
[49] Long-term effects of a low carbohydrate, low fat or high unsaturated fat diet compared to a nointervention
control. Lim et al. http://www.nmcd-journal.com/article/S0939-4753(09)00124-0/abstract
[50] A randomized study comparing the effects of a low-carbohydrate diet and a conventional diet on
lipoprotein subfractions and C-reactive protein levels in patients with severe obesity. Seshadri et al.
http://www.amjmed.com/article/S0002-9343(04)00344-4/abstract
[51] Comparison of low- and high-carbohydrate diets for type 2 diabetes management: a randomized trial.
Tay et al. http://ajcn.nutrition.org/content/early/2015/07/29/ajcn.115.112581.abstract
[52] Weight loss on low-fat vs. low-carbohydrate diets by insulin resistance status among overweight adults
and adults with obesity: A randomized pilot trial. Gardner et al.
http://onlinelibrary.wiley.com/doi/10.1002/oby.21331/abstract
[53] Metabolic impact of a ketogenic diet compared to a hypocaloric diet in obese children and adolescents.
Partsalaki et al. http://www.ncbi.nlm.nih.gov/pubmed/23155696
[54] A randomized controlled trial of 130 g/day low-carbohydrate diet in type 2 diabetes with poor glycemic
control. Sato et al. http://www.clinicalnutritionjournal.com/article/S0261-5614(16)30169-8/pdf
[55] Short-term safety, tolerability and efficacy of a very low-calorie-ketogenic diet interventional weight loss
program versus hypocaloric diet in patients with type 2 diabetes mellitus. Goday et al.
http://www.nature.com/nutd/journal/v6/n9/full/nutd201636a.html
[56] Visceral adiposity and metabolic syndrome after very high—fat and low-fat isocaloric diets: a randomized
controlled trial. Veum et al. http://ajcn.nutrition.org/content/early/2016/11/30/ajcn.115.123463.abstract
[57] An Online Intervention Comparing a Very Low-Carbohydrate Ketogenic Diet and Lifestyle
Recommendations Versus a Plate Method Diet in Overweight Individuals With Type 2 Diabetes: A
Randomized Controlled Trial. Saslow et al. https://www.ncbi.nlm.nih.gov/pubmed/28193599
It bothers me when people make negative comments about a Low Carb High Fat (LCHF) style of eating, without really understanding what it is – and what it isn’t. This article addresses a few of the common misconceptions about a Low Carb lifestyle that were presented in a recent French-language newspaper article.
FALLACY: “The LCHF diet targets a very low carbohydrate and high-fat diet, aimed at rapid weight loss.”
FACT 1: Firstly, there is no single LCHF diet.
The Atkins Diet is one kind of LCHF diet, so is a Paleo Diet, and these are substantially different from each other. There are LCHF diets written by non-healthcare professionals such as the “Bulletproof Diet”, as well as those from Dr. Jason Fung, a Nephrologist (kidney specialist) from Toronto and from Dr. Eric Westman of Duke University. Referring to “the” LCHF diet fails to take this huge range into account.
FACT 2: There is no one “goal” of LCHF diets.
From my experience, most of the well-designed LCHF diets written by healthcare professionals and researchers are aimed at lowering insulin resistance (IR), which underlies the symptom of high blood sugar and Type 2 Diabetes. Weight loss is a natural byproduct of eating in such a way as to lower IR.
FACT 3: LCHF diets that focus on weight management rarely aim for “rapid weight loss”.
LCHF diets designed by healthcare professionals with a weight management goal generally aim for consistent weight loss and/or inches lost, and reducing abdominal obesity. Morbidly obese people or those with a great deal of weight to lose and who begin eating low-carb will lose weight rapidly at first, firstly from water-loss and then from fat loss. That is not the aim, but the result.
FALLACY: “this diet is so restrictive”…
FACT 4: “this diet…”
Which LCHF diet? As mentioned above, there are many different LCHF-style diets and they differ substantially from each other.
Fact 5: The term “restrictive” is not defined, so this statement really has no meaning.
What are all LCHF diets “restrictive” in?
Foods that are not included on an Atkins Diet are very different from what is not included on a Paleo Diet. Dr. Fung’s recommendations differ from Dr. Westman’s. For example, Dr. Fung does not limit any fats, and Dr. Westman does.
Which LCHF-diet is “restrictive” and in what foods or nutrients?
FALLACY: “this diet is so restrictive that the likelihood that the people who adopt it will drop it in the short or medium term is high.”
FACT 6: Which LCHF diet is restrictive and what is it restrictive in? Is there evidence to support that people that stop eating those foods regularly are unable to continue to do so in the short- or medium term?
FALLACY: “There is a difference between processed high-carbohydrate foods such as juice, sweetened beverages, white bread, pastries and sweets, and whole foods high in unprocessed carbohydrates such as brown rice, whole wheat, vegetables, fruits, legumes , which are associated with good health and the prevention of the risk of diabetes, cardiovascular disease and obesity.“.
FACT: 7: all carbohydrates (whether from juice, fruit, pastry, brown rice or whole wheat) are broken down and supply the blood with glucose.
FACT 8: how quickly all carbohydrates are broken down to glucose varies.
FACT 9: how much insulin is released in response to all of these different carbohydrates is what most well-designed LCHF diets endeavor to address.
FALLACY: “Whenever an attempt is made to isolate a nutrient (carbohydrates, proteins or lipids) and make it responsible for all ills, it is wrong. The reality is that we need these three nutrients for the health and enjoyment of eating.”
FACT 10: Well-designed LCHF-diets have all three macronutrients in them; carbohydrates, protein and fat.
The major difference is LCHF diets are low in carbohydrate and high in fat. Which carbohydrates are eaten on different LCHF diets vary. Paleo diets for example eat starchy vegetables that ketogenic-style LCHF diets don’t. In addition, which fats are promoted in the different styles of LCHF diets also differs. Paleo diets are known for promoting lots of red meat, including processed meat such as bacon and sausage and lots of full-fat cream and butter.
LCHF diets, such as the one I teach, include the saturated fat found naturally in foods, such as in steak or in cheese but encourage the “high fat” part of the diet to come from mono-unsaturated fruits such as avocado and olives, from a wide variety of nuts and seeds, as well as from the oils from these foods as well as from omega 3 fats found in fish. It also includes the carbohydrates found in an abundance of non-starchy vegetables, specific fruit, nuts and seeds. A look at just a few of the recipe ideas posted on this web site, certainly do not indicate a “restrictive diet”.
FACT 11: The Dietary Guidelines in Canada (and the US) have “attempted to isolate a nutrient – fat, and make it responsible for all ills”.
In 1977, the Dietary Guidelines in both countries were first changed to restrict fat intake from all sources, especially saturated fat, in the belief that eating fat contributed to heart disease (see previous articles).
While it is now known that dietary fats do not cause heart disease, and even the Canadian Heart and Stroke Foundation changed their recommendations in this regard, it is my conviction that it was this vilification of fat and the corresponding promotion of diets very high in carbohydrates (45-65% of daily calories as carbs) that contributed to the dual obesity- and Diabetes epidemics that we now have.
Some final thoughts…
A LCHF-style of eating can be done safely, with slow yet consistent weight loss, while being overseen by one’s doctor and monitoring blood glucose and lab work.
It certainly doesn’t have to be restrictive, as one can eat meat, fish, seafood, poultry, cheese and other dairy, vegetables and fruit, nuts and seeds. It can provide a nutritionally adequate diet – certainly no less adequate that the average Canadian eats, following Eating Well with Canada’s Food Guide [see Do Canadian Adults Meet Their Nutrient Requirements Through Food Intake Alone? Health Canada, 2012, Cat.No.: H164-112/3-2012E-PDF].
Note: Everyone's results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody's nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
I am not one for popular remedies for health issues. I don’t believe in “cleanses” and I don’t “eat clean” – or do I? If not eating any dairy is “clean” then I eat “dirty” because I use cream in my coffee, but if not eating gluten or grains is “clean”, then my eating is pristine.
The problem with popular beliefs around food and eating and word-of-mouth remedies is there is no standardized means to define them or evaluate their effectiveness.
Folk Remedies
Folk remedies, on the other hand, are in a different category. These practices, on which many nutraceuticals and even pharmaceuticals are based have GRAS standing (“Generally Recognized As Safe”) and have been used by cultures around the world for hundreds, if not thousands of years.
Here’s are two examples of folk-remedies in this category;
Swallow’s Nest
The Chinese have made soup out of the nest of a particular swallow which builds its home on high cliffs. This “bird’s nest soup” is highly prized and very expensive to make, but considered to have restorative properties for those with breathing difficulties. As it turns out, this particular swallow’s nest is high in theophilline, a compound that has come to be used in Western medicine as therapy for respiratory diseases such as chronic obstructive pulmonary disease (COPD) and asthma. Bird’s nest from this swallow has a GRAS standing and can legally be purchased in traditional Chinese medicine stores. One can take medication or food containing the same active substance, and in both cases one’s symptoms improve.
Bitter Melon
Bitter melon or bitter gourd / karela is widely grown in Asia, Africa and the Caribbean – both for food (prized for its bitter taste) and for its medicinal properties. In both Ayurveda, the traditional medicine (Hindu) of India and in Traditional Chinese Medicine (TCM) different parts of the bitter melon plant are brewed as a beverage and taken as a treatment for Diabetes. As it turns out, bitter melon, which has GRAS standing, contains polypeptide-p which is an insulin analogue.
Apple Cider Vinegar
I’ve been hearing about the use of apple cider vinegar (ACV) since I first started reading about low carb high fat diets in early 2015, from Dr. Jason Fung, a nephrologist (kidney specialist) from Toronto. He recommended that 1 Tbsp. of unpasteurized ACV be taken in a glass of water prior to meals and that it be add it to broths, soups and marinades. He’d said that it inactivates the production of digestive enzymes and slows down the rate of digestion, stabilizing blood sugar levels. Since the recommendation to use ACV at the time did not come with any scientific evidence, I summarily dismissed the idea of using it.
Persistently High Fasting Blood Glucose
For those who have been following my own progress following a Low Carb High Fat style of eating over the past 6 months (posted on the tab “A Dietitian’s Journey”) you know that despite losing weight, significantly lowering both my triglycerides and LDL cholesterol and my overall blood sugar levels coming down significantly, I had two ongoing problems;
(1) my morning fasting blood glucose (FBG) remained high, and
(2) my blood glucose would only drop into the 5-point-something mmol/ L range (~94 mg/dl) or to the 4-point-something mmol/ L range (76 mg/dl) range after an entire day of intermittent fasting.
Since there are physiological risks associated with high blood glucose, I was very motivated to find out why they were high in the morning and to do something about them.
I decided to keep detailed food records for 3 weeks to see if there was a patter, and ruled out diet.
Then, I decided to take my blood sugar several times each night, from midnight until 8 am, over several days, to see when it rose. As it turned out, it would drop nicely after supper (as it would after eating at any other time of the day), to 7-point-something mmol/l (~130 mg/dl) after an hour or so, and then to 6-point-something mmol/L (121 mg/dl) around midnight, and then it would gradually begin to rise from ~2 am, reaching its highest point around 8 am, following the circadian rhythm of cortisol.
Since it seemed that my high morning blood sugar was due to cortisol rising after went to bed until 8 am, and since cortisol can be affected by many things including stress, I took up going for a walk after supper. It did help! My morning blood sugars were in the mid-6-point-something mmol/L (~117 mg/dl), which was a far-cry from the 8.0 mmol/L (144 mg/dl) level it had been!
The evening walks, however, were short lived due to a shift in the winds and the raging forest fires in and around the Lower Mainland which caused the skies to fill with Fine Particulate Matter, know as PM2.5 (as the are 2.5 micrometers or less, in size). Since these can enter the lungs and the blood stream resulting in ill-effects, my walks stopped. In fact, if I did have to go out, it was with a vented N-95 mask. The smoke briefly cleared being replaced by stifling heat in the mid- to high-30 Celsius (100 F) for 10 days, followed by more smoke, so I began to look for something- anything that might lower my morning blood sugars, which at this point were hovering in the 7.6 mmol/L mmol/L (137 mg/dl) range!
At first I tried doing a short workout on my Nordic-track or using my “step” before bed, but it didn’t do much for my blood sugars and made me far too awake to fall asleep.
Having some unpasteurized, unfiltered ACV in the house, I decided to try it. It tasted terrible!! I tried adding it to water and it was still awful! I couldn’t bring myself to drink it!!
From Masking the Taste to Food as Medicine
A few years ago, in an effort to drink more water each day, I began drinking Club Soda / Selzer and then purchased a Sodastream machine, to carbonate my own (filtered) water.
I usually drink it plain, but have been known to put a twist of fresh lemon or lime in it.
ACV Ginger-aid
I tried adding 1 Tbsp of unpasteurized ACV to 1 litre (quart) of carbonated water but I still couldn’t drink it! All I tasted was sour!
Needing to mask the taste, I decided to grate a bit of fresh ginger root into it and “ACV Gingeraid” was born!
The first time, I drank a litre (~ quart) of “ACV Gingeraid” mid-morning, and my blood sugar dropped from 7.3 mmol/L (132 mg/dl) to 6.6 mmol/L (119 mg/dl) in an hour. I thought to myself that maybe it would have dropped the same amount if I had done nothing.
I hadn’t had anything to eat or drink (except a coffee with only cream in the morning) but presumably under the effect of cortisol and my body’s own making of glucose from fat stores, my blood sugar continued to rise from 6.6 mmol/L (119 mg/dl) at 5:30 AM, to 7.7 mmol/L (139 mg/dl) just before 10 AM.
That was just too high – and I hadn’t eaten!
So, I made and drank a second bottle of ACV Ginger-aid and in 1.5 hrs, my blood sugar had dropped to 6.3 mmol/L (114 mg/dl). Then by 4:00 PM, and drinking no additional ACV Ginger-aid, it was 4.8 mmol/L (86 mg/dl).
I would previously only get to those kinds of numbers just before dinner, when I was on an intermittent fast day. This was 2-2.5 hours earlier.
That couldn’t be, I thought…
Several days in a row, the same thing would happen, with only slightly different numbers, some of them lower.
My blood sugar would be around 7.3 mmol/L (137 mg/dl) 2 hours after dinner and I would drink most of a bottle of ACV Ginger-aid before bed, and in the morning my FBG would be in the 6’s mmol/L (~119 mg/dl). Could it be because of the drink?
One day, quite by chance, I had some fresh turmeric root in the house (because I use it in cooking and because I like the taste). As well, is a potent antioxidant and the curcumin (the active compound in turmeric) has been demonstrated to have anti-carcinogenic properties).
I decided to add a little bit of grated turmeric root because I thought the turmeric would taste good with the ginger (it did!).
I also added a bit of freshly ground black pepper to the Turmeric-ACV Ginger-aid, because I had read that black pepper makes the curcumin in the fresh turmeric root 2000 times more bio-available.
Turmeric ACV Ginger-aid
The drink tasted delicious!
But what happened to my blood sugars was quite surprising.
It became evident that for me, using “food as medicine” has had some very impressive results!
Just 3 days earlier, I was impressed because by 4:00 PM my blood glucose was 4.8 mmol/L (86 mg/dl) – which was a good 2.5 hours earlier than usual.
Since adding the turmeric to the ACV Ginger-aid, I was getting numbers in the mid-4 mmol/L (i.e. 4.6 mmol/L / 84 mg/dl) by 2:30 in the afternoon!
By drinking the Turmeric-ACV Ginger-aid before bed, my morning FBG is consistently in the low 6’s mmol/L (~110 mg/dl) and on a few occasions, ”ve been getting numbers in the high-5s mmol/L (103 mg/dl). I was considering Metformin to get these kinds of results!
This is by consuming ordinary food found in my kitchen!
I continue to eat LCHF and I usually intermittent fast breakfast, as I’ve never been much of a “breakfast person”. I occasionally don’t eat until mid-day as that is when I usually first feel hungry.
My blood sugars are the best they’ve been since I started measuring them.
Now, 2 hours after meals my blood sugar is usually in the low 6’s mmol/l (~110 mg/dl) and the ONLY change has been adding this beverage before bed and occasionally one plain ACV Ginger-aid through the day.
Just to be a ‘good scientist’, last night I deliberately ate 1/2 a dark chocolate bar (72% cocoa) and drank 3/4 of a bottle of plain AVC Ginger-aid (no turmeric) and tested my blood glucose this morning. It was 6.6 mmol/L (119 mg/dl). That’s crazy! I was expecting 10 or 11 mmol/L. That’s what it used to be just a few weeks ago, when I’d eat a little bit of dark chocolate!
NOTE: I wanted to see what would happen if I ate the same way but discontinued the beverage. My blood sugar went up to 8.8 mmol/L the first morning after not having any the previous day and was 8.6 mmol/L the following morning. The third day, I drank only one bottle in the afternoon and on at night before bed and the following morning, my fbg was 7.2 mmol/L (still way too high, but much lower). I anticipate it will continue to drop as I have 2-3 bottles of the mixture per day.
Even thought I am NOT exercising (first because of the smokey conditions outside and because I fell back into old “bad-habits” of getting up early and working at my desk with my coffee), my blood glucose is what I would have anticipated would have occurred if I had taken Metformin.
Keep in mind, I am “a sample-set of one”. There’s no saying that others will have the same, or even similar results. In addition, I do NOT encourage people to make any changes in the amount of medication that a doctor prescribed without being told by that doctor. This drink is NOT a substitute for medication that has been prescribed! That being said, for those who are not taking medication but have persistently high blood sugar readings does it not make good sense to consider trying such food as medicine?
NOTE: I decided to find out if there was any scientific evidence for the anti-glycemic properties of ACV and did find a 2015 study, suggesting that it increases insulin-stimulated glucose uptake in those with Type 2 Diabetes (T2D), which I have. I then decided to look and see if ginger had anti-glycemic properties and found a 2015 study that reported that ginger significantly reduced FBG as well as HbA1c, along with Apo B, Apo B/Apo A-I, MDA and increased the level of Apo A-I in T2D patients. Naturally, I looked to see if turmeric was known to have anti-glycemic properties and sure enough, it did! I found a 2013 publication that indicated it is well-known that turmeric has a stimulatory action on pancreatic β-cells, and that this may be the mechanism by which it lowers blood sugar in those with T2D. Whether these substances used together have a far greater effect on blood sugar than any of them used separately would certainly make for an interesting study!
WARNING: Given the possibility of these ordinary foods resulting in a dramatic drop in blood sugar, if you have Type 2 Diabetes or pre-diabetes, first discuss incorporating these foods into your diet with your doctor. As well, be sure to monitor your high blood sugar often if you drink these.
ACV Gingeraid Recipe
Click on the link under “Recipes” for ACV Gingeraid with Variations – food as medicine. Enjoy!
Mitrou P, Petsiou E, Papakonstantinou E, et al. Vinegar Consumption Increases Insulin-Stimulated Glucose Uptake by the Forearm Muscle in Humans with Type 2 Diabetes. Journal of Diabetes Research. 2015;2015:175204. doi:10.1155/2015/175204.
Khandouzi N, Shidfar F, Rajab A, Rahideh T, Hosseini P, Mir Taheri M. The Effects of Ginger on Fasting Blood Sugar, Hemoglobin A1c, Apolipoprotein B, Apolipoprotein A-I and Malondialdehyde in Type 2 Diabetic Patients. Iranian Journal of Pharmaceutical Research”¯: IJPR. 2015;14(1):131-140.
Zhang D, Fu M, Gao S-H, Liu J-L. Curcumin and Diabetes: A Systematic Review. Evidence-based Complementary and Alternative Medicine”¯: eCAM. 2013;2013:636053. doi:10.1155/2013/636053.
Note: Everyone's results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody's nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
When people think of getting enough “fiber” they often imagine foods like “bran” and prunes – foods not usually eaten when one is following a LCHF style of eating. But what is fiber and how do we get enough when we don’t generally eat grains or legumes?
Fiber – soluble and insoluble
There are two kinds of fiber, insoluble and soluble.
Insoluble fiber is what most people think about when they think of “roughage” needed to form stool and prevent constipation. It helps form the bulk of the stool. Insoluble fiber is naturally present in the outside of grains, such as whole grain wheat, un-milled brown rice and the outside of oats. It is also found in fruit, legumes (or pulses) such as dried beans, lentils, or peas, some vegetables and in nuts and seeds.
Soluble fiber forms a ‘gel’ in the intestine and binds with fatty acids. It slows stomach emptying and helps to make people feel fuller for longer, as well as slow the rate that blood sugar rises, after eating. Soluble fiber absorbs water in the gut, and helps to form a pliable stool. Soluble fiber is found on the insideof certain grains, such as oats, chia seeds or psyillium, as well as the inside of certain kinds of fruit such as apple and pear.
Dietary Recommendations for dietary fiber intake varies with age and gender. Men under the age of 50 years are recommended to take in 38 gm / day of dietary fiber, and men over 50 years to take in 30 gm / day. Women under 50 years old are recommended to take in 25 gm of fiber per day and over 50 years, 21 gm per day.
[Reference: Government of Canada, nutrients in food, https://www.canada.ca/en/health-canada/services/nutrients/fibre.html]
Both kinds of fiber are needed and most Canadians eating a conventional diet are getting half of what is recommended.
For those eating a Low Carb High Fat Diet, even though grains and legumes are generally not eaten, getting enough fiber is not that difficult.
Avocado – Surprisingly, avocado which is an excellent source of vegetable fat, is also high in fiber, having more than 10 gm fiber per cup (250 ml). Avocado grown in Florida which are the bright green, smooth-skinned variety have more insoluble fiber than California avocado, which are the smaller, darker green, dimpled variety.
Berries – Berries such as blackberries and raspberries are fruit that I encourage people to use sprinkled on salads, as they are an excellent source of antioxidants, but also have 8 gm fiber per cup (250 ml).
Coconut – Fresh coconut meat has 6 gm of net carbs per 100 grams of coconut, but also packs a whopping 9 gms of fiber and is a very rich source of fat (33 gms per 100 gm coconut). It can be purchased peeled, grated and sold frozen in many ethnic stores or in the ethnic section of regular grocery stores.
Artichoke – Artichoke is a low-carbohydrate vegetable that is delicious boiled and it’s leaves dipped in seasoned butter. Surprisingly, one medium artichoke has over 10 gm of fiber.
Okra – Okra, or ‘lady fingers’ is a staple vegetable in the South Asian diet and is commonly eaten in the Southern US. Just one cup of okra contains more than 8 gm of fiber.
Brussels Sprouts – These low-carb cruciferous vegetables are not just for Thanksgiving and Christmas dinner. Split and grilled on the BBQ with garlic, they are a sweet, nutty addition to any meal, packing almost 8 gm of fiber per cup.
Turnip – Turnip, the small white vegetable with a hint of purple is not to be confused with the pale beige, larger rutabaga. Turnip contains almost 10 gm of fiber per cup. It is delicious pickled with a single beet, and eaten with Middle Eastern foods.
Constipation
Even though passing stool is as natural a part of the process as eating is, most feel awkward discussing it. Many don’t know what “normal” is in that regard, or even if there is such a thing. Is once every few days okay, is it detrimental if it is only once a week? Should it be every day and if so, is more than once a day too much? Does texture matter or is it only frequency?
Frequency and Texture
Many physicians consider normal bowel movement (BM) frequency from 3/day to every 3 days whereas I tend to lean towards daily to every two days as preferable. Even if BM frequency is in this range, hard, painful to pass stools are problematic and would be categorized as constipation.
Since the mid-1990s there is a standardized method to classify the texture of stools, called the Bristol Stool Chart based on research which indicated that stool is a useful surrogate measure of how long feces (stool) takes to go through the large intestine (called “colon transit time”).
Bristol Stool Chart
While Type 3-7 are considered valid for diagnosing diarrhea, Type 1 and Type 2 stool can have normal “transit time”, but be compact and hard due to lack of fluid / water.
The fact is, many, if not most people either have a lack of fiber or a lack of sufficient fluid or both and are constipated to a greater or lesser degree. They eat every day, but they don’t pass stool often and when they do, it is hard and compact. Their bodily waste sits in their colon for several days before finally being eliminated – and when it is, it is hard, dry and compact and often painful to pass.
Constipation is usually due to two factors;
(1) not taking in foods with enough fiber and
(2) not drinking enough water
Sometimes, despite eating the foods mentioned above, people find it isn’t sufficient. This is where what I have dubbed “birdseed” comes in. Of course, I don’t mean actual birdseed!
What I call “birdseed” is a mixture of 1 tbsp. freshly ground whole flax seed (3 gm fiber per tbsp.) to which 1 tbsp. of chia seed is added (5.5 gm fiber per tbsp.).
The chia seeds are ground a little bit with the previously ground flax seed, and then the two ground seeds are placed in a small bowl.
An added portion of psyllium husk (1 tbsp.) is optional.
Drinking “Birdseed”
To drink this mixture, diluted coconut milk can be added, the mixture briefly stirred and then drunk quickly, followed by a good amount of water (I recommend at least 2 cups (500 ml).
Eating “birdseed”
For even more fiber and a delicious taste, 2 tbsp. of tahini (ground sesame paste) can be added and the mixture eaten with a spoon.
Tahini has 0 net carbs, and almost 4 gm of fiber for 2 tbsp.
Note: people often ask if they can make “chia pudding” to which they add ground flax seed, but the idea here is to have the flax and chia seeds do their magic in the intestines, not in a container, beforehand.
Water – how much is sufficient?
Dehydration is another factor that contributes to constipation. Often people simply don’t drink enough water to form a bulky, pliable stool.
The Reference Daily Intake (RDI) for water for men over 18 years is 3.7 liters per day and for women over 18 years, 2.7 liters per day and this is from all water, including that contained in beverages.
Fiber and water together
Drinking one liter of water or club soda / seltzer with each batch of “birdseed” is a good idea, because the last thing we want is to have all this insoluble and soluble fiber this in our intestines, with insufficient water. In the worse case scenario, this can result in an intestinal blockage, so be sure to drink sufficient water when taking “birdseed”.
I usually recommend that people start off with having 1 tbsp of flax seed and 1 tbsp of chia seed once a day – increasing after a few days if needed to twice (or if needed, three times) a day – making sure to drink a liter of water immediately afterwards.
What about carbs in “birdseed”?
While flax seed, chia seed and psyllium are grains, they have very few net carbs.
1 tsp of whole flax seed (3.4 gm) is so high in fiber that it has no net carbs.
1 tsp of whole chia seed has only .3 gm of net carbs.
Even if you add 1 tsp of psyllium husk, that adds only 1 gram of carbs.
“Birdseed” can be drunk as described above, eaten with sesame paste (also very high in fiber and a good source of healthy fat), or sprinkled on salads or omelettes.
…and remember to drink a liter or so of water each time you take “birdseed”, so that passing stools daily, just like eating daily, will be the norm.
Note: Everyone’s results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody’s nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Finally! Like anyone else who’s been working long and hard towards achieving their health goals, I’m so excited that I’ve finally made a significant ‘breakthrough’! I didn’t think it would take this long, but when I think that it has taken me close to 20 years to become this insulin resistant, it only makes sense that it is going to take some time to become insulin sensitive again!
Last night, for the first time since I was diagnosed with Type 2 Diabetes (T2D) ten years ago, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl).
To put that in context for someone without Diabetes, blood glucose taken two hours after meals should be less than 7.8 mmol/L (140 mg/dl) – so my blood sugar after supper was not only in the non-Diabetic range, it was much better than that!
This means that the delaying the time between meals that I have been doing each weekday is starting to have its effect.
‘Hearing’ for the first time
When insulin was released after I ate dinner last night, my cells responded to insulin’s signal and took up the glucose from my blood, into my cells! This is what is supposed to happen, but from years and years of eating a diet that had far to many carbs (mostly as “healthy” fruit and milk), my cells had become non-responsive to insulin’s signal. The glucose (the blood sugar produced after food is digested) would stay at high levels in my blood because even though sufficient insulin was being produced and released by the βeta-cells of my pancreas, my cells had become insensitive to its signal. My cells had become insulin resistant – they were ‘deaf’ to insulin’s signal.
Last night, for the first time that I’ve observed, my cells responded to insulin properly! Like a hearing-impaired person hearing for the first time, my cells could ‘hear’!
Still “hearing-impaired”
My cells aren’t yet ‘healed’. They and my liver are still insulin resistant which is evidenced by the fact that even though I haven’t eaten anything since dinner last night, my blood glucose is high.
As it is supposed to do in response to both a low-carb diet and intermittent fasting, my body is breaking down my fat stores for energy (lipolysis) and the free fatty acids that are released are being used to produce glucose for my blood (in a process called gluconeogenesis) and ketones for my other organs, including my brain.
My blood glucose should increase from the gluconeogenesis, but it shouldn’t stay high!
In a perfect world, my blood glucose should be maintained around 4.0 mmol/L (72 mg/dl) when I am intermittent fasting, but it is much higher than that. The VERY good news is, it is falling to these ideal levels earlier and earlier each day, as I continue to intermittently fast Monday to Friday.
Intermittent Fasting – the missing ‘key’
It used to be late in the afternoon before my blood glucose would finally fall to 3.9 – 4.2 mmol/L, but over the six days it has been falling to these levels earlier and earlier each day.
blood glucose readings July 25 – August 23, 2017
Last Thursday, while checking my blood glucose every 2 hours, it dropped to 3.2 mmol/L at 1:55 PM and I immediately ate some carb-containing food, but the next day, late in the afternoon it only reached 4.8 mmol/L at 4:00 PM, despite me delaying the time between meals, both days. As someone with Type 2 Diabetes, I have to monitor my blood sugars every few hours when I am delaying meals, to be sure my blood sugar is being maintained by my body breaking down fat.
Monday, my blood glucose was 3.7 mmol/L (67 mg/dl) at 4:00 PM and yes, I ate something immediately.
Tuesday it was 4.6 mmol/L (83 mg/dl) at 2:30 PM
Today (Wednesday) it was 4.5 mmol/L (81 mg/dl) at noon!
Best of all was that last night, 2 hours after eating, my blood glucose was only 5.8 mmol/L (105 mg/dl) – not just ‘normal’, but well below the non-Diabetic cutoffs! This is what I have been waiting for!
Tracking Ketosis
Ketones (also called ‘ketone bodies’) are naturally occurring molecules (acetoacetate, βeta-hydroxybutyrate, and their spontaneous breakdown product, acetone) that are produced for energy while people are sleeping, or when they haven’t eaten for a while. Ketone production is natural and normal and occurs to everyone – otherwise we would need to get up at night to eat!
Ketones are picked up the body’s tissues and converted into something called ‘acetyl-CoA’ which then enters the citric acid cycle and is burned in the cell’s mitochondria (the ‘powerhouse’ of each cell) for energy. When we are sleeping, or are eating low-carb high health fat or simply not eating for a while, this is what our body uses as fuel instead of glucose. When eating low carb over an extended period of time, the body makes the little bit of glucose it needs for our brain and blood from fat and uses ketones for the rest.
A Ketostix® urine test strip (from several weeks ago)
Ketones can be easily and inexpensively detected in urine using a test strip, such as Ketostix®.
When people are at a low level of ketosis, they produce both acetoacetate and βeta-hydroxybutyrate in approximately equal quantities. These ketones are used by the muscle cells for energy. Ketostix® only measures the amount of acetoacetate in the urine.
For those that choose to eat very low carb and remain in ketosis for a while, their body’s will take the acetoacetate and convert it to βeta-hydroxybutyrate. Since Ketostix® only measures acetoacetate, the strips may become lighter and lighter because there is less acetoacetate in then urine. This is when blood ketone strips becomes helpful.
Abbott Laboratories® produce a small serum monitoring system that can test either blood glucose levels or serum β-ketone levels, using different test strips. The glucose strips cost about the same as glucose test strips used with other glucometers, but the β-ketone test strips are quite costly, costing between $3-$5 each, depending on where they are purchased. I don’t use them very often – only to make sure I don’t let my ketones get too high.
Note: I take a rather conservative approach to low carb eating and don't see any need to lower carbs to such a point as people are producing large amounts of ketones. I encourage insulin-resistant clients who are eating low carb to monitor both their blood sugar and ketone production often and to discuss their results with their doctors.
The β-ketone test strips measure the amount of βeta-hydroxybutyrate in the blood.
β-Ketone test strip, measures βeta-hydroxybutyrate in blood sample
This morning, about an hour after I measured my fasting blood glucose at 7.8 mmol/L, I measured my fasting β-ketones (which measures the amount of βeta-hyroxybuterate in my blood) at 1.6 mmol/L.
A low level of serum βeta-hyroxybuterate is considered 0.34 mmol/L and a mid-range level of serum βeta-hyroxybuterate is considered 2.36 mmol/L, so I was in the low-mid range level, which is the highest level that I go. I am also monitoring my blood sugar every two hours to make sure that my blood sugar level is being maintained adequately.
Note: as they say on TV “don’t try this at home”. Be sure to discuss following a low carb diet with your doctor first and also discuss whether there are any health reasons to avoid remaining in mild ketosis for any period of time.
At these levels, my body is happily breaking down my own fat stores for energy and the free fatty acids that are being released are being used to produce glucose for my blood (via gluconeogenesis). This is evident by my blood glucose being 7.8 mmol/L around 9:30 AM today.
This morning’s workout ‘selfie’
My body produces ketones (as evident by my βeta-hyroxybuterate being 1.6 mmol/L) an hour later and these ketones are being picked up my body’s tissues and are being converted into acetyl-CoA, which is being burned by my cells mitochondria for energy. These ketones not only fuel my brain, so I can work, they also fuel my body so I can exercise.
Yes! I aim to do some kind of exercise for 30-45 minutes most days.
This is the BIG difference between “starving” and “fasting”. I’m fat-adapted and I have plenty of fat stores to burn, so my body is really quite happy burning my own fat stores for energy while maintaining my blood sugar using the carbs in my diet and the glucose synthesized from my fat.
‘Getting moving’ and occasionally ‘breaking a sweat’
When I speak of ‘exercise’, it’s not crazy intense, but it is my getting my body ‘moving’.
All my morning walks (with and without Nordic poles) – from the very first one 5 1/2 months ago, have been done fasting.
Yesterday I did 15 minutes of aerobic exercise and 30 minutes of lower body resistance training – not in a gym, but at home. I was fasting…and continued to fast until late in the afternoon. Remember, my body is breaking down my fat stores for energy and I have plenty of those!
all the “gym” I need!
I’m not a member of a gym.
I have a corner of one room set up with my Nordic Track ski-machine, a few free-weights (2#, 5#, 10# and for the future 20#), a floor mat, 3 levels of resistance bands, and a “step”.
If I use my Nordic Track, I listen to music while I work out, and have a water bottle with homemade club soda (seltzer) close at hand. I have a Sodastream® machine, so I always have a steady supply.
I am using the “step” or doing aerobics of some kind, I use some videos I found on You-Tube of a TV show I used to exercise to years ago. I always liked them because they gave lots of instructions so that only one muscle group at a time is being worked. That way, only one part of my body needs to recover, and I can work other parts the following day.
If I am doing my free weights, I follow the routine I learned from a kinesiologist friend, when I took off the first part of the weight 5 years ago.
I keep it simple and simply make part of every day doing something that requires me to ‘get moving’ and 3 times a week I aim to make that activity something that ‘breaks a sweat’.
I don’t exercise to ‘lose weight’ – I’m active because it’s part of a healthy lifestyle. It’s good for my heart, for reducing stress and to increase muscle tone – and it makes me feel terrific.
Sure, I still have a long way to go but a each week and each month passes, I am closer to my goal that I was the week or month before. I am certainly closer than had I never started!
Here’s some more proof…
These three photos were taken on this date (August 23) in 2015, shortly after I had heard about low carb high fat eating from a retired physician-friend, last year in 2016 and today 2017. While there isn’t a huge difference weight-wise between last year and this year (14 pounds), the difference one can’t see is becoming evident.
Me – August 23 2015, 2016 and today 2017
Yes, the progress it is painfully slow and it would be easy to get discouraged except that I have read the studies and seen the results that other clinicians have obtained with their patients. It’s twenty-five weeks since I started – just about 1/2 a year, but my hard work and determination to ‘stick with it’ is paying off. Last night, for the first time since I was diagnosed as having Type 2 Diabetes, my cells provided evidence that they are beginning to respond to the signals from insulin the way they are supposed to.
This afternoon, they did it all again!
This was my blood glucose 3 hours after lunch (which I decided to eat today, because I felt hungry). As mentioned above, 4.5 mmol/L (81 mg/dl) is well below the ‘normal’, non-Diabetic post prandial glucose level of 7.8 mmol/L (140 mg/dl)
This was even better than after dinner, yesterday!
It took longer than I expect, but it’s happening!
So, one day at a time, one week at time, the weeks add up to months and the months to half a year and in half a year, I have measurable progress!
Oh, did I forget to mention that my weight is down again? I am seeing “numbers” I haven’t seen since I gave birth to my children!
Slow, yes – but very sure.
Now let’s see what I’ll accomplish in the second half of this year!
Have questions?
Want to know how I can help you accomplish your health goals? Why not send me a note using the “Contact Us” form above.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
INTRODUCTION: This recent Canadian study reports that the caffeine contained in 1 1/2 to 3 cups of unsweetened coffee is sufficient to increase plasma levels of ketones, including β-hydroxybuterate, for several hours.
A pilot Canadian study conducted at the Université de Sherbrooke in Sherbrooke, Quebec and published in the Canadian Journal of Physiology and Pharmacology on November 25, 2016 evaluated the effect of caffeine on the production of ketones in healthy adults. Researchers were interested in caffeine as a ketogenic agent based on its ability to increase lypolysis (the breaking down of fat for fuel).
Method of the Study
Two different doses of caffeine were administered to 10 healthy adults who had fasted for 12 hours and who then ate a breakfast that containing 85 gm carbohydrate, 9.5 gm fat and 14 gm of protein.
Subjects were either given;
(1) no caffeine
(2) a cup and a half of regular drip coffee
(3) three cups of regular drip coffee
The subjects plasma caffeine levels were measured over the next 4 hours and it was found that those that drank 1 1/2 cups of coffee had~ 2.5 mg caffeine per kilogram of body weight and those that drank 3 cups of coffee had ~ 5.0 mg caffeine per kilogram of body weight.
Plasma caffeine over time
Results – the effect of caffeine on ketone production
Subjects that had 1 1/2 cups of coffee (2.5 mg of caffeine per kilogram) had 88% higher ketone production than subjects that had no caffeine.
Subjects that drank 3 cups of coffee (5.0 mg caffeine per kilogram of body weight) had 116% higher ketone production over subjects that had no caffeine.
β-hydroxybuterate per hour
Expressed as the amount of β-hydroxybuterate in μmol/L, it is evident that this ketone rises significantly in response to caffeine, and rises in a dose-dependent manner. That is, the more caffeine consumed the more β-hydroxybuterate was produced.
Amount of β-hydroxybuterate produced in response to caffeine dose
Researchers reported that the level of ketones found in the blood after 3 cups of coffee was approximately twice that produced after an overnight fast.
This increase in plasma ketones obtained with these doses of caffeine could, at least in the short term (a few hours) contribute to ~5-6% of brain energy needs.
Mechanism
The increase in free fatty acids as well as β-hydroxybuterate is explained by caffeine blocking phosphodiesterase (PDE), preventing the inactivation of cyclic adenosine monophosphate (cAMP) – with increased caffeine leading to higher levels of cAMP.
Cyclic adenosine monophosphate (cAMP) is a cellular messenger that is involved with transferring hormones such as glucogon, which is the main catabolic hormone of the body and which functions to raise both the concentration of glucose and fat in the bloodstream and has the opposite effect of insulin).
Glucagon needs cAMP in order to pass through the plasma membrane, so as a result cAMP serves to regulate glucose, fats and glycogen.
cAMP activates hormone sensitive lipase, an enzyme which breaks down fat (lypolysis). This increased breaking down of fat, increases free fatty acids (FFAs), which can then be converted in the liver to the ketones acetoacetate and β-hydroxybuterate.
Final Thoughts…
While this is a small study, the data supports that a few cups of regular, unsweetened coffee (without any butter or coconut oil added) increases the amount of ketones produced for several hours.
If you are following a low carb diet and are monitoring your blood or urine ketones, be aware that having coffee can increase the amount of ketones your body is producing.
Vandenberghe C, St-Pierre V, Courchesne-Loye A, et al, Caffeine intake increases plasma ketones: an acute metabolic study in humans, Canadian Journal of Physiology and Pharmacology,2017, Vol. 95, No. 4 : pp. 455-458
Dr. David Perlmutter, MD (www.drperlmutter.com/caffeine-ketosis-friend-or-foe)
Note: Everyone’s results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody’s nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
When people think of “fasting” what comes to mind is an almost-intolerable short period of time without food, and with nothing to drink (except maybe water) and where people usually spend most of the time counting until they can eat again. This is the case when we are used to burning carbs as our fuel source and then just stop eating. Our body slows its metabolism in response to the severe calorie restriction in an effort to spare energy. We feel cold, tired, lethargic and we find it difficult to concentrate because our body is in starvation mode.
When we are fat-adapted, we use the fat in our diet (dietary fat) and our own fat stores (endogenous fat) as our fuel source. When we “fast”, we stop supplying our body with dietary fat, so our body relies solely on our fat stores to supply its energy needs. Most of us who are following a low carb high fat diet have plenty of endogenous fat, so when we aren’t eating, we don’t feel hungry, tired or cold because our body has a plentiful source of energy! Our basal metabolism doesn’t drop. Rather than feeling cold and tired and finding it difficult to think, we are able to think clearly using ketones produced from fat to fuel our body, rather than glucose.
“Intermittent fasting” is simply increasing the amount of time between meals. Fasting is not eating or rather, not eating now. It’s different than “starving” because our basal metabolic rate is being maintained through our fat stores. When we are in starvation mode, our basal metabolism drops significantly in order to spare energy – that’s why we feel cold and tired, because our body is saving calories for our brain and our heart to function. Fasting also doesn’t mean that we can’t consume anything! There are plenty of things we can have during the delay before our next meal. The most natural “intermittent fast” is the one between after supper and breakfast the next morning. Yes, that is why it is called “breakfast”.
Why Fast?
When we eat, insulin is released in response to the presence of carbs in the food we eat and functions to (a) move glucose out of the blood and to (b) store the glucose that is not immediately needed for energy, as fat.
When we are accustomed (as most of us have been) to eating three meals a day plus having a couple of snacks, insulin is released every few hours. If we have been “grazing”, we have been constantly releasing insulin. As a result of this, our cells have become insensitive to insulin – something known as “insulin resistance“, or insulin tolerant. To conceptualize this, think of going into a room with loud music. At first your ears buzz and your auditory system is overwhelmed, but after a bit of time, your body adapts. It’s similar with smell. When you’re exposed to a pungent odor, at first that’s all your can concentrate on, but after time passes, your brain starts to “tune out” the signals from your nose and you become less aware of the smell. It’s not that the odor decreases, but our response to the odor, decreases as we become “tolerant” to that molecule bound to our olfactory receptors.
The difference with “insulin resistance” is that it is more than our body becoming “tolerant” of the circulating insulin, it actually responds less to it.
Think of someone that drinks considerable amounts of alcohol. They can have 3 or 4 drinks and not feel intoxicated, because they have a “high tolerance” to the ethanol in the drink. It takes more and more alcohol for them to respond. When someone is “insulin tolerant” (also called “insulin resistant”), the same amount of insulin has less and less effect, so to adapt, to be able to move the glucose out of the blood and store the excess energy as fat, the body needs to release more and more insulin. From years and years of eating 3 carb-based meals plus a couple of carb-laden snacks each day, our insulin levels simply don’t fall to baseline.
When someone is not insulin resistant, delaying the time before the next meal enables their insulin levels to fall to baseline (10-30 pMol) in approximately 12 hours, so if they don’t eat anything after dinner and their first meal of the day is breakfast the next morning, that time period is usually close to 12 hours. However, for people who are insulin resistant, a longer time period is often needed for their insulin levels to fall to baseline. Just as insulin resistance developed over time, gradually, a new lower baseline can be set over time by increasing the length of time that one intermittently fasts.
Twelve-Hour Fast
A twelve-hour fast is the easiest one for most people to do, because during most of it, they’re asleep!
This is the one I suggest to my clients once they’re fat-adapted (usually after ~4 weeks of eating low carb high fat) as all it entails is not eating anything after supper until breakfast the next morning.
That’s it.
So, say they finish dinner at 6:30 PM, then the next time they eat is breakfast the next morning at 6:30 AM. This simple, short 12-hour “fast” is just enough to enable their insulin to fall to baseline. Doing this often, if not daily is the goal. This is entirely do-able and an important first step in restoring insulin sensitivity and it is certainly not something “radical”. Years ago, people didn’t eat after supper!
People who have Type 2 Diabetes should check with their doctor before beginning doing any form of Intermittent Fasting – and definitely should do so if they are on any kind of medication to manage their blood sugar, blood pressure or cholesterol, without having their doctors oversee it. Medication will often need to be adjusted downward (and sometimes eventually discontinued entirely) as insulin sensitivity returns, so don’t do this without involving your doctor, first!
Eighteen Hour Fast
Once people have become used to not eating from supper until breakfast, they may want to wait to eat their first meal until noon the next day, especially if they don’t feel particularly hungry in the morning. Some people are not “breakfast” people and if they eat well the night before, they may not want to eat in the morning. An eighteen hour “fast” is from after someone has finished dinner (say, at 6:00 PM) until noon the next day.
Many do want their cup of coffee, which is totally fine provided it is unsweetened. I don’t recommend that people use sugar substitutes, especially the sugar alcohols such as sorbitol, mannitol or xylitol which have the same number of carbs per teaspoon as ordinary table sugar.
Cappuccino foamed with 1/2 oz of cream diluted with 1 oz of cold, filtered water
Cream can certainly be added to drip coffee and there’s no need to give up your morning latte or cappuccino – just a little creativity to replace the milk (which has almost as many carbs per cup as a slice of bread!).
My trick is to foam 1/2 an ounce of cream with an ounce or ounce and a half of cold, filtered water.
This makes fasting until lunch entirely possible!!
Twenty-four Hour Fast
Note: I don’t do these and I don’t recommend that my clients do these unless they are being very closely monitored by their doctor, however I want to describe them, so people know what they are.
A twenty-four hour “fast” is from the end of supper one day, until the start of supper the following day (technically it is a 23-hour fast unless you add the extra hour ). As with the eighteen-hour fast, one can have unsweetened coffee or tea with a drop of cream, club soda (seltzer) with a twist of lime or lemon, or “bone broth”. “Bone broth” can be made from any kind of meat, fish or poultry bones, but for me, when I think of “bone broth”, I think of a wonderful, rich broth made from beef marrow bones, that is gently simmered overnight on the stove, ready to be sipped as desired, on a fast day.
To avoid getting constipated, many people will take psillium fiber with water each morning and which can be added to cups of “bone broth” or dissolved in a little bit of diluted coconut milk.
Ingredients for “bone broth” – beef marrow bones, ox feet, onion, garlic and fresh peppercorns
cup of beef “bone broth” – made from ingredients above
What’s not to love about sipping this when “fasting”?
The main purpose of delaying the time between meals (“intermittent fasting”) is to restore insulin sensitivity. When we aren’t eating, we aren’t releasing insulin – and as we continue eating low carb high fat and delaying the time between meals, our insulin receptors become sensitive to insulin once again.
Normalized blood sugar levels (both fasting blood glucose and HbA1C) is a natural byproduct, not the goal. The goal is releasing less and less insulin in response to the food we eat and our body’s sensitivity to the insulin that we do release, being restored.
Weight loss is another added benefit!
Have questions about how I can help you? Please send me a note using the “Contact Us” form on the tab above.
Note: Everyone’s results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody’s nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
For the last 2 weeks, the Lower Mainland has been covered in smoke due to hundreds of wildfires in the area. The very poor air quality had made going for a walk impossible.
Everywhere I went, I needed to wear an N95 mask to filter out the particulate matter and with the excessive heat and reddish-yellow skies, I had no desire to be out any longer than I needed to.
Over the weekend, cool marine finally air arrived and the air cleared for the first time in weeks. Finally it didn’t look like I was living on Tatooine.
When I woke up yesterday, the first thing I wanted to do was go for a morning walk. I walked 3 km around the local track and today I went again and decided to make a short video. When I went to upload it, I noticed how very different my face looked than from my first walk, 5 months ago (March 16 2017).
LEFT: March 16, 2017 | RIGHT: August 15 2017
I’ve only lost 13 pounds in the last 5 months since I began eating Low Carb High Healthy Fat, but the difference in how I look and how I feel is quite evident. As I’ve covered in previous “A Dietitian’s Journey” blogs, my blood work has certainly reflected the change.
I don’t really do any exercise outside of walking and even then, I only started doing it regularly 7 weeks ago (June 22, 2017) and not for the last 2 weeks (due to the air quality advisory). Five weeks of walking has helped me tone my muscles a bit and lower my overall blood sugar, but not had any significant impact my weight loss. While for the last 8 weeks, I’ve delayed the start of my first meal (intermittent fasting) which has impacted my fasting blood sugar, it hasn’t really impacted my weight, as I consume the same amount of protein, fat and carbs per day, just over a shorter period.
My weight loss has really only been accomplished by doing what I have been teaching my professional clients to do over the last 2 years; eating low carb and high healthy fat. I was tired of being the “fat Dietitian”! Now I’m now “practicing what I preach”.
Is it hard? Not at all! This has to be the easiest way to eat and requires little, if no culinary skill. Sure, one can get pretty creative making all kinds of exciting ethnic foods if they know how to cook, but it is certainly not required!
The difference in how I feel is truly all the motivation to keep doing it! Losing weight is a bonus.
Want to know how I can help you achieve your own health and nutrition goals? Why not send me a note using the “Contact Us” form above.
Note: I am a "sample-set of 1" - meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating "low carb" and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
For the last two weeks, I have been living on Tatooine. Not really, but it certainly has felt like that – with smoky, red sunrises and sunsets, inhospitable heat and high levels of ground-level ozone. British Columbia, where I live, remains under a state of emergency as 148 wildfires continue to burn across the province, with this being BC’s worst fire season in almost sixty years. As a result, the air quality in many communities, including mine, has deteriorated to dangerous levels.
This is what the sunrise has looked like from my backyard the last two weeks:
There have been high concentrations of fine particulate matter known as PM2.5 in the air, which are solid or liquid droplets with a diameter of ≤2.5µm (micrometres). Due to their small size, these particles easily penetrate indoors, even when windows are closed and are small enough to pass from the lungs into thebloodstream –putting people withlung or heart disease, Diabetes or asthma at risk.
In addition to the smoky air, temperatures each day have been in the low- to mid-thirties Celcius (90-95 degrees Fahrenheit) which is highly unusual. Here in the Greater Vancouver area, we’ll get a few days in a row like that once or twice each summer, but not for two weeks solid! Thankfully I have air conditioning, but it has been brutal to be outdoors.
Concentrations of ground-level ozone have reached and stayed at advisory levels. This is formed when pollutants given off by the forest fires and compounds from the solvents used to put out the fires react in the air, in the presence of sunlight.
Even wearing an N95 mask outside which is designed to filter out the small smoke particles, I have found my breathing very laboured.
Needless to say, my morning and after-dinner walks have been impossible. I tried exercising indoors, but my lungs were simply too irritated from the small smoke particles.
I have continued with delaying the time between meals (referred to as “intermittent fasting”)but for shorter periods of time as my body is under physiological stress and I continue to eat a low carb high fat diet. My weight has dropped another pound over these last two weeks, despite no exercise at all. My blood sugar on the other hand is considerably higher without the walks.
An air quality analyst with Metro Vancouver has reported that the weather is expected to shift this coming weekend, allowing some of the smoke to begin to dissipate. Until then, part of taking care of my health is not to exercise.
Reporting from Tatooine, British Columbia, I’m Joy Kiddie, practicing what I preach.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This recipe is posted as a courtesy to those following a variety of low-carb and ketogenic diets (not necessarily Meal Plans designed by me). This recipe may or may not be appropriate for you.
I have been asked so many times for this recipe, that I’ve decided to post it and while this isn’t everyday fare for me, one of my sons would eat it as often as I would make it. There is a local fish and chips place right on the Pacific Ocean and I’ve been told this easily rivals theirs.
Have a look:
Low Carb Beer Batter Fish
The batter is light and crispy – like the best tempura batter.
In fact, when I make fish this way, I dip slices of zucchini in the leftover batter, and make a deep fried side to go with it. I mean, why not? Once you’re frying, might as well, right?
This is definitely not “everyday food” but “sometimes food”, but oh, is it good!
Low Carb Beer Batter Fish and Zucchini
I fry in cold-expressed virgin coconut oil, as it has a high smoke point and unlike commercial refined seed oils like grapeseed, soybean, sunflower, safflower and corn oil, cold-expressed virgin coconut oil doesn’t produce Advanced Glycation End-Products (AGEs), which can cause oxidative damage to cells in the body.
I heat the coconut oil to between 160-170 °C or 320-340 °F, which is hot enough that a piece of batter dipped vegetable begins to puff and get golden quickly, but still allows some frying time for the internal parts to be fully cooked.
My favorite fish to fry this way is fresh Pacific Cod loins, but even defrosted Haddock Loins come out pretty good, if defrosted in the fridge until ~80% thawed, then pressed dry with a paper towel prior to dipping in batter, to get the excess water out.
Okay, enough background…here’s the recipe.
Low Carb Fish and Vegetable Beer Batter
11 Tbsp unflavoured Whey Protein Isolate powder
1 1/2 tsp baking powder
1 tsp baking soda
1 tsp pink Himalayan salt, ground
1 tsp guar gum (or xanthan gum)
3 eggs, large, free-range, beaten well
3 Tbsp low carb beer (such as Sleeman Clear 2.0) or sparkling water (Club Soda, Seltzer)
Cooking Instructions
Slice 6 cod or haddock loins in half and pat dry well with a paper towel.
Cut one or two firm slender zucchini into 1/8″ (1/3 cm) slices.
Heat the coconut oil in a heavy pot until between 320-340 °F. (160-170 °C). Make sure there it is deep enough that the thickest piece of battered fish can float.
Mix all the batter ingredients together in a wide, shallow bowl and whisk well for a minute or two, to make sure there are no lumps. (You can’t toughen the batter, as there is no gluten!) The batter should be a light creamy yellow.
When the coconut oil is hot enough, dip your zucchini (and/or other vegetables) and fry first on one side and then the other and set aside on a plate lined with several paper lunch bags, to absorb the excess fat. Don’t over cook. Be sure to whisk your batter back together for 20 seconds or so before dipping the fish to ensure the perfect consistency.
Dip your dried, cut fish loins in the batter and coat well on both sides, and fry in the coconut oil until the batter is golden brown on the first side. Flip each piece over gently and fry on the second side, until the fish is cooked in the middle and a golden and crisp.*Don’t overcrowd the pot, as it will cause the oil temperature to decrease to much, and your fish will be greasy. I fry two pieces at a time in a 10″ (25 cm) pot.
Transfer each piece to a plate lined with paper lunch bags, to absorb the excess oil.
Enjoy!
If you would like more information about the services I provide please have a look under the Services tab. If you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
It’s been 5 months since I began my own weight-loss journey, following a low carb high healthy fat diet and here is a short update.
Fasting Blood Glucose
When I began this journey at the beginning of March, my fasting blood glucose was averaging 12 mmol/L. Four months into eating low carb high fat, my fasting blood sugar was averaging 8.5 mmol/L.
July 25th, it was measured at the lab and on my home glucometer as 8.0 mmol/L – still way above the cutoffs for those with Type 2 Diabetes of 6.0 mmol/L, and way above the normal levels of 4.5-5.5 mmol/L.
It is highest is in the morning, I believe due to cortisol’s effect (see 4 month update, for details).
2 hour Post-Prandial Blood Glucose
I’ve been tracking my blood glucose regularly since I started implementing the dietary and lifestyle changes 5 months ago, and my 2 hr post prandial (after a meal) glucose had been averaging ~7.2 mmol/L, which is much better than the 7.7 – 8.6 mmol/L which is what it was at the beginning of March, but still no where good enough!
…but I noticed that after I go for my brisk 3-4 km each morning, it is 5.4 mmol/L. This gave me an idea (see below).
Blood Glucose through the night – effects of Cortisol
For about a week, I measured my blood glucose at 1 AM and 4 AM and 6 AM (in the interest of science, of course!) with a brand new glucometer that I standardized at the lab, when I had my fasting blood glucose and fasting insulin done on July 25th. My morning fasting blood glucose would rise to ~6.6 – 6.8 mmol/L (119 – 123 mg/dl) from the 5.4 mmol/L it was when I went to bed, even though I hadn’t eating or had anything to drink. This had to be the effect of cortisol!
Fasting Cortisol
I had my fasting cortisol assessed the same day that I had my fasting blood glucose assessed (July 25 2017) and it was, as I suspected, high: 421 (125-536) nmol/L
…and this is with walking 4 km / day and sleeping 8 hours (restful sleep).
I need to come up with some additional strategies for lowering stress.
Fasting Insulin & Calculating Insulin Resistance
I also had my fasting insulin assessed the same day that I had my fasting blood glucose and fasting cortisol assessed (July 25 2017).
Based on the July 25th lab work, I calculated my Insulin Resistance using both Matthews (1985) Equations (HOMA1-IR), as well as using Oxford University Center for Diabetes, Endocrinology and Metabolism homeostasis model assessment (HOMA2-IR) calculator (2013).
From when my fasting insulin and fasting blood glucose was last tested 2 years ago in August 10, 2015, my insulin resistance calculated by HOMA2-IR had gone down from 3.06 to 2.77, but it’s still too high because my fasting blood glucose remains high.
Average Insulin Resistance – in the normal population
One study reported that the average HOMA2-IR in the general (non-Diabetic) population is 2.1 +/- 2.2 (Diabetes Care, Volume 24, Number 3, March 2001), so I am guessing that a HOMA2-IR of 1.00 would be a healthy target – one that will likely take me a year to approximate.
Whether that will be possible with diet and lifestyle change alone, has yet to be seen.
That is my goal.
High Morning Glucose – assessing the problem
I believe the reason that my blood glucose remains high in the morning is due to a combination of residual hepatic (liver) insulin resistance (from years of eating way too many carbs) and high cortisol that is stimulating an overproduction of waking glucose.
Effect of Walking
The last 5 months, my fasting blood glucose has been consistently high at 8.0 – 8.5 mmol/L (144 – 153 mg/dl) and my 2 hour postprandial is fine for a Type 2 Diabetic at ~7.2 mmol/L – but a far cry from the non-Diabetic range I am seeking.
…but I noticed that after I go for my brisk 3-4 km walk each morning, my fasting blood glucose is 5.4 mmol/L (yes, I go fasting).
The effect of moderate exercise seems substantial, so I decided to see what effect there would be on my early morning fasting blood glucose levels if if I took a short walk after dinner.
The results were dramatic!
For the last week and a half, my blood glucose drops to ~5.2 – 5.4 mmol/L (94-97 mg/dl) after a very leisurely 15-20 minute walk around my neighbourhood.
High Morning Glucose – assessing the solution
Based on my high fasting blood glucose of 8.0 mmol/L on July 25th, my physician’s colleague naturally recommended that I go on Metformin, but I have decided to hold off on introducing it for 3 months provided that;
(1) I continue the dietary and lifestyle changes I have been doing for the last 5 months and…
(2) I add a 20-minute walk after dinner.
Plan to Reassess in Three Months
I am requesting that my physician provide me with a requisition to have my fasting insulin and FBG re-run in October, when I update my HbA1c, so I can recalculate my HOMA2-IR again and see how much less insulin resistant I am by then.
I want to know the magnitude of the insulin levels dropping, not just the fasting blood glucose, which I expect, will drop…after all, the goal is to lower the very high levels of insulin. High blood glucose is a symptom – the cause is too much insulin being released, due to insulin resistance.
Blood Pressure
As mentioned previously, I asked to be started on a very low dose of Ramipril (Altace) about 6 weeks ago, as my blood pressure had begun to creep up again. When I saw 160/90 mmHg two days in a row, I went to see my doctor.
10% of the time I am ≤ 119 / 79 mmHg, considered normal blood pressure
64% of the time I am ≤ 120/80 mmHg, categorized as “Prehypertension”.
…and 26% of the time, measured before I take my medication, I am ≤ 138/90 mmHg, categorized as “Stage 1 Hypertension”.
I will continue to take the blood pressure medication as a temporary measure to offer some protection against heart attack, stroke and kidney damage until I lose some more weight, and my blood pressure stays down on its own.
Weight
Overall, in the last 5 months, I have lost 12 pounds and ~3 inches off my waist. I’ve lost about the same number of inches off my neck circumference (3 inches) which has had a dramatic effect on how I look. I have a neck and ONE chin.
I’ve lost overall about an inch off my mid-arm, an inch off on my thighs (gaining muscle and losing fat, at the same time) and lost around an inch off my chest.
Lowering Stress, Lowering Insulin
I need to get my cortisol levels down, as these are driving my high morning fasting blood glucose levels. Walking in the morning has been good, adding the short evening walk even better. Now I am adding (on alternate days from my 3-4 km walks) a workout with 5 and 10 pound weights and other forms of resistance training. I am even jumping rope (which has gotten much harder since when I last did it at around age 16!).
The goal is to get my insulin levels down, and I am already doing everything that needs to happen for that; eating only the carbs necessary to have a nutritious diet, with no excess protein and extending the time between meals (intermittent fasting) a few days per week.
It is going to take time…
Over the next 3-6 months, I expect fasting insulin will keep falling.
My goal over the next year is to reach a ‘normal’ 2 hour postprandial peak of 60 mIU/L (430.5 pmol/L) as determined by Dr. Kraft’s Insulin Response curves, which should be an Insulin Resistance (HOMA2-IR) of between 1.0 and 2.0.
Over time, the fat in my liver (“hepatic adiposity”) will continue to decrease, and the derangement which took time to develop will resolve.
While the rate of resolution to for me to achieve normal insulin metabolism is unknown, I know if I keep doing what I am doing, it should happen. It doesn’t always occur, but I won’t know if I don’t try.
Have questions?
Want to know how I can help you achieve your health and weight goals? Why not send me a note using the “Contact Us” form, above.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Changing how and what we eat, as well as managing stress and getting enough restful sleep has been shown in research studies to reduce pain and symptoms in people with chronic inflammatory diseases such as Rheumatoid Arthritis, Fibromyalgia, Hashimoto’s Hypothyroidism, Celiac disease, etc.. As well, there is increasing evidence that cardiovascular disease, including heart attack and stroke are inflammatory in nature and that lowering risk is best managed through dietary and lifestyle changes. For those with a strong family history of heart disease, the Anti-Inflammatory Protocol dove-tails perfectly with a low-carb high healthy fat diet.
Knowing which foods promote inflammation and why and which foods are evidence-based to have anti-inflammatory properties and why is essential for those seeking to reduce pain and symptoms associated with a chronic inflammatory condition. Choosing foods that are nutrient dense, promote gut health, address diet-related disruptions in hormone-regulation and that target immune system regulation are key in the Anti-Inflammatory Protocol.
Nutrient density — Every system in the body, including the immune system requires an array of vitamins, minerals, antioxidants, essential fatty acids, and amino acids to function normally. Micronutrient deficiencies and imbalances are considered key players in the development and progression of autoimmune disease, therefor attention is put on consuming the most nutrient-dense foods available. A nutrient-dense diet provides the building blocks’ that the body needs to heal damaged tissues. The goal is to supply the body with a surplus of micronutrients to correct both deficiencies and imbalances, supporting regulation of the immune system, hormone and neurotransmitter production.
Gut health — It is thought that gut dysbiosis’ (gut microbial imbalance) and leaky gut’ may be key facilitators in the development of autoimmune disease. The foods recommended on the Anti-inflammatory Protocol support the growth of healthy levels and a healthy variety of gut microorganisms. Foods that irritate or damage the lining of the gut are avoided, while foods that help restore gut barrier function and promote healing are encouraged.
Diet-related Disruptions in hormone regulation – What we eat, when we eat, and how much we eat affects a variety of hormones that interact with the immune system. Eating foods with too much sugar or grazing’ throughout the day, rather than eating food at set meals spaced apart deregulate these hormones. As a result, the immune system is typically stimulated. Promoting regulation of these hormones through diet, in turn has a modulating effect on the immune system. As well, dietary hormones that impact the immune system are also profoundly affected by how much sleep we get, how much and what kinds of activity we do, and how well we reduce and manage stress, so looking at diet and lifestyle together, is key.
Immune system regulation — Our intestines are home to millions of bacteria which live in symbiotic relationship with us. We provide food for them and when in balance, they maintain the integrity of the gut wall, which serves as a protective barrier. When our gut ‘flora’ gets out of balance, having an excess of pathogenic bacteria, this protective barrier becomes compromised, resulting in small ‘holes’ that permit exchange between the inside of our gut and the blood stream. This is what is called “leaky gut“. Endotoxins produced by the proliferation of “bad” bacteria can get into the blood stream, stimulating the immune system, and resulting in systemic inflammation. What becomes critical is to limit the factors that contribute to excess of the “bad bacteria” and restore a healthy amount and diversity of ”good” gut microorganisms, so that the gut once again functions as a protective barrier, and immune system regulation is achieved.
What is the Anti-Inflammatory Protocol?
The Anti-Inflammatory Protocol identifies foods that promote inflammation from those that research indicates have anti-inflammatory properties. It isn’t simply a list of “eat this” and “don’t eat that”, but explains what about a particular food promotes inflammation or inhibits it. It explains the role of key inflammatory -producing compounds such as lectins, saponins and protease inhibitors, and which foods they are found in, and how eating those foods contribute to “leaky gut”. Which grains can one eat? Which should be avoided? What about beans and lentils? Are there some better than others?
The Anti-Inflammatory Protocol explains which healthy cooking and eating fats won’t contribute to the production of Advanced Glycation End-Products (AGEs) – and how this compound causes oxidative damage to the cells in the body. Knowing this enables people to know whether oils such as grapeseed for example, are a good choice and if not, why – as well as which other oils would be preferable.
I want people to understand in simple terms how omega 6 (ρ‰-6) fats compete for binding sites and elongation enzymes with omega 3 (ρ‰-3) fats, as this enables them to determine whether foods such as nuts and seeds should be included in an anti-inflammatory diet. If they understand the role of hormones such as insulin and what causes it’s release, they can determine for themselves whether products like agave syrup or coconut sugar are preferable to table sugar when following an anti-inflammatory protocol. I find that once people understand the theory as to why they should eat less of certain foods (explained in ways that don’t require an educational background in science!) and they also understand which types of foods they should aim to eat more of, they are empowered to make dietary choices that contribute to reducing inflammation, as well as symptoms, along with risk factors for other inflammation-related conditions.
I consider my primary role is as an educator. I don’t want to tell someone they need to eat this food on this day and this other food on the next day. It is far more rewarding and helpful to them, if I help them know how to make these decisions themselves.
Want to know more? Why not send me a note using the “Contact Us” form above.
Note: Everyone’s results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody’s nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
INTRO: There are a number of tools available for measuring insulin resistance, most of which are more suited to a research setting, including the Quantitative Insulin Sensitivity Check Index (QUICKI) and the Matsuda Index. Others, such as the McAuley -, Belfiore -, Cederholm -, Avignon – and Stumvoll Index are better suited for epidemiological (population) research studies and are often compared to the ”gold standard” for the measurement of insulin sensitivity, the Hyperinsulinemic Euglycemic Clamp (HEC).
The homeostasis model assessment (HOMA-IR) method is suitable for individuals to use with their doctors or Dietitians to assess insulin resistance, and is useful for using over time to measure the impact of dietary and lifestyle changes in lowering insulin resistance.
Visualizing Insulin Resistance
Insulin resistance can be determined by measuring insulin response to a standard glucose load over a 5 hour period and plotting the Insulin Response curves – which is precisely what Dr. Joseph R. Kraft MD, who was Chairman of the Department of Clinical Pathology and Nuclear Medicine, St. Joseph Hospital, Chicago, until his retirement.
Dr. Kraft spent more than a quarter century devoted to the study of glucose metabolism and blood insulin levels – collecting data in almost 15,000 people, aged 3 to 90 years old. Between 1972 and 1998, Dr. Kraft measured the Insulin Response and data from 10,829 of these subjects indicated that 75% of subjects were insulin resistant.
Compiling this data, five distinct Insulin Response Patterns emerged.
Pattern I
The light green curve below, is what a normal insulin response should look like. Insulin levels should rise steadily in the first 45 minutes (in response to the standard glucose load) to no higher than ~60 mIU/L (430.5 pmol/L) and then decrease steadily until baseline by 3 hours.
PATTERN II
People who are in the early stages of insulin resistance (Pattern II, represented by the yellow curve) release considerably more insulin in response to the exact same glucose load. Insulin levels rise to ~ 115 mIU/L (825 pmol/L) in the first hour and then take considerably longer (5 hrs) to drop back down to baseline, than the normal response.
PATTERN III
People who have progressed in insulin resistance to Pattern III have insulin levels that keep rising for the first 2 hours and then drop off more sharply, back down to baseline.
PATTERN IV
Those with Type 2 Diabetes / very high insulin resistance (Pattern IV) release huge amounts of insulin almost immediately, reaching levels of ~ 150 mIU/L (1076 pmol/L) at 1 hour. Then for the next 2 hours, insulin continues to climb, before it begins to decline to baseline. Even at 5 hours, insulin levels never decrease to normal values.
PATTERN V
Is what is seen in Type I Diabetes (T1D), when there is insufficient insulin production.
While a 5 hour glucose tolerance test is not available at most labs, a 2 hour glucose tolerance test (2hrGTT) will indicate whether or not a person is insulin resistant or Type 2 Diabetic.
However, once a person is already diagnosed as Type 2 Diabetic, most medical plans will not cover the cost of having the test re-performed in order to determine if insulin response has changed in response to diet and lifestyle changes.
This is where the the homeostasis model assessment of insulin resistance (HOMA-IR) comes in – a tool easily used by clinicians and relying on standard blood tests.
Homeostasis model assessment of insulin resistance (HOMA1-IR) – Matthew’s Equations (1985)
The homeostasis model assessment was first developed in 1985 by David Matthews et al and is method used which quantifies insulin resistance and β-cell function of the pancreas from fasting blood glucose and either fasting insulin or C-peptide concentrations.
Pancreatic β-cells are responsible for insulin secretion in response to increasing glucose concentrations, so when there is decreased function of the pancreas’ β-cells, there will be a reduced response of β-cell to glucose-stimulated insulin secretion.
In addition, glucose concentrations are regulated by insulin-mediated glucose production in the liver, so insulin resistance is reflected by reduced suppression of hepatic glucose production, stemming from the effect of insulin.
The HOMA-IR model describes this glucose-insulin homeostasis using a simple equation, based on fasting blood glucose and fasting insulin. The equation uses the product of fasting plasma insulin (FPI) x fasting plasma glucose (FPI), divided by a constant of 22.5, providing an index of hepatic insulin resistance:
HOMA1-IR = FPI (mu/I) x FBG (mmol/L) / 22.5
The “Blood Code” book is based on these 1985 equations. The problem with the Matthew’s Equations is that they underestimate Insulin Sensitivity (%S) and overestimate % β-cell function.
Homeostasis model assessment of insulin resistance (HOMA2-IR)
Oxford University, Centre for Diabetes, Endocrinology and Metabolism in the UK, has designed a HOMA2-IR model (2013) that estimates β-cell function (%B) and insulin sensitivity (%S) for an individual from simultaneously measured fasting plasma glucose (FPG) and fasting plasma insulin (FPI) values. It also can be used with fasting specific insulin or C-peptide values, instead of fasting RIA insulin.
It is important to note that HOMA-IR values vary by ethnic group, but looking at humans as one, a normal HOMA-IR value for a healthy person ranges from 0.5-1.4
Less than 1.0 means you are insulin-sensitive which is optimal.
While these tools are primarily used by clinicians, knowing about them is useful in being proactive in managing one’s own health. For example, if you have already started making the dietary and lifestyle changes to lower insulin resistance, having your fasting insulin measured along with your fasting blood glucose, will enable your doctor or myself to calculate your progress, as well as recommend adjustments in your plan.
Have questions?
Why not send me a note using the “Contact Us” form at the top of this web page.
Note: Everyone's results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody's nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
The hormone insulin plays a number of roles, one of which is to help move the glucose that is produced from the digestion of food – from the blood and into the cells for energy. Insulin resistance is where the body isn’t responding to insulin’s signals to take up glucose, so blood glucose remains high, despite normal or high levels of insulin.
Type 2 Diabetes (T2D) is essentially a state of very high insulin resistance.
Insulin normally goes up when we eat foods that contain carbohydrate (breads, pasta, rice, fruit, milk products, etc.) and acts on the liver to help store the incoming food energy – first as glycogen and when liver and muscle glycogen stores are “full”, it acts to store the excess energy as fat (de novo lipogenesis).
When we haven’t eaten for a while or are sleeping, the hormone glucagon acts to break down the glycogen in our muscles and liver (glycogenolysis) in order to supply our brain and cells with glucose. Insulin acts to inhibit glucagon’s action, which signals the body to stop making new glucose from its glycogen stores. When our glycogen stores run out (such as when we are fasting), the body turns to non-carbohydrate sources such as fat to make the glucose it needs for essential functions (gluconeogenesis).
When we are insulin resistant, insulin continues to act on the liver to signal it to store energy. When glycogen stores are “full”, it stores the excess energy as fat. When fat stores are “full”, the body starts storing the excess fat that the liver keeps making, inside the liver itself. There shouldn’t be fat in the liver, but when we are insulin resistant, such as in Type 2 Diabetes excess fat gets stored in the liver in a condition known as “fatty liver disease”.
In insulin resistance, the liver becomes more sensitive to insulin’s signal to make fat (and as a result keeps making more and more fat) yet at the same time, the liver becomes less sensitive to insulin’s inhibition of glucagon – resulting in more and more glucose being produced and released in the blood.
High levels of glucose remain in the blood despite adequate insulin, and it is this high level of blood glucose that is the hallmark symptom of Type 2 Diabetes. For the same quantity of insulin released, the body moves less and less glucose into the cell.
What does the body do to compensate? It makes more insulin!
KEY POINT: Insulin resistance results in the increased production of insulin. Increasing blood sugar CAN a symptom, caused by the insulin resistance, but blood glucose can be normal and one can still be insulin resistant (see Featured Article on Insulin Resistance).
When we are insulin resistant and keep eating a carb-based diet, the body requires more and more insulin in order to move the same amount of glucose into the cell.
The main issue then becomes too much insulin (hyperinsulinemia).
Defining the Problem Defines the Treatment
In Type 2 Diabetes (which is in essence, very high insulin resistance), the symptom is high levels of glucose in the blood. That is not the cause. It is the symptom.
High levels of glucose in the blood resulting from uncontrolled Type 2 Diabetes, results in proteins in the body becoming “glycosylated”. Glucose, is a highly reactive molecule and easily accepts (or “shares”) electrons from other molecules – especially from the amino acid Lysine, which is found in virtually every protein in the body. When Lysine and glucose share an electron, it creates an irreversible chemical bond between the glucose molecule and the protein – and that protein is said to have become glycosylated. It is this glycosylation that lies behind the complications found in Diabetes.
To reduce the glucose in the blood and the glycosylation of the body’s proteins, current treatment for Type 2 Diabetes involves medications that move glucose from the blood into the cells. This doesn’t really remove the excess glucose from the body, it simply moves it to a different location in the body. While these medications can be very helpful in the short term (until people begin to address the underlying dietary causes), over time these medications become less and less effective at removing glucose from the blood. In a sense, we become “medication resistant”, so additional medications are added. Once the various combinations of medications loose their effectiveness, people with Type 2 Diabetes are prescribed insulin as a treatment – because insulin moves excess glucose into the cells. But the cells are already overflowing with too much glucose!
Insulin is added as a treatment when the body is already producing too much insulin. The problem is the cells aren’t responding to the signal from insulin. The body doesn’t need more insulin – it needs the cells that are sensitive to respond to insulin’s signal.
Diabetes as a “chronic, progressive disease”
Type 2 Diabetes is described as a “chronic, progressive disease” because with current medication treatment, people eventually get worse. When they no longer respond to the initial medications prescribed that help move excess glucose from the blood into the cells, they are prescribed insulin which they take by injection – in order to force more glucose into already over-full cells. While people’s blood glucose gets better (i.e. the symptom improves), they gain weight as a result of the insulin injections and develop complications such as heart disease, stroke, kidney disease, blindness etc..
In the end, they don’t get better, but worse, fulfilling the belief that T2D is a chronic, progressive disease.
Redefining the Problem, Redefines the Solution
Rather than looking at the symptom (high blood glucose) as something that needs to be “fixed” with medications and later with insulin (when the medications are no longer effective), when we define insulin resistance and Type 2 Diabetes as a problem of excess insulin, we approach addressing the problem differently.
By changing what we eat, we can lower the amount of glucose in the body, which in turn causes the body to produce less insulin. With less insulin being produced, the cells begin to respond to normal amounts of insulin – reversing insulin resistance and yes, reversing the symptoms of Type 2 Diabetes.
Eating a low carb high fat diet and extending the amount of time between meals (intermittent fasting) lowers the production of insulin, resulting in the cells become more sensitive to its signal. Rather than addressing the symptom (which is high blood glucose) we are addressing the problem of too much insulin.
Have questions? Would like to know how I could help you?
Why not send me a note using the “Contact Us” form on the tab above.
In Part 2, I will explain how insulin resistance is measured and how we can track insulin sensitivity returning, as we continue to eat a low carb diet and increase the time between meals.
As I’ve made it a habit to do each weekday, this morning I went out for my walk, using Nordic poles. I had an appointment to keep, so I kept it to 3 km at a brisk pace, around that beautiful lake that I’ve previously posted a video update from.
Despite eating quite low carb and delaying the amount of time between meals each weekday, my fasting blood sugars remain high. I’ve noticed that after I walk in the morning, they come down significantly, so I’ve decided to integrate a short walk around my neighbourhood after dinner, to see if my fasting blood glucose lowers. It should, which leaves me to determine how long a walk is ideal. I don’t want to make it a “workout”, as that can interfere with sleep, but I also don’t want to make it so short that it doesn’t have any effect. Today I started with a 15 minute walk at a comfortably brisk pace. Tomorrow, I’ll try longer, to see if it changes the results in the morning, and if so by how much.
As I began my walk, I realized that I’ve lived in this neighbourhood for several years, yet never walk around it. I guess it’s time I get to take in the beauty that is all around me.
Practicing what I preach!
Joy
UPDATE
It turns out, that a leisurely 20 minute walk after dinner results in my blood glucose dropping to ~5.2 – 5.4 mmol/L (94-97 mg/dl) and staying that way through the night (measured at 1 AM and 4 AM and 6 AM in the interest of science, of course!).
Note: Everyone’s results following a LCHF lifestyle will differ as there is no one-size-fits-all approach and everybody’s nutritional needs and health status is different. If you want to adopt this kind of lifestyle, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.



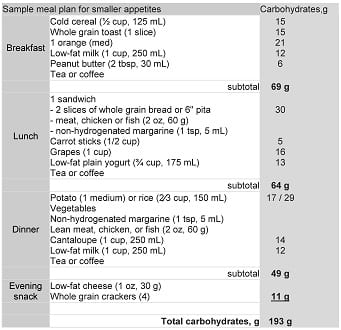


 Prepare an 8 1/2 or 9″ spring-form pan by lining with parchment paper and spraying well with an oil spray.
Prepare an 8 1/2 or 9″ spring-form pan by lining with parchment paper and spraying well with an oil spray. In the bowl of a stand mixer using the flat paddle or by hand, beat the cream cheese until very well blended and add the eggs one at a time, continuing to blend. Add the egg yolks, then the salt, granulated erythritol, and real vanilla.
In the bowl of a stand mixer using the flat paddle or by hand, beat the cream cheese until very well blended and add the eggs one at a time, continuing to blend. Add the egg yolks, then the salt, granulated erythritol, and real vanilla. Remove the bowl from the stand mixer and fold in the melted, cooled chocolate.
Remove the bowl from the stand mixer and fold in the melted, cooled chocolate. Turn off the heat of the oven and open the door, but leave the cheesecake inside for 30 minutes until partially cooled.
Turn off the heat of the oven and open the door, but leave the cheesecake inside for 30 minutes until partially cooled.








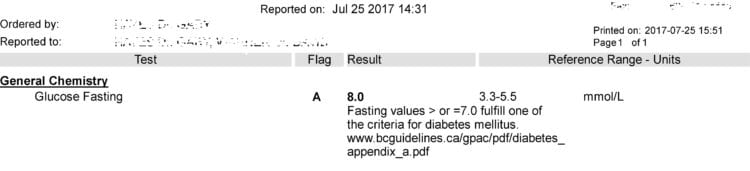
 I’d have a coffee in the morning (my usual cappuccino made with diluted cream, as opposed to milk as it has no carbs) and since there aren’t any carbs in it, it’s something I can enjoy when I am “fasting”…just like “bone broth”.
I’d have a coffee in the morning (my usual cappuccino made with diluted cream, as opposed to milk as it has no carbs) and since there aren’t any carbs in it, it’s something I can enjoy when I am “fasting”…just like “bone broth”.











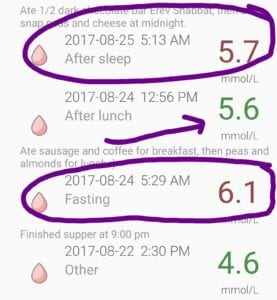


 The chia seeds are ground a little bit with the previously ground flax seed, and then the two ground seeds are placed in a small bowl.
The chia seeds are ground a little bit with the previously ground flax seed, and then the two ground seeds are placed in a small bowl.




 Last night, for the first time since I was diagnosed with Type 2 Diabetes (T2D) ten years ago, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl).
Last night, for the first time since I was diagnosed with Type 2 Diabetes (T2D) ten years ago, my 2 hour post-prandial blood glucose (i.e. two hours after a meal) was 5.8 mmol/L (105 mg/dl). My cells aren’t yet ‘healed’. They and my liver are still insulin resistant which is evidenced by the fact that even though I haven’t eaten anything since dinner last night, my blood glucose is high.
My cells aren’t yet ‘healed’. They and my liver are still insulin resistant which is evidenced by the fact that even though I haven’t eaten anything since dinner last night, my blood glucose is high.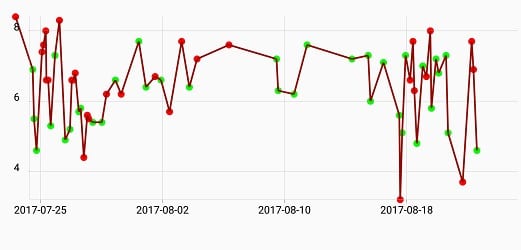
 Monday, my blood glucose was 3.7 mmol/L (67 mg/dl) at 4:00 PM and yes, I ate something immediately.
Monday, my blood glucose was 3.7 mmol/L (67 mg/dl) at 4:00 PM and yes, I ate something immediately.









 ). As with the eighteen-hour fast, one can have unsweetened coffee or tea with a drop of cream, club soda (seltzer) with a twist of lime or lemon, or “bone broth”. “Bone broth” can be made from any kind of meat, fish or poultry bones, but for me, when I think of “bone broth”, I think of a wonderful, rich broth made from beef marrow bones, that is gently simmered overnight on the stove, ready to be sipped as desired, on a fast day.
). As with the eighteen-hour fast, one can have unsweetened coffee or tea with a drop of cream, club soda (seltzer) with a twist of lime or lemon, or “bone broth”. “Bone broth” can be made from any kind of meat, fish or poultry bones, but for me, when I think of “bone broth”, I think of a wonderful, rich broth made from beef marrow bones, that is gently simmered overnight on the stove, ready to be sipped as desired, on a fast day.

 For the last 2 weeks, the Lower Mainland has been covered in smoke due to hundreds of wildfires in the area. The very poor air quality had made going for a walk impossible.
For the last 2 weeks, the Lower Mainland has been covered in smoke due to hundreds of wildfires in the area. The very poor air quality had made going for a walk impossible.


 Even wearing an N95 mask outside which is designed to filter out the small smoke particles, I have found my breathing very laboured.
Even wearing an N95 mask outside which is designed to filter out the small smoke particles, I have found my breathing very laboured.