When I set out on my “journey” on March 5, 2017 I didn’t have a particular weight loss goal in mind. I just knew that I was metabolically unwell and very overweight and that something needed to change (you can read a summary of that story here)! For years, I’d look in the mirror and long to see someone that looked like “me” looking back.
Over the first year since adopting a low carbohydrate and then a ketogenic therapeutic diet (March 2017-March 2018) I lost 32 pounds, put my Type 2 Diabetes into remission and significantly improved my blood pressure, but I didn’t reached the goal of getting my waist to height ratio (i.e. waist circumference half my height) so I knew I wasn’t “done” yet.
Since last December, I’ve lost 25 pounds (45 pounds in total) and today while cleaning a shelf over my desk, I found a piece of paper on which I had been keeping track of my body measurements since June 2017, including those taken from this time last year. That’s when I decided to see where on my body these last 25 pounds came from.
Of course, where my body took the weight from is specific to me, but for those reading this who are ‘women of a certain age’ or the friend of one, you might find this encouraging. It was a physician who teaches a low carbohydrate approach to her patients who suggested two summers ago that I take my measurements periodically to see where I am losing fat from and suggested measuring at my umbilicus*, chest (under my bust-line), neck, bicep and thigh. And so I have.
*umbilicus isn’t the same as “waist”. Waist is measured in a particular location explained in this article and umbilicus is the region where one’s “belly button” is.
taken November 2017
Since December of last year, I lost 6.5 inches off my umbilicus region. That’s pretty cool and yes, it shows as I recently had to punch 4 holes in my belt which I hadn’t worn since then. I’ve lost an additional 1 inch off my chest and 1 inch more off my neck (that shows too), 1.5 inches off my bicep (while adding muscle!) and here’s where it’s crazy; I lost 4 inches off my thighs — also while gaining muscle. In the first year I had only lost a total of a 1/2 an inch off my thighs, as can be seen here.
taken November 2018
When I look at these measurements over the last year and a half (from June 2017 until now), it is very encouraging. I’ve lost 9 inches off my umbilicus region, 2 inches off my chest (below my bust-line), a whopping 4 inches off my neck, 2.5 inches off my bicep while gaining muscle, and 4.5 inches off my thighs also while gaining muscle.
It’s my opinion that weight loss, like improved metabolic health is best done gradually but consistently. I don’t promote “rapid weight loss” even though a low carbohydrate or ketogenic diet is often promoted that way in the media. I also don’t believe that a ketogenic diet is necessary for all people, or even for most people. In fact, those who do not have significant metabolic health issues often do just great on a low carb diet, so my view is why limit good whole-foods that happen to contain carbohydrates if it is not needed to improve metabolic outcomes? In the four and a half years that I have been teaching this lifestyle, I have only had a handful of clients who were metabolically unwell enough for a long period of time that needed to keep lowering their carbohydrate intake down, some to a ketogenic level. Necessarily, each is being overseen by their own doctors — especially when it comes to monitoring (and adjusting the dosage of) their medications.
I approached my health as if I were my own ‘client’, so I didn’t start off at a ketogenic level of intake. I started “low carb” and only lowered the level of my carbohydrate intake gradually and only as much as necessary to achieve the metabolic improvements necessary. Since I had been overweight for 25 years and was diagnosed as Type 2 Diabetic 10 years earlier, I ended up needing to lower my carbohydrate intake to a ketogenic level but did so under the supervision of my doctor and with the oversight of my endocrinologist.
Whether you have a few pounds or like I did — many to lose or want to put one or more metabolic conditions such as high blood pressure, blood sugar or cholesterol into remission, you may want to find out more about how a low-carbohydrate approach can help, and why.
Feel free to send me a note using the Contact Me form above and I will reply as soon as I’m able.
To our good health!
Joy
NOTE: This post is classified under “A Dietitian’s Journey” and is my personal account of my own health and weight loss journey that began on March 5, 2017. Science Made Simple articles are referenced nutrition articles, and can be found here.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
From the beginning of my ‘journey’, I’ve said that I had no specific “ideal weight” in mind — that my goal was to reach a body weight where my waist circumference was half my height; whatever weight that was. This week, I reached that goal; 21 months from when I began.
This story began March 7, 2017. I was sitting at my office desk and didn’t feel well. I dug out my blood pressure machine (sphygmomanometer) which I had not used in ~ 2 years and took my blood pressure. The reading defied comprehension. I rested a bit and took it again. It was nominally lower, but still in the “hypertensive emergency” category. A hypertensive emergency is where the top number (systolic pressure) is at or over 180 millimeters of mercury (mm Hg) and the bottom number (diastolic pressure) is at or above 120 mm Hg, or higher. Mine systolic pressure was significantly higher than 180 mm Hg! I was seriously concerned that I could have a stroke! I was scared. Then I went to dig out my glycometer to measure my blood sugar.
Hint: it is never a good thing when someone with Type 2 Diabetes does not know where their sphygmomanometer or glycometer are!
I should have known where my glycometer and sphygmomanometer were and should have been using them regularly, but I was in denial. After all, I was eating “properly”; lots of fruit and vegetables, whole grain bread and rice and while I was overweight, my weight had been stable for a long time. Okay, I was obese, but was consistently fat. Like I said, I was in denial!
My blood sugar after lunch was 13.0 mmol/L (234 mg/dl). That was bad. I was clearly not tolerating the amount of carbohydrate in the fruit and whole grain crackers and it didn’t matter how many salad vegetables and lean protein I ate with it! I was carbohydrate intolerant.
A few months earlier, two women I had known from school died suddenly. Both were in healthcare. One was a public health nurse who retired on the Friday and was dead on the Monday and the other was a care aid working in long-term care who died alone in her home of a massive heart attack. She had been diagnosed about 8 months earlier with Type 2 Diabetes and was working with her “Diabetes Dietitian” and was diligently following the recommendations and eating 65 g of carbohydrate at each meal and 45 g at each snack. When I mentioned I had been doing a lot of reading in the literature about the application of a low carbohydrate diet in controlling Type 2 Diabetes, she said “I’m going to follow this for one year. If it doesn’t bring my numbers down enough, I will look into it“. She didn’t live long enough for either.
Obviously she didn’t die from following the recommendations, but I have to wonder what difference 6-months on a well-designed, supervised low carb diet might have had.
The fact is, I was no example! Why should she listen to me? I was as overweight as she was (okay, we were both obese!) and I had Type 2 Diabetes for 10 years. Who was I to suggest it if I wasn’t actually doing it? All the scientific literature and knowledge isn’t convincing coming from an obese Dietitian.
As I sat there March 7, 2017 reflecting on my astronomical blood pressure and blood sugar, I realized I could be next in having a heart attack or stroke if I didn’t DO something. As I’ve said many times before in this blog, I should have gone to my doctor and let him prescribe blood pressure medication, medication for lowering my blood sugar and the statins for my cholesterol that would have come along with them (as he’d been recommending those for a while), but I didn’t. What I did instead was immediately adopt a low carbohydrate diet. I designed myself a Meal Plan, as I do for my clients, based on the best evidence at the time. I’ve never looked back.
Without using any medication, here is what I was able to accomplish in one year’s time, as it appeared on Diet Doctor.
The full measurements are there, but in short, I had lost 32 pounds and lost 8 inches off my waist. I still had 4 inches to go until my waist circumference would be half my height, but I no longer met the criteria for Type 2 Diabetes and my blood pressure ranged from between normal and pre-hypertensive. My triglycerides were ideal and I had excellent cholesterol levels.
Here is my “before” and “after” pictures now, at 21 months. I’ve lost the additional 4 inches off my waist – a foot in total! I lost a FOOT off my waist!!
In total, I’ve lost 45 pounds.
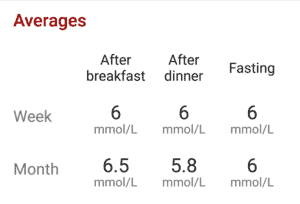
My 3-month average fasting blood glucose is 5.1 mmol/L (92 mg/dl) and 3-month overall average blood sugar is 5.4 mmol/L (97 mg/dl). I am below the diagnostic criteria for Type 2 Diabetes provided I limit the amount of carbohydrate-based foods I eat. I expect these numbers will continue to improve now that (based on my waist circumference being half my height) it is unlikely I have fatty liver (NAFLD) disease. It will still take more time for my liver to continue to get well, as well as my pancreatic beta-cells, if recovery is possible.
I am not an “angel” when it comes to eating. I do indulge in some dark chocolate after meals each weekend and I do taste non-low carb treats like pizza and cake. After all, this is not a diet, but a lifestyle and to be a lifestyle, it has to be sustainable. The question for me is the same as for anyone: “how much” and “how often”.
Was it difficult? No. It really wasn’t…isn’t.
I eat real, whole food that can be as simple or complicated as I feel like preparing. It can be some store-bought BBQ chicken and a boxed salad or moussaka from scratch (which is what I’m making for dinner, tonight). I eat animal-based sometimes, plant-based other times, I eat nuts and seeds, fish, poultry of all types and a wide range of vegetables and some fruit and I include some “starchy” vegetables like winter squash and yam from time-to-time. I eat dairy such as cheese and plain Greek yogurt and I occasionally eat eggs (I am not a big “egg person”!). I eat grass-fed beef when I get it and supermarket meat, pastured chicken and the one that goes on sale when I’m picking up staples. My butter is regular, local and unsalted (not fancy imported butter) and I don’t slather it on everything. It is just one of my fat choices along with really good olive oil and other pressed oils such as avocado oil and the occasional macadamia nut oil. If I’m craving a really good pizza, I make my Crispy Keto Pizza which is 85% the texture of a yeasty flour-based pizza. If I feel like one that’s a little less rich, I make my Crispy Cauliflower Pizza (see Recipe tab).
I usually don’t make “low carb bread”, although one of the most popular recipes on my recipe blog are my Low Carb Kaiser buns. Here’s a picture, so you can see they are pretty legit for a sandwich and are great as hamburger buns.
I even make the occasion dessert, with my most requested being my low carb New York Style Cheesecake (also under Recipes).
Low carb or not, I think desserts are “sometimes foods”, not “everyday foods”. As a formerly obese person, I don’t think it’s helpful to think of dessert as a necessary part of an everyday meal. I think they’re great for a special occasion, and make special occasions…well, special. After all, what’s not to love about a slice of cheesecake with the same number of carbs as a slice of bread, but the added fat, above and beyond what is found in the whole foods I eat is still an ‘extra’.
I invent recipes for myself that my ethnic clients find really helpful, including things such as Low Carb Roti (Indian flatbread) and Low Carb Chow Mein Noodles because I believe that a low carb lifestyle is not a “one-sized-fits-all”.
Everybody’s nutritional needs are different based on their stage of life, age, gender and health conditions and people have different food preferences. What works for me may not be what’s best for you. I design people’s Meal Plans based on the evidenced-based principles and their own preference, because it has to be sustainable.
Low Carb as a Maintenance Lifestyle
So, I’ve finally entered that wonderful phase known as “maintenance”; of needing to balance intake so I don’t continue to lose significant amounts of weight, but continue to achieve a more idea body composition (less extra fat, more muscle). That involves adjusting my “macros” (the percentage of protein, fat and carbohydrate) as I do for my clients when they reach this stage, and continuing to engage in activity that challenges my muscles.
It’s also about continuing to evaluate (as I do for my clients) which carbohydrates I can or cannot successfully eat, and in what quantities. I know that from research studies, carbohydrate is best tolerated after eating some protein and low carb veggies (you can read more about that here) but even then a 2105 study showed that each person’s response to carbohydrate is very different (discussed in this article). For example, I found that my blood sugar is great with whole, cooked chickpeas cooked from dried but is terrible with hummus as the grinding of the chickpeas makes the starch in them more available to digestion and absorption (you can also read more about that here). So, just like I follow-up my clients who are seeking long-term weight loss and healthy improvement, I do the same for myself.
Low carb is not “magic”. It’s not like the food you eat somehow doesn’t “count”. It has more to do with the different way our body metabolizes carbohydrate, compared with protein and fat and finding the mix of those that best achieves our goals. For me, that setting my intake in a way that maximized lowering my blood sugar and blood pressure and achieving a normal body weight. For someone else, it will be different. That’s why I say there is no one-sized-fits-all “low carb (or ketogenic) diet.
What are your weight loss and nutrition goals? Depending on your health and metabolic conditions, most can be realized using a well-designed, individualized, low carbohydrate Meal Plan.
Have questions?
Why not send me a note using the Contact Me form on the tab above and I will reply as soon as possible. Remember, I provide both in-person services as well as via Distance Consultation, using Skype or phone.
To our good health!
Joy
NOTE: This post is classified under “A Dietitian’s Journey” and is my personal account of my own health and weight loss journey that began on March 5, 2017. Science Made Simple articles are referenced nutrition articles, and can be found here.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
It’s twenty months today that I adopted a low-carb lifestyle and it’s hard to believe how very different I feel.
March 5, 2017, I was sitting in my office working on Meal Plans for my clients and I just didn’t feel well. I didn’t know what was wrong but for lack of a better term I felt “unwell”. I went and took my blood pressure (after not taking it for almost 2 years!) and it was dangerously high! I laid down and waited a bit until I took it again, and it was only nominally less. I was scared.
I decided to take my blood sugar too and opened a new package of test strips and took it. It was crazy high and I didn’t eat anything out of the usual. While I can’t remember exactly what I ate that morning, I’m guessing it was a few thin gluten-free crackers with peanut butter substitute and a bit of marmalade — which is what I usually ate along with a double espresso cappuccino made with low fat milk, without sugar. I just looked up the carb content of those crackers; 24 g of carbs for 3 and I probably ate 5 or 6, so, 50 g of carbs right there. Another 8 g of carbs for the 2 Tbsp of soya butter spread and 14 g per Tbsp for the Seville Marmalade — so altogether, that was 72 g of carbs, plus another 3 for the milk in the cappuccino. I had 75 g carbs for breakfast —’at least’ the 65 g of carbs that was recommended for me to eat as a Type 2 Diabetic.
Mid-morning, I probably had 2-3 ounces of cheese and a piece of fruit. Given it was early March, for sure it was an Ataufo mango — 25 g of carbs; a recommended combination of carbohydrate and protein…and not even the 45 g of carbohydrate recommended, as cheese doesn’t have any carbohydrate. The mots I would have had after that would have been some plain tea, so no additional carbs but knowing what I know now, my blood sugar probably continued to climb from breakfast for the next 3 hours, then I had the “healthy (recommended) snack” of protein and carbohydrate for another 25 g of carbs which would have caused it to rise some more. It was no wonder my blood sugar that day was 13.0 mmol/L (234 mg/dl).
I was a sick! I had out of control blood pressure and blood sugar that was anything but controlled! I contemplated going to my doctor but figured he’d either send me to the hospital by ambulance because of my crazy high blood pressure, or he’d prescribe at least one kind of blood pressure medication, blood sugar medication and a statin for my cholesterol (which he wanted to put me on for some time). In retrospect, I should have gone to see him and let him put me on the blood pressure and blood sugar medication and THEN changed my lifestyle. The meds would have protected me in the meantime until the dietary and lifestyle changes began to have their effect. But I didn’t. What I did do was instantaneously adopt a low-carb lifestyle — the same type of plan I had been designing for my clients for over 2 1/2 years.
The rest, as they say, is history.
All the details are in previous entries in “A Dietitian’s Journey”; all the lab tests, all my blood glucose and blood pressure readings and all my fat pictures! There it is in Technicolor for anyone to see!
The photo on the left (below) was taken April 21 2017 — 7 weeks after I began my current lifestyle and the photo on the right was taken last week or the week before.
Yes, I am a lot grayer, but the change in the shape of my face and my neck (I have a neck!!) is evident. When I look in the mirror, I now recognize the person that looks back.
Best of all I feel good and my lab tests and blood pressure readings indicate that I am much healthier — not just for someone diagnosed 10 years ago with Type 2 Diabetes (T2D), but for someone of my age without any chronic diseases! My T2D is in remission, which means that as long as I keep eating the way I do, it will stay that way. This is not a “short-term fix”. If I want to remain healthy, I need to keep eating the way I do. Does that bother me? No! The alternative is being as unhealthy as I was 20 months ago. No way.
Note: I use the word “remission” and not “reversal” because for Diabetes to be reversed, a person should be able to eat like a non-Diabetic and not have their blood sugar spike. For me, that’s not likely to ever happen because I was Diabetic for so long, so I use the term “remission”.
Remission is a good thing!
Having normal blood sugar levels and normal blood pressure is fantastic, and catching my reflection in a store window or on a store video camera isn’t an unpleasant experience.
Of course I’m not going to look like I did in my mid-twenties when I was last at this weight but to be someone of normal body weight, with labs that testify that I am not the metabolically unwell mess that I was 20 months ago is just fine with me. I’m not going to get any younger, so I will just have to keep getting better!
If you are wondering if it is even possible to go from being obese and metabolically unwell to being normal body weight and metabolically as healthy as reasonably possible, I hope my story encourages you that yes, it is entirely possible. Is it hard? No, not really. It takes learning how to do things differently, but if doing the same thing was making me sicker and sicker, I didn’t need my Masters degree to figure out doing the same thing was not going to make me better. There were years of scientific data before I began teaching this almost 5 years ago and now there is significantly more. Even the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) now recognize that a low-carbohydrate diet is safe and effective and has deemed it appropriate Medical Nutrition Therapy for the treatment and management of T2D (you can read more about that here).
If you have questions about how I might be able to help you please send me a note using the form on the Contact Me tab above and I’ll be happy to reply.
I provide both in-person visits in my Coquitlam, British Columbia office as well as visits via Distance Consultation on Skype or by phone if you prefer, so please let me know how I can help.
To our good health!
Joy
NOTE: This post is classified under “A Dietitian’s Journey” and is my personal account of my own health and weight loss journey that began on March 5, 2017. Science Made Simple articles are referenced nutrition articles, and can be found here.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Today I reached “normal body weight” according to Body Mass Index (BMI) classification — no longer obese and not even overweight. Normal. It seems surreal.
When I began my health and weight loss journey on March 5, 2017 (19 1/2 months ago) I was obese. My weight bordered between Class I and Class II Obesity and I had multiple metabolic health issues. I was diagnosed with Type 2 Diabetes 10 years earlier, had elevated blood pressure and abnormal lipids (cholesterol). Most significantly, I was in denial as to just how ill I really was. The undergraduate and post graduate degrees on my wall did not inform reality. The mirror did.
I didn’t feel well that day and took my blood pressure. It was dangerously high— classified as a hypertensive emergency. I decided to take my blood sugar too and it was way too high. I sat and considered the numbers of both and considered my options. At the time, I only saw two choices; I could go see my doctor who would have immediately put me on multiple medications or I could change my lifestyle. In hindsight the safest option would have been to do both, but I chose instead to begin to “practice what I teach”.
You see, I had two girlfriends suddenly die of natural causes within 3 months of each other just previous to that day; one of them I had known since high school and the other since university. They were both my age, both chose careers in healthcare, just like I did, and both died from preventable causes. They spent their lives helping others get well, yet unable to accomplish the same for themselves. It was not for lack of trying, but for not having found a solution before death ended both of their lives. March 5, 2017, I realized that if I didn’t change I would likely die of heart attack or stroke, too. Their deaths may have saved my life.
I began a low carbohydrate diet immediately. I cut refined foods, ate whole unprocessed foods, didn’t avoid the fat that came with whole foods but didn’t add tons of fat either. While it helped a great deal, after several months I realized that I needed to lower my carbohydrates further in order to achieve the remission from Type 2 Diabetes that I sought. I didn’t simply want to lose weight — I wanted to get healthy!
I consulted the experts and continued to make dietary modifications that got me closer to my goal. The first significant improvement was in blood pressure followed by blood sugar. I lost weight and more significantly lost inches off my waist. While I hadn’t been formerly diagnosed with non-alcoholic fatty liver disease based on my lab work I more than likely had it. I tweaked and adjusted my Meal Plan many times over the last 19 1/2 months — each time moving myself closer and closer to my goal. Ten days ago I was within an inch of my waist circumference being half my height and now I am within 3/4 of an inch of it. It’s happening!
Body Mass Index (BMI) October 17 2018
Two days ago, I got on the scale and saw a series of digits that I had not seen since my twins were born 26 years ago tomorrow. I decided to crank some numbers. I was almost there. The photo on the left shows the weight category form two days ago. Today it was in the normal range!
I am not one of those people that the press frequently writes about that pursued a low carbohydrate or ketogenic diet for “quick weight loss”. I wanted to get well. I chose a low carbohydrate diet for therapeutic reasons because it was my underlying high insulin levels which drove my high blood glucose and high blood pressure. To get well, I needed to address the cause, not the symptoms.
So here I am, having reached normal body weight!
Did I think at the beginning that I would actually get to this point? I wasn’t sure. I knew it was possible because I had helped others achieve it, but had never tried myself, so I didn’t know.
For health reasons, I no longer had the option of doing nothing!
At first, I set my preliminary goal as “no longer being obese“. Then I revised it to “being less overweight“.
I found some old photos recently of what I looked like as a young adult and realized what the weight was where I felt and looked my best then reset my goal weight once again. I knew it was entirely doable!
I am almost there!
Then the hard work begins.
Losing weight has been challenging, but not difficult. Sure, I needed to determine what was holding things up at various stages of my journey and make dietary adjustments just as I do for my clients, but it’s much easier to do that for someone else than for oneself. The “hard work” will be finding out how to eat where I don’t lose any more weight, while maintaining my blood sugar and blood pressure at the best possible level.
If possible, I want to achieve full remission from Type 2 Diabetes and if not, I will learn how to maintain full reversal of symptoms.
I’ve documented the entire process throughout “A Dietitian’s Journey”, including “fat pictures” and lab test results to demonstrate the therapeutic benefit of a low carbohydrate diet and that this lifestyle is bothpractical and sustainable.
Perhaps you would like to find out how I can help you achieve your own health and nutrition goals?
Please send me a note using the form on the Contact Me tab above and I’ll be happy to reply.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This week has been 19 months since I started a low carbohydrate lifestyle and 10 months since I began following a ketogenic diet with my doctor’s and endocrinologist’s oversight and I’m very close to reaching most, if not all of my health and weight loss goals.
Weight
When I began my health and weight loss ‘journey’, I had 30 lbs to lose to get to the preliminary weight goal that I set for myself — which was still in the overweight classification, but was the only goal that seemed theoretically attainable at the time.
When one is obese, it’s difficult to imagine being anything but “only overweight”, even for a Dietitian. As I do with my clients, I set a preliminary weight target that seemed it may be attainable.
I reached my preliminary goal weight in February of this year and said to myself “okay, now what“? My waist circumference was still not 1/2 my height (associated with the lowest risk of cardiovascular disease, described in this article) so I carried on.
So far this year, I’ve lost 15 additional pounds and 4 more inches off my waist.
As I jokingly quipped on social media recently;
“my waist circumference is FINALLY half the height I was before I started shrinking… does that count?”
Based on my current height (an inch less than I was as a younger adult), I have another inch to lose. I’m so close!
I’m also 10 pounds from the weight I was before I had children — and given my twins will be 26 years old soon and my singleton will be 25 at Christmas, achieving my “pre-baby weight” has been a long time coming!
Me with my 3 sons in 2002
What We Believe is What We Achieve
I realized yesterday that what we believe is possible has a lot to do with what we achieve.
There are a handful of life goals that I thought I’d never achieve because I didn’t believe they were attainable, but after a few years of using a low carb approach with my clients and seeing their success, I started “practicing what I teach”… and here I am, 10 pounds from the weight I was before I had children. With having had twins and then a singleton within 14 months of each other, that is a lot of weight that was not lost previously by trying to cut calories and exercise more…plus the added weight I gained from eating foods that were a mixture of fat and carbohydrates because they were irresistible.
For the last number of months I have been steadily losing inches off my waist but without losing any weight at all. I knew that as long as I was losing either inches or pounds, I was not at a “plateau”, so I carried on.
Adapt Your Life Vancouver – September 15, 2018
September 15th, a little less than month ago, I had the opportunity to hear Dr. Eric Westman speak in Vancouver on the ketogenic diet that he uses in his own clinical practice.
Dr. Westman is Associate Professor of Medicine at Duke University Health System and the Director of the Duke Lifestyle Medicine Clinic and is an internationally known researcher specializing in low-carbohydrate nutrition. Dr. Westman is currently the Vice-President of the American Society of Bariatric Physicians and a fellow of the Obesity Society and the Society of General Internal Medicine and has co-authored three books to date, including The New Atkins for a New You (co-authored with Dr. Stephen Phinney and Dr. Jeff Volek).
I welcomed the opportunity to learn from someone that has been following a ketogenic lifestyle, researching and publishing about it and teaching it to his patients for many years.
One of things I learned was a very practical way to determine one’s idea body weight. According to Dr. Westman, it’s the adult weight that a person felt and looked their best at. The other thing that I learned was in his approach to following a strict ketogenic diet, there is a need to eliminate fruit and nuts. More on that later…
I began to think about what was the adult weight I felt and looked my best?
I came up with what that weight was and thought to myself; “What? Really? That’s very…low!” To try to look at it more objectively, I asked myself if that weight was either unrealistic or unattainable.
My ‘best’ adult body weight is 18 pounds more than my lowest adult body weight (where overweight family members were concerned I had an eating disorder!) but is 5 pounds less than the weight I was before I had my children, including multiples. I concluded that this weight seems both attainable and realistic.
When I calculate my Ideal Body Weight, it’s the weight I was at 21 years old when family members worried about me and which was only sustained for a very short time before my wedding. It was certainly not where my natural set point was when I was physical active and fit. That weight was where I looked and felt my best. Dr. Westman’s method made sense for me.
Calculated Ideal Body Weight
I’ve always found that calculated Ideal Body Weight (IBW) based on established formulas to be a discouraging and unattainable goal for my overweight or obese clients.
Ideal Body Weight (IBW) Formulas
Men: 50 kg + 2.3 kg for each inch over 5 feet
Women: 45.5 kg + 2.3 kg for each inch over 5 feet
Clinically, I’ve tended to use Adjusted Body Weight (ABW) as “ideal” with my overweight and obese clients as it is applicable if a person’s Actual Body Weight (what they currently weigh) is greater than 30% of the calculated Ideal Body Weight (IBW). To most, if not all of my overweight and obese clients, achieving Adjusted Body Weight usually seems like a Technicolor dream.
Adjusted Body Weight Formulas
Men and Women: IBW + 0.4 (actual weight – IBW)
For me, my Adjusted Body Weight is also the adult body weight that I felt and looked my best at so that is my next goal.
Using Dr. Westman’s method of aiming for the adult weight that I felt and looked my best, which is also my Adjusted Body Weight, I still have ~15 pounds to lose.
The Exercise Factor
Something else I needed to factor in to my weight loss plan is the “exercise factor”. Now that my eating is no longer driven by cravings for carbohydrate, made worse by high insulin levels, I am naturally “eating less and moving more“; which is a natural outcome of eating a low carbohydrate diet, not a means to an end! I am ABLE to move more BECAUSE I am eating less!
For the last 6 weeks, I’ve been doing resistance training 4-5 times per week (using body weight, resistance bands and dumbbells and barbells) and this is resulting in me building and toning muscle.
I expected that my weight loss would be slowed because muscle is heavier, but that’s not actually happening.
Strict Ketogenic Diet – Dr. Eric Westman’s Approach
Since January (i.e. for the last 10 months) I have necessarily been following a ketogenic diet in order to lower my blood sugar to below the Diabetic range, eliminate high blood pressure and to achieve and maintain a waist circumference that is half my height. As I’ve told many of my clients, my level of carbohydrate intake is significantly lower than any Meal Plans that I have designed for others and this is because of the degree of metabolic disruption I had previously caused myself. I had been Type 2 Diabetic for 10 years, was obese and worse, was in complete denial about the health risk to myself until March 5, 2017 when this ‘journey’ began.
Dr. Westman taught at the conference was that in the weight-loss phase of a strictly ketogenic diet he recommends that his patients stick to real protein foods (meat, poultry, fish and shellfish and eggs), salad greens and low carbohydrate vegetables, plus limited quantities of healthy fats and oils, cheese and cream. What isn’t included in this phase of the ketogenic diet he has his patients follow is fruit and nuts, not even on salad.
Since I saw Dr. Westman speak on September 15th, I gave up nuts and fruit and since then, I’ve since lost 2 pounds and another 1/2 inch off my waist.
Effect on Blood Glucose
The effect of giving up fruit on blood glucose is also observable.
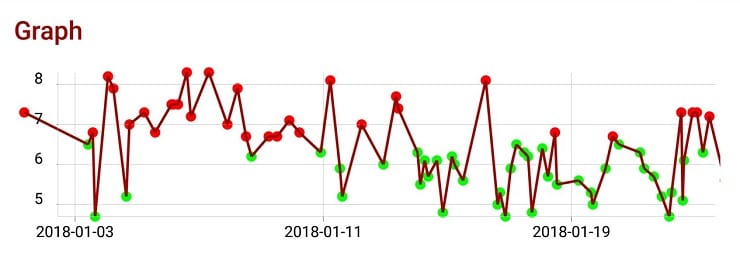
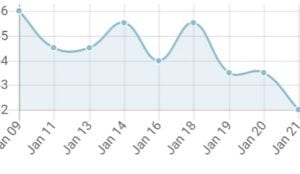
September 15-October 10 2018 blood glucose versus previous 2 months
During July and August it was local blueberry and blackberry season and I ate far too many, way too often. I justified that they are good antioxidants, which they are, but they are not ideal foods for someone like myself who’s been Type 2 Diabetic for 10 years…at least not at this stage of my metabolic reversal.
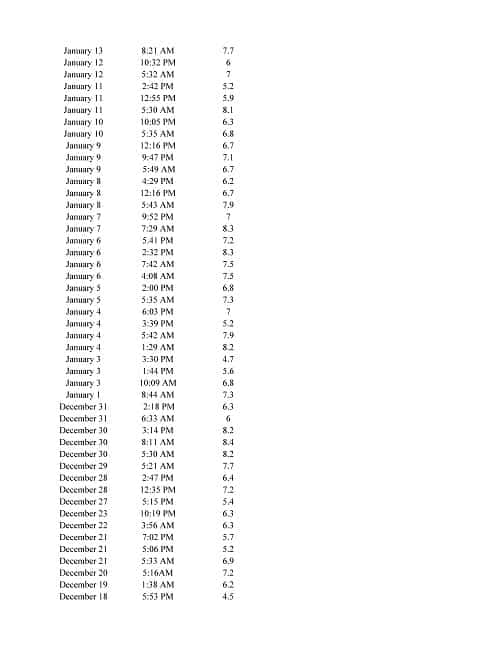
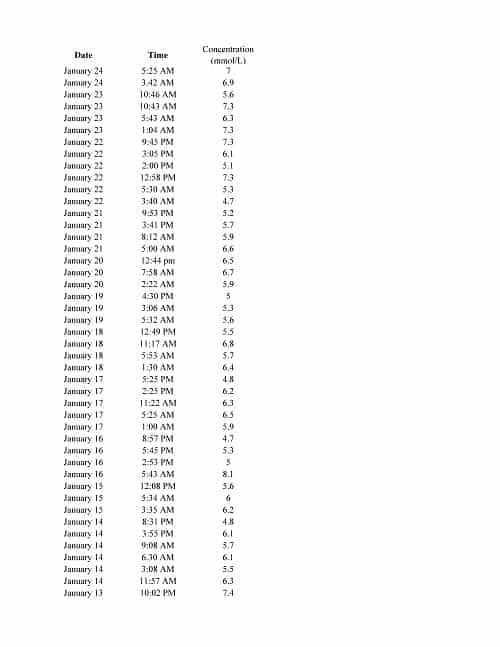
As can be seen in the graph of my own glucometer readings (above) my average blood glucose in July and August was 6.3 mmol/l (114 mg/dl). Since September 15th, I’ve cut out all fruit, not even a few berries on my salad and I no longer reach for nuts as part of a mid-day meal, but a hard boiled egg or hard cheese or fish, instead. My average blood glucose has dropped to 5.1 mmol/L (92 mg/dl).
Based on the literature, about half of this effect is due to the Metfomin that I continue to take (protective measure given the Alzheimer’s diagnosis of my father and family history of cardiovascular disease) and the other half is due to me having stopped eating fruit.
I am currently achieving normal blood sugar levels, which is amazing! Both my endocrinologist and I hope that in time she can withdraw the recently prescribed Metformin and I will be able to sustain my blood glucose with diet alone, once my liver and pancreas have more fully healed. Time will tell. In the meantime, I am doing everything I can do to get well and stay well.
NOTE: Keep in mind, these are my (n=1, sample set of 1) results based on my specific medical history and metabolic conditions. Since everybody’s needs are different, there is no one-size-fits-all “low carb” diet for everyone.
Perhaps you wonder how a carefully-designed low carbohydrate or ketogenic diet could help you improve symptoms of Type 2 Diabetes, lower high blood pressure or simply lose weight? Please send me a note using the ”Contact Me” form above to find out more.
Feel free check out the various services that I offer under the Services tab or in the Shop and if you’d like to get started, you’ll find everything you need there.
I provide both in-person in my Coquitlam, British Columbia office or via Distance Consultation on Skype of long distance phone, so please let me know how I can help.
To our good health,
Joy
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
A month into following a low carbohydrate diet I came out of denial with respect to how very unhealthy I was (and had been for a very long time). I wrote about facing the reality that I had Type 2 Diabetes for 10 years, was obese and had dangerously high blood pressure and high cholesterol. You can read about that here.
My fasting blood glucose was close to 12 mmol/l (216 mg/dl), my blood pressure ranged between Stage 1 hypertension about 50% of the time to 1/3 of the time in Stage 2 hypertension (with one hypertensive emergency that was the impetus for me beginning this “journey”), and my LDL cholesterol was higher than it should have been given my family history. The fact was I was an obese Dietitian (BMI > 30) and coming out of denial enabled me to plot my course for what I had to do to get healthy and what that needed to “look like” — how much my blood sugar, blood pressure and cholesterol needed to come down and how many pounds and inches around my waist I needed to lose. It seemed daunting!
So here I am coming out of denial again — just a different type of denial this time.
The cold, hard truth is that I am out of shape. Sure, I no longer get puffed out walking briskly for a few kilometers as I did at the beginning of my “journey” (as these two really short video clips testify), but my efforts at implementing slow high intensity workouts has failed miserably. While I still have relatively strong arm and leg muscles and can lift and carry heavy objects, my “core” is hit and miss — mostly miss. Our “core” are those muscles in the trunk of our body that are responsible for supporting the heavy lifting work that the muscles in our arms and legs do. When they aren’t sufficiently strong, pain and injuries occur.
Core Muscles
Over the last few months of continuing to do slow high intensity workouts (working large muscle sets until failure), I’ve suffered with sore knees and periodically a sore back, too. Since I’d had both knees operated on a number of years ago (after years of martial arts and dance) my knees bothering me really wasn’t too much of a surprise. Neither was my intermittent lower back pain as I was hit from behind in a car accident a decade ago and was in physiotherapy for many months.
I thought I was engaging my “core muscles” when I was lifting, but I wasn’t —at least not all of them. While I remembered where my ‘transverse abdominals’ were (having learned in physio) and was engaging them when lifting weights, I had completely forgotten about using my pelvic floor muscles in tandem with them, as well as the other muscles that make up my ‘core’. I wasn’t consciously aware of it, but little by little I was injuring myself; my knees, my shoulder and my back. The ‘last straw’ was me setting up a gazebo for a family BBQ at which point my back made it clear that I could not continue. I was in terrible pain like I had not been since the car accident a decade ago and had to stop everything. I couldn’t sit for long, walk for long or stand for long so that didn’t leave much. I needed help.
After a few weeks of applying ice, rest and taking anti-inflammatories, I am now in active rehabilitation — doing many of the same exercises that I did a decade ago after my car accident. The harsh reality is there is no “quick fix” to my physical health, just like there wasn’t with my metabolic health when I began changing how I ate 18 months ago. I will need to work on this 3-4 times a week for an hour or more at a time over the next few months. But I will get healthy.
Why am I sharing this?
Because achieving health isn’t something we can always do on our own.
We can all workout on our own and make our muscles stronger, but the fact is if we aren’t working with a kinesiologist who has studied muscle physiology, then we will only be achieving partial results while putting ourselves at risk of injury. We can convince ourselves that a book or a friend or the “trainer” at the local gym can help us (and they can to a point), but they are not kinesiologists. If we have had previous injuries or for those that have never really exercised regularly before, then we need to work with someone that can teach us how to do it safely and design a program for us to make progress without getting hurt or doing ourselves damage.
Likewise, people can buy a book or find a generic ‘diet’ on the internet to lose weight, lower blood sugar and blood pressure a few points and bring their cholesterol down, but if they have metabolic conditions and especially if they are taking medications for them, they are putting themselves at risk doing it on their own (more about that in this article). Getting nutrition advice from a book, or a friend or the “nutritionist” at the gym is not the same as working with a Registered Dietitian and/or a physician who specializes in it, and who can design a individual diet based on a person’s specific needs and supervise their progress. To put Type 2 Diabetes into remission, reverse the symptoms of high blood pressure and high cholesterol and to get off medications for these conditions takes working with a professional.
I’ve learned my ‘lesson’ the hard way but it need not have been so.
The first step for any of us is coming out of denial — in admitting how unhealthy we are and to seek the help of a healthcare professional that is qualified to help.
Perhaps you’ve never considered getting the support of a Dietitian such as myself and have questions, or maybe you are where I was at 18 months ago and feel overwhelmed with the amount of weight you have to lose and what needs to occur to get metabolically healthy.
I can help.
Please feel free to send me a note using the Contact Me form above and I will reply as soon as possible.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This morning I went for a walk at one of my favourite places (Como Lake Park) and decided it was time to post a video update. It’s short (1:36 seconds) and stands in sharp contrast to the video that I made and posted 16 months ago on March 16, 2017 (1:35 seconds) at the very start of my low carbohydrate journey, a Dietitian’s Journey.
Looking at the two videos (posted below) there’s no mistaking how significantly overweight and out of shape I was on March 16, 2017 compared to today – and I’m not done yet.
July 25, 2018 – today’s video
March 16, 2017 – my first video
Looking at freeze-frame photos from both videos one on top of the other (below), the progress I’ve made is unmistakable.
I have 4- 1/2 years experience teaching a low carb lifestyle to my clients, and I have 16 months living it myself, with weight loss and clinical results that are visible and verifiable. You can review my latest lab test results here.
A Dietitian’s Journey – 16 month video update (March 16, 2017 – July 25, 2018)
I am no longer an obese Dietitian with uncontrolled Type 2 Diabetes, high blood pressure, abnormal cholesterol and high insulin levels. I “practice what I teach”.
If you would like to begin your own “journey” and want the professional support of a knowledgeable Dietitian that’s been there, then please feel free to send me a note using the Contact Me form on this web page or you can send me the completed Intake and Service Option Form if you’d like to get started. I provide services via Distance Consultation using Skype or long distance telephone, as well as in-person in my office. You are welcome to begin with a single visit to get to know me and my teaching style or to take a package which will give you everything you need to get started on your own journey. A complete description of each package is available under the Services tab as well as in the Shop, with a summary on the form.
I greatly look forward to helping you recover your own health, as I’ve been able to recover my own.
To your good health,
Joy
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
If you’ve been following my 16-month journey, you know that my goal has been to put my Type 2 Diabetes into remission and to no longer meet the criteria for Metabolic Syndrome.
July 11, 2017 I had complete lab work done, including fasting insulin, cholesterol, fasting blood glucose and glycated hemoglobin (HbA1C). I planned to redo the same tests at the same time this July to see how much progress I was making.
The day I had been waiting for arrived!
So, how did I do?
Let’s see where I started from in July 2017;
fasting insulin July 11, 2017
Last year, my fasting insulin was 54 pmol/L which converts to 7.8 μU/ml — well above the ideal insulin sensitive range of 2-6 μU/ml. I was insulin resistant, which was no surprise given I had Type 2 Diabetes for more than 10 years.
What about yesterday – 16 months after starting a low carbohydrate lifestyle?
fasting insulin, July 10, 2018
I went from 54 pmol/L (7.8 μU/ml) to 33 pmol/L (4.8 μU/ml). I no longer have high insulin; in fact, my insulin was now in the ideal range, between 2-6 μU/ml. Very cool!
But then what explains why my fasting blood sugar is still so high?
fasting blood glucose July 11, 2017
I mean, it has dropped a lot from 8.0 mmol/L (144 mg/dL) last year to 6.9 mmol/L (124 mg/dl) this year, but this was still a huge disappointment. Yes, many days my fasting blood sugar is in the low 5’s mmol/L (94-95 mg/dl) but not this time. It was at the high end of what it goes to!
Why?
fasting blood glucose July 10, 2018
In the last several months, I’ve been losing a lot of fat from my abdomen (2.5 more inches since the beginning of March, on top of the 8 inches I lost in the first year) and the end result of the action of hormone sensitive lipase on fat cells (adipocytes) is the release of free fatty acids and glycerol. The liver cells (hepatocytes) take the glycerol and turn it into glucose in a process called gluconeogenesis (literally “making new glucose”). It is this glucose that is produced by my liver from my broken down fat stores that is raising my fasting blood sugar.
The good part is that my fat cells are emptying out. The bad part is that my liver is making glucose out of it…and what complicates the matter is that I have what’s called “peripheral insulin resistance” from often eating only once a day (time-restricted-eating) and that causes my body to “save” the glucose for necessary processes. As a result, my body cells don’t take in the excess glucose made by my liver and it hangs around in my blood until I get moving. Then it will dissipate (provided I eat some breakfast).
What about my glycated hemoglobin (that is effectively the three month average of my blood sugar)?
glycated hemoglobin (HbA1C) July 11, 2017
A year ago, my HbA1C was 7.5% which is well above the cutoffs of 7% which is set for those with Type 2 Diabetes.
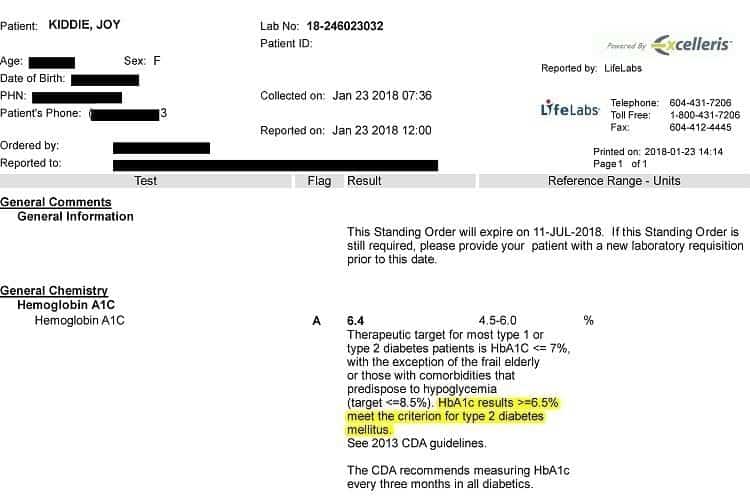
glycated hemoglobin (HbA1C) July 10, 2018
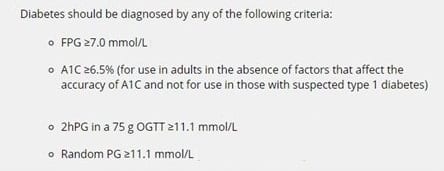
This year it was 6.3% which is below the cutoffs for Type 2 Diabetes of 6.5% and lower than what it was 3 months ago, which was 6.4%. Naturally, it is higher than I would like because it includes all the glucose my liver is making from the fat cells it is breaking down, but sooner or later it is going to run out of that! Soon my waist circumference WILL be half my height and around that point, my fasting blood glucose should be dropping. My goal is to see my HbA1C below 5.5 mmol/L (100 mg/dl) and be in full remission from Type 2 Diabetes, not only partial remission which is what I have now.
But celebrating the victory, I am in partial remission of Type 2 Diabetes!!
So how have my lipids changed this last year, with the butter, coconut oil and coconut milk and full fat cream that I have been eating, as well as much more meat than I used to?
Last year, four months into my low-carbohydrate journey, this is what they looked like:
Lipid panel, July 11, 2017
…and this year?
Lipid panel, July 10, 2018
My LDL is down (2.60 to 2.47 mmol/L) , my HDL is up significantly (1.97 to 2.44 mmol/L), my non-HDL cholesterol (chylomicrons and VLDL) is down (2.45 to 2.11 mmol/L) and my already low triglycerides went even LOWER (0.64 to 0.52 mmol/L).
In July 2017 my TG:HDL ratio was 0.35, which is well below 0.87 and this year my TG:HDL ratio was 0.21! This means that of my LDL cholesterol, most are the large fluffy kind (the ‘good’ LDL), and not the small dense kind (the ones that put us at cardiovascular health risk).
I no longer meet the criteria for Metabolic Syndrome which is having 3 or more of the following 5 symptoms:
Criteria for Metabolic Syndrome – from Merck Manual
My waist circumference is significantly <35″
My blood pressure is well below 130/85 (usually around 120/70)
My triglycerides are well below 1.7 mmol/L (150 mg/dl) at 0.52 mmol/L
My HDL is well above 1.29 (it’s 2.44 mmol/L!!)
…but yes, my fasting blood glucose is still > 5.6 mmol/L (100 mg/dl).
So, I’m not “done” yet.
While I didn’t get “perfect” blood work, it’s pretty good for someone that 16 months ago was obese, had been Type 2 Diabetic for 10 years, had been diagnosed 3 years earlier with mast cell disease (which elevates blood sugar and insulin), had extremely high blood pressure and abnormal cholesterol.
Not bad at all.
…and all this by simply reducing my carbohydrate intake and eating whole, real food, including fruit, dairy, meat, lots of veggies and healthy fats from a variety of sources.
Of course, these are only my results. Everyone is different, but at a year, my results closely mirrored the results Virta Health’s study published at one- year study, with 218 subjects that had been eating the same as I have. So, it is certainly not unusual for people following a well-designed low carbohydrate diet to get these kinds of results.
NOTE: There is no "one-size-fits-all" low carbohydrate diet and what works for me may not be what is best for you. Before undertaking a major change in diet, please discuss your plans with your doctor.
Perhaps you wonder what adopting this type of eating style would look like for you, or have questions about how Distance Consultation services work and the cost involved. Please send me a note using the ”Contact Me” form above and I’ll reply shortly.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
I’ve never told anyone that what they needed to do to lose weight was “eat less and move more”, but I know many of my clients have been told this by other clinicians, but who was I to talk? After all, I was an obese Dietitian.
The photo on the left was me before I began what I’ve called “my journey”, a Dietitian’s Journey.
Not only was I very overweight, but I had Type 2 Diabetes, high blood pressure and high cholesterol and was in denial about how very metabolically ill I was.
I was in denial partly because I believed that I was eating a healthy diet for someone with Type 2 Diabetes. I dutifully followed the recommended diet from the time I was pre-diabetic until I was diagnosed as having Type 2 Diabetes and continued on it because that is what was recommended to control my blood sugar. I deliberately avoided missing meals or fasting, to keep my blood sugar stable.
As per the recommendations for Diabetics, I ate 193 – 259 g of carbs per day, plus sufficient daily protein for my age and a little essential fat. Keep in mind that only the recommended amount of daily carbs adds up to ~800 – 1000 calories per day — and with sufficient protein for my age was another ~4oo calories, plus another ~150 calories or so in olive oil and a few nuts or seeds on my salad. With intake of 1400 – 1500+ calories per day, how was I supposed to lose weight?
If “eating less” was not an option for me then of course, I was expected to “move more”. If I didn’t move enough to burn off the excess carbohydrates that I was expected to eat as someone with Type 2 Diabetes, then this was my fault. This is why I was fat. Right?
Really?
My diet was “healthy” by most people’s understanding — certainly as defined by the Dietary Guidelines (Canada’s Food Guide) as well as the Clinical Practice Guidelines for Diabetes. My bread was whole grain and so was my pasta and I ate brown or red cargo rice (with the husk). Lunch and dinner and my 2 snacks per day were comprised of lots of fruit and vegetables of all kinds along with some lean protein; 3-4 oz at each meal and an ounce of cheese at snacks. I barbecued meat, fish and chicken all year round and if I did pan-fry something, I always poured off the ‘excess fat’. The quantities I ate were recommended by the guidelines and as evidenced by the fact that I neither gained nor lost any weight.
Eating 65 g of carbs at each meal along with protein and 45 g of carbs at each of 2 snacks each day along with a bit of protein however didn’t help me avoid getting Type 2 Diabetes — so what was I expecting to accomplish eating this way after I was diagnosed?* It was supposed to help me “manage my blood glucose levels”, but unfortunately after a few years of eating that way, I ended up getting high blood pressure and then abnormal cholesterol as well, which is common.
*I believe that some people with Type 2 Diabetes do well eating according to the standard recommendations of the Clinical Practice Guidelines and others by following a whole foods, Mediterranean-style Diet. There is also strong research evidence that still others achieve excellent clinical results following a therapeutic low carb or a well-formulated ketogenic diet for a period of time. There is no one-size-fits-all diet for everybody and it is for this reason that I offer people choices.
When I saw my Endocrinologist 2 1/2 years ago, she said that if I kept eating as I had been, that in 2 years I would be on medication for Diabetes, hypertension and high cholesterol and within 5 years, I would be on insulin. At that time, I discussed with her my intention to eat a low carb diet and how low in carbohydrate I was willing to go, if I needed to. I was expecting a great deal of resistance from her, given some doctors consider a low carb diet unconventional. Her response surprised me. She told me that me that eating very low carb was the best chance that I had to avoid the scenario she outlined above as well as the complications of Diabetes, including blindness and lost limbs. In fact, she recommended less grams of carbs per day than I was intending.
Unfortunately, it took another 2 years before I became metabolically unwell enough to actually begin to implement the dietary changes, but with my Endocrinologist’s approval and encouragement, as well as my GP monitoring my health, March 5, 2017 I began changing how I was eating and I’ve never looked back.
Me – July 2 2018 (16 months later)
The photo on the left is of me yesterday.
As of today, 16 months into my journey, I’ve lost;
39 pounds (18 kg)
10.5 inches off my waist (27 cm)
2.5 inches off my chest (6.5 cm)
3 inches off my neck (8 cm)
1.5 inches off each arm (4 cm)
1.5 inches off each thigh (4 cm)
Both my HbA1C and FBG are in the non-diabetic range
My blood pressure is normal for someone without Type 2 Diabetes
My lipids (cholesterol and triglycerides) are considered ideal.
I still have an inch and a half to lose off my waist to get to where my waist circumference is half my height and I’m guessing that will take me losing another 18 lbs but who knows? Whatever it is, it is.
I had a foot to lose from my waist when I started — so what’s an inch and a half more?
Now, “moving more” is possible! Yesterday, as I do most weekends, I walked for 2 hours and wasn’t tired at all. I work out each week doing slow High Intensity Training and love it and am thinking about joining a dance class in September. “Moving more” is the result, not the solution.
Keep in mind that my results are only relevant to me, as I am ”a sample-set of one” (n=1). As well, my doctor’s recommendations to me may not be the same as your doctor’s recommendations to you. Everyone’s results following a low carb diet will differ, because each person’s Meal Plan will be based on their own medical history, any metabolic conditions they may have, medications they are taking, their family risk factors, starting weight and lifestyle factors. What my journey and yours will have in common if you’re working with me is that it will begin as a moderately low carb intake, where you’ll be eating whole foods from all food categories, with your doctor monitoring your labs and the dosage of any medication that you may be taking. I’ll gradually lower the amount of carbohydrate you’re eating only as necessary to achieve the clinical outcome(s) that you’re seeking and with you doctor monitoring the dosage of any medications you’re taking. This often has to occur quite soon after lowering the amount of carbohydrate, and in time they may be discontinued entirely.
Some “low carb diets” available on the internet or in popular books promote unlimited amounts of meat, cream, butter and eggs and others promote (or promise) “rapid weight loss”. I don’t do either. But if you are looking for a Dietitian to support your desire to eat a low carb diet in order to lose weight and lower metabolic markers of Type 2 Diabetes, high blood pressure or abnormal cholesterol, then I’d be glad to be part of your healthcare team.
I have almost a decade of experience providing services via Distance Consultation (Skype and long telephone) and for those living in the Lower Mainland of British Columbia you can see me in-person in my Coquitlam office.
Do you have questions about how I might be able to help you?
Please send me a note using the ”Contact Me” form above and I will reply shortly.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
The LCHF-Dietitian website is preparing to celebrate a significant milestone; our 100,000th visitor in just over a year!
While I’ve been providing low-carb services to my clients for slightly over 4 years, the first three were through BetterByDesign Nutrition Ltd., my private practice located in British Columbia, Canada. It was when I began writing a blog about my own “n=1 experience” following a low-carb lifestyle (called “A Dietitian’s Journey”) that visits to the website took off; jumping from a couple of hundred people per day to 600-800 daily. So as not to overwhelm those coming to BBDNutrition’s website seeking support for food allergies and sensitivities, Irritable Bowel Syndrome (IBS) and healthy eating with articles dedicated to low carb, I decided to create a separate website, The LCHF Dietitian and there’s been no looking back.
Interest in “A Dietitian’s Journey” continued as I began to reverse my decade-long Type 2 Diabetes, lower my blood pressure and get lab work that showed my triglycerides and cholesterol becoming not only normal, but ideal. There was considerable interest in the “Science Made Simple” articles I was writing, where I explain the evidence-base for the use of a low carb or therapeutic ketogenic diet, complete with references.
I joined Twitter (@lchfRD) as a place to post a link to newly written articles but it was when I began to post pictures of food I prepared for myself and my family, that people began asking me for my recipes and it was at that point, the Food for Thought (blog) tab on my web page added a third section; Recipes. At present ~1200 people are following me on Twitter and it grows daily, depending what I post about. Some folks are very interested in the researched articles I write, others in the recipes and still others want to know about my continued weight loss or latest lab work, as posted in A Dietitian’s Journey.
Around the same time I joined Twitter, I created The LCHF-Dietitian Facebook page as another place to post links to new articles and much to my surprise, I now have ~430 people ‘like’ me there and 493 ‘follow’ me, with 40-60 new people per week “liking” the site.
I really don’t think I am that interesting!
I believe it’s the content on the site; the topics that I write about that brings people to my site initially. There is a huge interest in the LCHF lifestyle as a whole, and in the use of a therapeutic ketogenic diet. People are looking for credible information. I believe that I provide that.
I think once people have read through some of my content, they feel comfortable approaching me to provide them with services; because they trust that they are going to get a Meal Plan designed specifically for them – for their needs, their food likes and dislikes and lifestyle, and designed to help them achieve their personal health goals.
I also think that me being a formerly obese Dietitian that has reversed my own Type 2 Diabetes*, high blood pressure, high triglycerides and cholesterol encourages people. Everyone is different, and they know because I repeat it often that their ‘journey’ will be different than mine, but in posting mine folks know that I understand the issues personally, as well as from a clinical perspective. I’ve been fat! I’ve been metabolically unwell! Yes, I do understand.
HUGE PERSONAL MILESTONE: It’s not only my HbA1C that is in the non-Diabetic range (<6.4 mmol/L / 115 mg/dl) but my fasting blood sugar is finally in the normal range too (averaging 5.3 mmol/L / 95 mg/dl over the course of the past month!). This morning for the first time EVER, my fasting blood sugar was 4.9 mmol/L / 99 mg/dl!!
Currently, there is a great deal of interest in all things “low carb”, so much so that in the last few months I’ve need to begin posting some of the articles that I wrote for The LCHF Dietitian web site on my regular web site, because I’ve had so many people contacting me there, asking whether I can help them follow a low carb or ketogenic diet.
So, it’s come full circle.
I have always believed that nutrition is “better by design” which is how I came up with the name for my private practice, and the web site that represents it. I also firmly believe that a low carb diet needs to be designed.
Some young adults with no clinical conditions and not taking any medication may do very well following a generic “low carb diet” online, but for adults and older adults with Type 2 Diabetes, hypertension, high cholesterol or triglycerides and especially taking medications, following a low carb diet they found on the web can put them at significant risk. If you fall into this category, please read this article.
A low-carb diet is BetterByDesign.
Do you have questions about how I can help support your own ‘journey’ back to health? Please send me a note using the Contact Me form above and I will reply as soon as I am able.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Last night, Dr. Andreas Eenfeldt, the founder of Diet Doctor posted on Twitter that they had just updated their “Success Stories” page – encouraging people to;
“have a look at some of the most amazing and inspiring personal stories from the over 600 that we have published.”
I clicked on it, only to discover that my story is 5th in the women over 40 category! There are many incredible stories there, but perhaps what makes my story so popular, is that I am a formerly obese Dietitian.
For those that haven’t yet read my story yet, here is the summary of my progress from March 5, 2017 to March 5, 2018, as it appeared on Diet Doctor on March 14th, 2018;
While my weight loss plateaued for a month as I had begun my resistance training program (gaining muscle and losing fat) my weight loss has resumed once again. This “Dietitian’s Journey” will continue as I have not yet reached a low-risk waist circumference (one where my waist circumference is half my height). I still have to lose another 3 inches to lose (having already lost 8 inches!), so however many pounds I need to lose to get there, is how much longer I have to go. I am guessing that will be in about 20-25 pounds which may take another 6 months or so, but I’m not really concerned about the time because this “journey” is about me getting healthy and lowering my risk factors for heart attack and stroke, and any amount of time it takes is what it will take. It took years to make myself that metabolically unhealthy and it will take time for me to get to a healthy body weight and become as metabolically ‘well’ as possible.
Although I am a Dietitian, I have to lose weight and lower my blood sugar the same way as everyone else does; one pound and one meal at time, but it can be done!
It has been slightly over 10 years since I was diagnosed as having Type 2 Diabetes, and while it may not be possible to reverse my Diabetes because it has been this long, based on the clinical data I’ve seen I will be able to achieve complete and long term remission of symptoms provided I keep doing what I need to do once I achieve it. This is a lifestyle, not a “diet”. My health and quality of life depend on it.
While I may not be able to reverse my own Type 2 Diabetes, I get the joy (and privilege) of helping those who have been more recently diagnosed work on reversing theirs . Equally rewarding is helping those who have been diagnosed as having pre-Diabetes from ever getting that diagnosis!
If you would like to know how I can help you in this regard, please send me a note using the Contact Me form on this web page and I’ll be glad to answer your questions.
Meanwhile, be encouraged. If I can do it, so can you. You can read my one-year anniversary post here.
Note: I am a "sample-set of 1" - meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating "low carb" and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
For the last month I haven’t lost any weight and on top of that, my HbA1C went up a bit (from 6.4% to 6.5%, despite the fact that I’m eating the way I’m supposed to, tracking my macros and exercising. Like anybody else, I was a little discouraged. Defeating discouragement often involves me asking myself what I would I say to a client who was in the same position.
My “Dietitian self” reminded “me” that March 5th, at the beginning of my second year living a low-carb lifestyle, I began resistance training and have been doing it regularly since and muscle weighs more than fat.
In fact, 5 lbs of fat and 5 lbs of muscle take up very different amounts of space, and I’ve certainly lost “inches” this last month, especially off my abdomen. Loss of fat from deep inside my gut is very likely related to loss of the dangerous and metabolically active visceral fat (the fat around my organs and in my liver). This is good! At the same time, I’ve gained significant amount of muscle on my arms and legs that I can feel.
So what happened to the fat?
Here is the Science Made Simple explanation:
The fat (triglycerides) in my liver was broken down into glycerol and free fatty acids and the free fatty acids were then moved into my blood and sent to my tissues, which used them for fuel. Since I have been eating a ketogenic level of carbohydrates for approximately 5 months now, my main fuel source is fat and ketones.
The mitochondria in my tissues broke the free fatty acids down using a process known as β-oxidation and the end result is a product called acetylCoA. This acetylCoA was used in a metabolic pathway called the Citric Acid Cycle to make an interim source of energy called NADH2 which then went to the electron transport chain in my mitochondria (the powerhouse of the cells) where it was made into ATP, the energy that the entire body runs on.
Once the glycogen in my muscles was all used up and as I continued to exercise to muscle failure, ketones were made from the AcetylCoA and used as fuel in the mitochondria of all my organs, including my brain. The brain always has some glucose uptake but that can be made from the same source as the glucose used to maintain blood sugar; from the breakdown of amino acids from protein and the breakdown of fatty acids.
So is that why my blood sugar went up?
When I am doing High Intensity Training (lifting weights very slowly until muscle failure) my body first uses up all the glycogen stored in those muscles.
(Remember, glycogen is the short-term storage location for energy.)
As I keep exercising faster than my body can produce energy via the electron transport chain in my mitochondria, lactic acid builds up. This lactic acid goes to my liver and makes pyruvate which gets converted to glucose – and it’s this glucose which raises my blood sugar. Ahhh, yes. The good ‘ol Cori Cycle and gluconeogenesis (literally “making new glucose”).
During the last month, I lost approximately 5 pounds of fat and gained about 5 pounds of muscle which I estimated from the visible amount of fat lost mostly from my abdomen (also from other areas), and the amount of muscle I gained over the same time period.
Above is a representation of what those 5 pounds of fat looks like in a garbage can – where they belong, not around my organs!
To see the approximate 5 pounds of muscle I gained, I took a ‘selfie”. Not great, but compared to what I looked like before I changed my lifestyle, it’s certainly an improvement. I’m a work in process.
In case I forgot what I looked like before I changed my lifestyle, yesterday I found a picture of myself barbecuing out back from a year and a half ago.
This photo is quite the glaring reminder of what I looked like before I adopted a low carb lifestyle (Mar 5 2017).
…and here is the thirty pounds of fat (not counting the estimated 5 pounds of additional fat that I lost this month and gained in muscle) – also in a garbage can, where it belongs!
That is a lot of fat.
So, even if I can’t “see” the 5 pounds of fat that I lost this month on the scale, I can see it off my abdomen. At the same time, I can see the 5 pounds of muscle that I gained in the mirror and I weigh the same. The math is easy.
This isn’t ‘water’ loss, as I am well into my weight loss journey.
While I’m not thrilled that my HbA1C went from 6.4% to 6.5% during the last 3 months, it is explainable from the exercise that I am doing which breaks down glycogen to make glucose for my blood.
Increasing my muscle mass in time will make me less insulin resistant, eventually enabling me to lower my blood sugar more quickly after a meal. As well, as the visceral fat continues to be decreased, my liver should become more insulin sensitive, as well. This is both a good thing and a challenging thing. It is good, because it will enable my liver to take glucose out of my blood more efficiently than it can now, but it will be challenging, because the main role of insulin is as a storage hormone. If I eat more than my body can use, it will be stored again in my fat cells (both under my skin and the bigger problem; back in my liver and around my organs). I will develop the symptoms of Type 2 Diabetes again, and likely the high cholesterol and high blood pressure that I had before. That is why this is a lifestyle and not a “diet”. It’s easy to do something as if your life depends on it, when it does.
As long as I maintain the lifestyle I have adopted, I can continue to reverse the symptoms of my Type 2 Diabetes and despite the naysayers, this is a very sustainable way to live. One look at the Science Made Simple articles that I’ve written about the wide range of food we can eat, my food posts with pictures of some of the meals I’ve made and the range of recipes I’ve developed, one can see I am not being deprived and neither are others that follow a well-designed low carb eating style.
Much of what I do as a Dietitian in helping people be successful at losing weight and turning around symptoms of chronic disease is determining how much of which kinds of food will both provide them with the nutrients they need and also enable them to reach their weight loss and health goals. But I also provide coaching which supports people to be successful over the long term and this is very satisfying work. Sometimes ‘coaching’ may involve ‘tweaking’ their Meal Plan or helping them find some breakfast options or eating-out-at-restaurant options, and other times it is helping them understand why they haven’t loss weight and what approach might be best to turn that around.
Do you have questions about what’s involved with having me design a Meal Plan for you? Please send me a note using the “Contact Me” form located on the tab above and I will reply shortly.
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Waking up to discover that my story and first anniversary health improvements from “A Dietitian’s Journey” was featured on Diet Doctor today was better than coffee. So timely too, as today is International Dietitian’s Day.
For those that haven’t yet read the story yet (located here) this is a summary;
My one year summary as it appears on Diet Doctor (link below with Tweet)
My journey wasn’t a straight path as it took a little bit of time to figure out which type of low carb diet my body responded to best. I started out with a low carb high fat approach and a few months ago switched to a low carb higher protein approach, along the lines of what Phinney and Volek use with great results (more info on the type of low carb approaches here).
Perhaps you’ve heard people say that a low carb or ketogenic lifestyle is somehow ”restrictive”, ”imbalanced” or that it’s ”not sustainable. This new post titled “Low Carb or Keto – what can you eat?” shows pictures of some of the meals that I currently eat (following a low carb higher protein approach) and also posts links to recipes. You’ll see that it is way more diverse than slabs of meat and piles of bacon and eggs!
If you’ve considered getting started eating low carb or keto but would like personalized support, I can help. Whether you live locally (in British Columbia) or far beyond, I provide both in-person and Distance Consultation services via telephone or internet.
If you have questions, please feel free to drop me a note using the “Contact Me” form above and I will reply soon.
To our good health!
Joy
A Dietitian’s Journey – front page news on Diet Doctor – March 14 2018
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Last March 5th I wasn’t feeling very well. It had been ages since I had monitored any of the things that I was supposed to be keeping an eye on. I had Type 2 Diabetes (T2D) for ~10 years but hadn’t checked my blood glucose in close to 2 years. I had high blood pressure, which is common for those with T2D and even though I had a quality blood pressure monitor, I hadn’t used it in about as long as I hadn’t monitored my blood sugar. Needless to say, I also had not gone to have my glycated hemoglobin (HbA1C) checked in the same length of time which would have told me my average blood sugar the previous 3-4 months because I didn’t want to know the results. I was in classic denial and facts would interfere with my ability to keep ignoring it all. Denial is simply not thinking about something you know exists. The problem doesn’t go away – only your conscious awareness of it does. You just don’t think about it.
This time last year I felt unwell and went and took my blood pressure. The reading was so high it was incomprehensible. I waited and rested for 10 minutes and took it again, however it was not much better. It was so high that if I gone to see my doctor that day, he would have had me go to the hospital immediately, perhaps even by ambulance. Looking back, the responsible thing would have been for me to go to my doctor or to the hospital and ALSO changed my lifestyle but I knew what that would lead to; at least one or two medications for high blood pressure and they would have run blood tests at the hospital and then would have likely put me on at least one medication for Diabetes and on statins to lower my cholesterol, too and I didn’t want to do that (more denial). Two years earlier I already had blood sugar that was too high, cholesterol and triglycerides that were imbalanced and had blood pressure that was higher than it should be and was told by my endocrinologist that if I didn’t follow through with my plan of following the low carb diet that I had started at that point, that I would “be on insulin in 5 years, along with medication for high blood pressure and cholesterol“. While I had started with all the good intentions of continuing to follow a low carb lifestyle, I didn’t follow through and my health wasn’t going to get better on its own and I wasn’t living in such a way as to improve it. I was teaching others about the benefits of eating a low carb diet and helping them lose weight and lower their blood sugar and blood pressure and cholesterol but not actually doing it, myself.
My diet was well within the criteria of what Diabetes Canada says those with Type 2 Diabetes should eat; lots of whole grain, low glycemic index foods and since my meals were often below the 60 g of carbs at each of 3 meals and 45 g of carbs at snacks they recommended, I pushed the words of my endocrinologist into my sub-conscious and carried on. I cooked and ate all home-prepared foods, but avoiding the carbs inherent in a whole-food Mediterranean diet just seemed too difficult. I couldn’t get my head around eating shinglish cheese or hummus without whole wheat pita, or lamb brochettes without the bed of basmati rice underneath. Even though I was serving these foods with beautiful low carb vegetables they didn’t offset the constant flow of carbs every few hours.
I also lived with a secret sense of futility – that achieving a normal body weight when I was obese was simply unattainable. Why even try?
In October 2015, one of my girlfriends I had known since high school and who worked in healthcare dropped dead of a massive heart attack while alone at home. A few months later another girlfriend that I’d known since my early 20’s died suddenly from what I believe was a stroke – the Monday after the Friday she retired from 30 years as a Public Health nurse. My two girlfriends being in healthcare did not protect them from the ravages of chronic health conditions and cardiovascular disease, and last March 5th I realized that being a Dietitian with a post graduate degree wasn’t going to protect me either. I actually had to change.
That day I decided to do whatever it took to get well and live optimally and every day since then I’ve recommitted myself to that very same decision.
When I started this journey last year, this is what I looked like:
A Dietitian’s Journey – the road to better health (March 16 2017)
Now, I look like this:
taken at Belcarra Provincial Park, February 12, 2018
So far, I’ve lost;
32 pounds
8 inches off my waist
2 inches off my chest
3 inches off my neck
1 inch off my arms
1/2 inch off my thighs.
I no longer meet the criteria for Type 2 Diabetes
I have blood pressure that ranges between normal and pre-hypertension
I have ideal triglycerides and excellent cholesterol levels.
While I’m still overweight and have approximately another 20 pounds to lose to reach a healthy waist circumference, I am not as desperately unhealthy as I was this time last year.
I am alive, much healthier and committed to continuing this journey.
The last year’s journey was not a straight-forward path as one might think given I’ve taught a low carb lifestyle to my clients for the past 3 years, as it took a bit of time to figure out which type of low carb diet my body responded to best. Everybody’s a bit different. I started out with a low carb high fat approach and a few months ago switched to a low carb higher protein approach, along the lines of what Phinney and Volek use with great results (more info on the type of low carb approaches here).
Beginning Year Two
As I planned to do when I reached this level of health, this past week I began introducing exercise into the equation, but not what I did before (what people called “cardio”).
My focus is on building muscle tissue using slow high intensity exercise (slow HIT), following the protocol of Dr. Doug McGaff. This will have the benefit of improving my insulin sensitivity, and along with eating sufficient protein distributed through the day should enable me to continue to live an active lifestyle, as I age.
Last year I was given a ‘second chance’ and I am taking it!
To celebrate my one year anniversary, as a ‘present’ to myself, I bought a weight bench to use with my free weights and resistance bands, and have set it up in a corner of my room.
I’ve folded up the Nordic Track for now, but can open it up to use it should I want to later. I may resume morning walks now that the sun rises earlier, mostly as a way to reduce the muscle stiffness and start the day well – but building muscle mass is, by necessity, a priority.
Motivation for Change
My journey has never been about “looking good” but about being healthy and living optimally. While looking better is a wonderful side-benefit, it is just that – a bonus.
As a Dietitian, I’ve always believed that if people “go on” a diet because they want to lose weight and look better, they will eventually “go off” a diet because there simply isn’t enough internal motivation to continue. It is way too easy to buy the tempting food that is readily available all around us – all the more when our insulin levels are high and we’re always hungry.
To change long-term requires the motivation to change.
As one of my sons says “dying is bad” and since living, and living well was my motivation for changing my lifestyle, it continues to serve as my motivation every day since.
Like many of my clients, I was at a fork in the road and had a choice;
(1) to continue to live in denial about the seriousness of these conditions (high blood sugar, blood pressure and abnormal cholesterol / triglycerides)
or
(2) to face the reality that if I didn’t significantly change my lifestyle I would probably die from one of the chronic health conditions I already had, would get, or from one of the many metabolic results of having these conditions.
I made my choice a year ago and I don’t regret it for a minute!
Are you at a fork in the road – having to choose between continuing to do the same things that haven’t worked previously or like me, ignoring it all and doing nothing?
Perhaps you’ve been told by your doctor or specialists where making such a choice may lead and you ‘don’t want to go there’, but are overwhelmed thinking of making this kind of change on your own.
I can help. I provide personalized low carb and keto services both in-person in my office and by Distance Consultation (telephone, internet).
I have both the clinical knowledge and the personal experience that a low carb lifestyle is not only entirely ‘doable’, but is entirely delightful.
There are those that maintain it’s not sustainable long term, however I know many people that have been eating this way for 15 or 20 years and so that simply isn’t true.
UPDATE: This new post titled ”Low Carb or Keto — what can you eat?” shows pictures of some of the meals that I eat (following a low carb higher protein approach) and also posts links to recipes. You’ll see that it is way more diverse than slabs of meat and piles of bacon and eggs!
I like to compare my decision to pursue a low carb lifestyle to someone that gets diagnosed with a serious food allergy such as Celiac disease. They need to avoid gluten containing foods to live without damaging their bodies and I need to avoid carb containing foods for the same reason.
Few people diagnosed with Celiac disease will walk around their whole lives complaining about how “unsustainable” it is because for them, living itself or living in good health requires them to make this adaptation, and so they do. For me and for many of my clients, choosing to follow a low carb lifestyle enables us to put chronic health conditions into remission, so we make a similar type of adaptation.
Have questions?
Wonder how I might be able to help you? Please send me a note using the “Contact Me” form above and I will reply soon.
Note: I am a "sample-set of 1" - meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating "low carb" and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
March 5, 2018, it will be one year that I’ve been following a low carb lifestyle and today I took stock of what I’ve accomplished so far and set goals of what I will accomplish this coming year.
(4) a waist circumference in the ”at or below” recommended values of the Heart and Stroke Foundation
…and I wondered aloud in one of the first blogs in my ‘journey’;
“Will I meet all these goals? Who knows?! But I won’t know if I don’t try and the alternative of a life of medication for blood sugar, blood pressure and eventually cholesterol too does not appeal to me!”
Well, its a year later and what have I accomplished?
(1) My HbA1C is below the cutoffs for a Diabetes diagnosis and much of the time my fasting blood glucose is as well.
(2) My blood pressure is in the normal range for someone with Type 2 Diabetes and half the time it is in the normal range for someone without it.
(3) I have normal / ideal HDL cholesterol and triglyceride levels and my LDL is in the normal range.
(4) I have a waist circumference that is within the recommended range set by the Heart and Stroke Foundation.
This is good, yes and I am pleased with my progress but I am not content to pat myself on the back, buy a new outfit and rest on my laurels. I have things I still want to accomplish and towards that end, I have set some new goals for the coming year – year two in A Dietitian’s Journey.
I have updated the above goals for this year. I want to have;
(1) HbA1C that is in below the high end of the normal range (i.e. < 5.5 % instead of 6.0%) and to consistently have fasting blood glucose that is also below the high end of the normal range (i.e. ≤ 5.0 mmol/L | 90 mg/dl instead of 5.5 mmol/L | 99 mg/dl),
(2) blood pressure that is in the normal range for healthy adults without Diabetes,
(3) normal to ideal triglyceride and cholesterol levels – as good, or better than currently,
(4) a waist circumference to be half my height based on research covered in an earlier article,
(5) I want to be fit.
So what is “fit“?
I think that most people think of fitness in terms of what is usual for people of the same age and gender. If that’s the case, I definitely do NOT want that!
I want to be fit enough to shovel the snow off my driveway without needing a break. I want to be fit enough to carry in two 20 kg bags of salt myself – one in each hand. I want to chop the firewood for my fireplace and stack it myself and I want to be able to change the tire on my car myself, if need be. I can do those things now, but I want to keep being able to do that as the years go on. I don’t want to be one of those “women of a certain age” that sit in a chair doing “seniors fitness”! I want to be able to manage a resistance or weight training workout of women half my age, when I am in my 60’s and 70’s. Heck I want to live a full and productive life like I do now, when I’m “old”.
My grandmother and I
My grandmother lived until the age of 104 years and was in good health until a few months before she died and like many seniors, it was a ‘fall’ that began the health failure cascade that eventually ended her life.
If I begin strengthening my muscles now, I won’t become one of those frail seniors with spindly little legs. That’s what I mean by “fit”.
With the encouragement of a few doctors that I know that are quite a bit younger that I am, but considerably more knowledgeable in this area, I’ve decided to get fit following two main recommendations;
(1) eat sufficient protein to prevent sarcopenia, the visible loss of muscle mass and strength that is commonly associated with aging
and
(2) to practice high intensity training (HIT) to build up my muscles, so that they are the healthiest they can be for my age.
Something I have learned by listening to the lectures of Dr. Donald Layman (on protein requirement as we age) and to Dr. Doug McGuff (on strength training for health and longevity) is that what is common as people age is not what is normal.
It is common in our society to see older adults with muscle loss, however when we look at seniors in other cultures, this is not normal.
Okinawan senior woman, farming
The seniors of Okinawa, Japan for example continue to do manual jobs and practice martial arts well into their 80’s and 90’s and the aborigines of Australia remain lean and fit as seniors.
Aborigine senior
This is “normal“.
We’ve confused “common” with “normal” and instead of visualizing seniors exercising looking like this;
Okinawan man practicing karate
…all too often, we picture this:
“seniors exercising”“Weight training in your twilight years” – Global News
An article last year on Global News titled “weight training in your twilight years” had the picture to the left accompanying it – as if all one can reasonably expect from a woman in her 60’s is to be able to lift a 1 pound weight.
No, that is not fitness.
…which brings me back to my last goal. I want to be ‘fit’ the way it is normal to be fit – not what is commonly viewed as fitness for “women of a certain age”.
I want to eat optimally and function optimally because anything else is less than what we were created to do and be. This means continuing to eat low carb because as someone who met all the criteria for Metabolic Syndrome, including obesity, Type 2 Diabetes, high blood pressure and high cholesterol, this is what it will take to keep those diseases and disorders in remission. It also means strength training my muscles and eating sufficient protein to accrue new muscle – not to become a body builder, but to be a fit woman.
Final Thoughts…
In the lecture given by Dr. Doug McGuff on strength training for health and longevity that I watched, he told the story of Satchel Paige (1906-1982), considered the best pitcher in baseball history and who began pitching at the age of 42 years.
One of the quotes he is renowned for happens to hang on the wall in my client bathroom and reads;
“How old would you be if you didn’t know how old you are?”
– Satchel Paige
My grandmother was often mistaken for a woman 20 years her junior right up until the last year or two of her life because she didn’t “act old”. She lived in an apartment for seniors and cooked her own porridge each morning and in good weather walked to the local shopping center two blocks away until she was a centenarian.
I want to be that kind of senior!
And so, as I close off the first year of A Dietitian’s Journey, I begin the second with goals having been met and new ones to be achieved.
So let me ask you this, “how old would you be if you didn’t know how old you are?”.
Have questions about how I can help?
Please send me a note using the “Contact Me” form above.
To our good health!
Joy
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
A month ago I made some changes in the macro distribution of protein to fat in my Meal Plan which has resulted in some significant progress in terms of weight loss, as well as inches lost.
Weight loss since increasing ratio of protein:fat
I knew that my weight had been decreasing about 1/2 pound a week over the previous several months, and in only the last month I had lost 7 pounds and an inch off my waist since I had increased my protein to fat ratio – that’s more than 1 1/2 pounds per week!
Over the long weekend, one of my sons took a cell phone picture of me when we were at Burrard Inlet, and he took a few to make at least one came out. This was a good thing because I would have thought that maybe it was just one photo or the camera angle that made me look slimmer. No, it wasn’t the camera angle, but the change in my weight over the last few months. It wasn’t until I saw a picture of what I looked like that I could ‘see’ it more objectively.
Here is the photo:
photo taken February 12 2018
When I got home, I remembered that in October I was out at the same location and had a photo from that day. That was 7 months into me following a low carb / ketogenic lifestyle.
I also had a photo of me from 2 1/2 years ago (taken around the time I first learned about the clinical benefits of following a low carb lifestyle) that was also taken in the same location.
Here are those three photos side by side:
Me on the left 2 1/2 years ago, 4 months ago in the middle, on the right now
I am not yet at my goal weight – which will be when my waist circumference is half my height, but I am well on my way. For me, changing the ratio of my ‘macros’ (short for ‘macronutrients’ i.e. protein, fat, carbohydrate) has helped overcome a slow and often stalled weight decrease.
Currently, what is working very well is for me is for me to plan my meals around getting sufficient protein and what is ‘sufficient’ is based on research regarding what older adults need to prevent sarcopenia (loss of muscle mass) as they age, as well as to continue to build muscle mass which helps improve insulin sensitivity.
Instead of focusing on how much and what types of fat are in my meals, I now set my attention around getting my individual need for 1.5 g protein / kg of ideal body weight. I eat the natural fat that is found in my protein source (skin on fatty fish or chicken, yolk in egg, etc.) but don’t ‘add’ much fat to my meals, except for maybe a little olive oil on salad. I eat the carbohydrates that come naturally in non-starchy vegetables and the nuts and seeds that I regularly eat, up to my carbohydrate maximum (or “carb ceiling”) for the day. For me, based on my significant degree of insulin resistance, this is working very well – but everyone is different.
My Meal Plan looks different than the Meal Plans I design for my clients because we all have different needs. Some people are overweight but insulin sensitive, others are normal body weight and insulin resistance and many already have Type 2 Diabetes (T2D). Even comparing my Meal Plan with those of my clients with T2D, mine is different because my ability to tolerate carbohydrate is very low. Think of the ability to tolerate carbohydrates for those who are insulin resistant like lactose intolerance to those who are lactose intolerant. Some people can drink some milk and be okay, whereas others are unable to tolerate even a small amount.
Something to keep in mind is that having a Meal Plan doesn’t mean it is ‘carved in stone’. Our physiological needs change as we lose weight and for those who are insulin resistant or T2D, as our level of insulin sensitivity improves over time which is why Meal Plans needs to be modified as weight loss progresses. As well, sometimes we benefit by a tweaking of the ‘macros’ (as I did with mine) to enable a more sustained and consistent weight loss.
Remember that everybody’s journey is different, because we all start from a different place.
As a result of the photo taken of me this past weekend, I have some thoughts about how we can use photos to chart our progress. While clinically, we measure our success in weight and inches lost and improved laboratory test results, often the way we as individuals can best recognize and celebrate our success is by seeing photos of ourselves over time. Don’t get me wrong, when I was obese I hated seeing photos of myself but now seeing them serves as a “sign post” of the progress I’ve made on my journey. Now, the very photos I detested I post on the internet for all to see, because I am now well on the road to much better health; with normal cholesterol and triglycerides, normal blood pressure and blood sugar levels that no longer meet the criteria for Type 2 Diabetes.
I certainly haven’t “arrived”, but today I take a moment to celebrate that progress, as I encourage my clients to do.
Have questions as to how I can help you achieve your health and nutrition goals? Please send me a note using the “Contact Me” form located on the tab, above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
As I’ve been saying from the beginning, my data is “a sample-set of one” (n=1), but yesterday data from 218 subjects that followed a low carb ketogenic diet for one year was published, so now I have something to compare my data with. Like the subjects in the study, when I began on March 5 2017, I was obese and had been diagnosed with Type 2 Diabetes more than a decade ago. The comparison between my results and those of subjects in this study is very encouraging!
Method Comparison
Carbohydrate Intake
Subjects in the study typically ate <30 g total dietary carbohydrates per day, whereas I ate 50 g of net carbohydrates per day which is approximately ~65 g of total carbohydrate per day for the first 5 months (more than double the amount of carbohydrate of those in the study). Most of these carbs came from berries and nuts.
It became clear through lab tests (fasting insulin along with fasting blood glucose) that I was quite insulin resistance and that level of carbohydrate intake was not providing me with the reduction in blood glucose I was seeking. It is only in the last 6 months that I lowered my carbohydrate intake to the level of those in the study and began to see significant progress.
Protein Intake
Subjects in the study had their protein intake targeted to a level of 1.5 / kg based on ideal body weight.
Until very recently, my protein intake was at 1.0 g / kg based on ideal body weight (which is at the minimum level of protein intake) and the bulk of my intake was from fat.
Vegetable Intake
Just as subjects in the study, I ate 3-5 servings of non-starchy vegetables per day.
My 11-month outcomes compared with 1-year data from the study
Blood Glucose Levels
At baseline, the average HbA1c level of participants in the study was 7.6% ±1.5%, with less than 20% of participants having a HbA1c level of <6.5% (with medication usage).
As I documented in my one-month update, I didn’t measure my HbA1C at baseline, but there are clinical calculators for estimating that from blood glucose levels. From laboratory tests, my fasting blood glucose the previous three years was 7.9 mmol/L (Feb 2013), 9.1 mmol/L (Sept 2014) and 9.7 (Aug 2015). Extrapolating that data to the start of my journey (March 5 2017) brought it to approximately 12 mmol/L. As documented in an earlier progress update, four months into eating low carb high fat, my fasting blood sugar was averaging 8.5 mmol/L.
Here is a graph of my blood sugar levels the first few weeks;
My blood sugar levels a month after starting my journeyAs can be seen from the graph, my blood glucose was at lowest at 7.7 mmol/L (see photo to the left) and I had spikes well above 10 mmol/L, and I was averaging around 8.5 mmol/L over the course of the day – which is slightly higher than the average of those in the study.
On average after 1 year, participants in the study lowered HbA1c from 7.6% to 6.3% — which is in the sub-Diabetes range. A month ago, my laboratory HbA1C came back at 6.4% and in the last month, I am averaging 6.33%.
My average blood glucose readings the last two weeks
My highest ‘spikes’ are just above 7 mmol/L whereas at the beginning they were closer to 10 mmol/L.
Weight Loss
At one year, mean body mass reduction of participants in the study was 12% of their initial body weight, with an average of 30 pounds lost.
Average Weight Loss at One Year [from Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study.]At only 11 months, my body mass reduction has been 17% of of my initial body weight, with 35 lbs lost. Even eating a much higher fat diet for most of my journey and more carbs for the first 5 months, my weight loss so far has been better than the average of those in the study.
Other Metabolic Markers
At 10 months, participants in study experienced a 20% reduction in their triglycerides levels and after one year, reduction in triglycerides was at 24%. After one year, LDL increased on average by 10% however HDL increased on average by 18%.
My triglycerides dropped from .95 to .64 from the last time I had them checked in 2015 (with no change in diet until March 2017), which is a decrease of 33%, which is even better than the average 24% subjects in the study obtained. My LDL dropped from 3.26 to 2.60, which is a decrease of 20% – even better than the average of 18% from the new 1-year study data.
My HDL was previously good as I ate a liberal carb Mediterranean diet and not a standard American / Canadian diet, so it only rose 3% (from 1.91 to 1.97) from the last time I had it checked, however with the drop in my triglyceride levels, my TG:HDL ratio is now 0.32 (with <0.87 considered ideal).
Eleven months ago, my blood pressure was 1/3 of the time in Stage 2 Hypertension with one hypertensive emergency (higher than Stage 3 hypertension!) with the rest of the time in Stage 1 hypertension. The last two weeks, my blood pressure is 50% of the time in the normal range for non-Diabetics to 50% pre-hypertension (which is considered the ‘normal range’ for those with Type 2 Diabetes) and I am off Ramipril. Except for stating that participants in the study had improvements in both systolic and diastolic blood pressure, no data was provided, so no comparison is possible.
Conclusion
Even eating almost double the amount of carbohydrates as those in the study ate for the first 5 months, my weight loss and improvements in blood glucose levels the last 6 months enabled me to match or exceed the results of those in the study!
On average after 1 year, participants in the study lowered their HbA1c from 7.6% to 6.3% and I lowered mine from 8.5% to 6.3% after 11 months.
Average weight loss in the study during the first year was 12% of body weight which on average was 30 pounds and my weight loss has been 17% of my body weight with a 35 pound weight loss, in 11 months.
My triglycerides decreased 33% which is even better than the average 24% in subjects in the 1 year study.
My LDL decreased 20% which was also better than the average of 18% from new 1-year study data.
My blood pressure was dangerously high 11 months ago and today is in the normal range for someone with Type 2 Diabetes and half the time is in the normal range for someone without it.
Finally here are two additional ways that I can measure my success to date;
Early this morning, my fasting blood glucose was 5.3 mmol/L (95 mg/dl) which is in the normal non-Diabetic range. This is a first! This was without taking Metformin.
At 10:20 AM while still fasting (today in an intermittent fast day for me), my fasting blood glucose is still 5.3 mmol/L (95 mg / dl) – also with no medication.
This is my body maintaining a stable non-diabetic fasting blood glucose level – which means my liver is not over-synthesizing new glucose (gluconeogenesis)
This is huge progress.
Up until now, my liver and muscle was so insulin resistant that my liver just kept making more and more glucose (via a process called gluconeogenesis).
Normally, the hormone insulin stops excess glucose production by stopping glucagon secretion by the pancreas (alpha cells), but I was SO insulin resistant, glucagon would be released telling my liver to make more glucose!
The fact that my fasting blood sugar has been stable for so many hours, means my liver is starting to respond to signals correctly. My liver is maintaining my blood sugar at a normal level – without any medication. This is great news.
UPDATE: My morning fasting blood glucose the following morning was just as wonderful (5.3 mmol/L / 95 mg/dl), Feb 9) and my 2 hour post prandial blood glucose after eating a high protein low carb breakfast was also amazing (5.4 mmol/L / 97 mg/dl, Feb 9). That is, the above result was not a ‘one-off’ event but the start of becoming insulin sensitive!
Finally, here are two photos of me; one from March 2017 and one from February 2018 – taken 10 months apart. Using the width of my glasses as a reference, it is easy to see the decrease in the width of my face.
Goals compared with results
March 14, 2017, I set very specific goals that I wanted to achieve and they were;
I have a long way to go to get to my goals (plural) because I’ve set the bar very high…and why not? If the literature indicates that this works, then I want;
(1) blood sugar in the non-diabetic range
(2) normal blood pressure
(3) normal / ideal cholesterol levels
(4) a waist circumference in the ”at or below” recommended values of the Heart and Stroke Foundation
Will I meet all these goals? Who knows?! But I won’t know if I don’t try and the alternative of a life of medication for blood sugar, blood pressure and eventually cholesterol too does not appeal to me!
So join me in my journey — a journey of change, of good health and on a road less traveled.
It is 11 months later this is what I have achieved;
My HbA1C is below the Diabetic range and I am much of the time, I am able to maintain my fasting blood sugar in a normal, non-Diabetic range.
My blood pressure is in the normal range for someone with Type 2 Diabetes and half the time it is in the normal range for someone without it.
I have normal / ideal HDL cholesterol and triglyceride levels and my LDL is in the normal, but not ideal range.
I have a waist circumference that is ”at or below” recommended values of the Heart and Stroke Foundation (see photo , above).
A waist circumference in the ”at or below” recommended values of the Heart and Stroke Foundation for a Caucasian woman is < 35 inches
Three weeks after setting the above goals, I updated my waist circumference goal to be that I wanted my waist circumference to be half my height. This was based on a meta-analysis study from 2012 which pooled data from multiple studies with more than 300, 000 adults in several ethnic groups and which found that Waist to Height Ratio (WHTR) was a far better predictor than BMI or Waist Circumference of cardiovascular or metabolic risk factors in both sexes.
from Ashwell M, Gunn P, Gibson S (2012) Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev 13: 275—286
How to take Waist to Height ratio: Measure your waist at the location that is the mid-point between your last rib and the top of your hip bone, with the front and back of a flexible seamstress-type tape measure at the same height, and your belly fully relaxed, not sucked it in! Your waist circumference in inches should be half your height in inches.
Based on having a low-risk waist to height measurement, I still have to lose another 2- 1/2 inches off my waist. I haven’t yet “arrived” but I am certainly making progress in my own, personal health and weight loss journey.
Comparing my own results over the last 11 months to the 1 year data of over 200 adults with Type 2 Diabetes who were eating a low carb ketogenic diet, I am doing at least as well, and in some cases, better. This is reason for me to be encouraged.
NOTE: There is no “one-size-fits-all” low carb / ketogenic diet and what works for me may not be what is best for you. Before undertaking a major change in diet, please discuss your plans with your doctor.
Have questions?
Wonder how a low carb / ketogenic lifestyle can help?
Please send me a note using the ”Contact Me” form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Hallberg, S.J., McKenzie, A.L., Williams, P.T. et al. Diabetes Ther (2018). Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. https://doi.org/10.1007/s13300-018-0373-9
NOTE: A “Dietitian’s Journey” is my “sample set of one” (n=1) personal story. My results following a low carb / ketogenic lifestyle are just that; my results. There is published scientific evidence of physicians discontinuing patient’s medication following adoption of a low carb / ketogenic diet, but this post should not be viewed as objective data. This is simply me documenting my own, personal journey. Do not discontinue any medication without first consulting with your doctor.
Three years before I adopted a low carb lifestyle, I was diagnosed by the head of Immunology and Allergy at a Canadian university with a relatively rare immunological condition known as Mast Cell Activation Disorder / Syndrome (MCAD / MCAS). I had numerous debilitating symptoms that are not unlike those that accompany other immunological / autoimmune disorders such as Lupis, Rheumatoid Arthritis (RA) and fibromyalgia – plus a few unique to MCAD (such as food and environmental sensitivities and pronounced flushing). According to the Immunologist, the MCAD was likely triggered from my exposure to toxic mould exposed in a basement repair in November 2012. I was prescribed a whole host of medications in order to manage many debilitating symptoms.
In April of 2013, my Immunologist prescribed two types of antihistamines (H1 and H2) in very large quantities, including Cetirizine HCL 10 mg (H1) 4 times a day and Ranitidine 150 mg (H2) three-four times per day in an effort to lower my body’s release of inflammatory products. The dosage of Cetirizine is 4 times the amount used for treating seasonal allergies and the dosage of Ranitidine was twice the dosage typically used for treating acid reflux. These medications were in addition to two tablets of diphenhydramine hydrochloride 25 mg (Benedryl) that I took every 4 hoursfour times per day. It’s amazing I could function at all, taking that much Benedryl, but I had no choice. I also needed to use a Salbutamol (asthma) inhaler four times per day to manage my environmental sensitivity to various odors, including laundry soap and the smell of certain foods.
In November 2013, the Immunologist prescribed Sodium Nalcrom 100 mg, a mast cell stabilizer in an effort to reduce and eventually discontinue taking all the Benedryl. I took 2 capsules of Nalcrom before each meal three times per day and 2 capsules at bedtime – a total of 8 capsules per day.
Sleep disruption is one of the inconvenient symptoms of MCAD, so I was prescribed Trazadone 100 mg before bed to assist with that.
I took all of these medications as prescribed above until shortly after I began eating a low carb diet in March of 2017.
Within 3 months of beginning to eat a low carb diet (~50 gm carbohydrate per day), I was able to take less and less Nalcrom – first dropping it in the morning, then at lunch time, but continuing to take it at supper and occasionally before bed.
After about 6 months eating low carb (still ~50 gm carbohydrate per day), I was able to reduce the Cetirizine to three times per day from four and was also able to reduce the Ranitidine from 3-4 times a day to twice a day. I stopped taking the Nalcrom completely. With the MCAD much better, I was able to lower my Trazadone for sleep to half.
Once I reduced my carbs further, down to 35 gm per day (in order to better manage continued high glucose readings), I was able to reduce the Cetirizine to twice a day and the Ranitidine to just once per day, at night (which at that point was more to manage GERD than for any symptoms of MCAD). I continued to take the Trazadone ~ 3 times per week as needed for sleep.
It’s been about 3 months since I stopped taking the Ceterizine completely and about a month since I stopped taking the Ranitidine. This left me with the “baby dose” of Ramipril 2.5 mg that I asked for in July 2017, as my blood pressure had begun to creep back up. When I saw my doctor in December, we discussed when I should discontinue the Ramipril, to which he said “when your blood pressure gets too low”. I asked him to give me a number, so I could continue to monitor it. He said, when it goes below 110 / 65 then you can discontinue it.
my blood pressure readings last night
Two days ago I felt a little light headed but didn’t stop to think it might be my blood pressure. I drank more water and carried on. Yesterday late in the afternoon (when my blood pressure is usually the highest) it was 119/79. I continued to monitor it in the evening, and it continued to drop to 112/63, 109/59, 100/59 and then back up to 108/60. Based on my doctor’s instructions to me, it seemed it may be time for me to discontinue the Ramipril. Last night I didn’t take it, but this morning I took 1/2 of it as I want to make discontinuing it gradual. I will take a 1/2 dose for a few days and keep monitoring my blood pressure to make sure my body is adapting to maintaining my blood pressure without medication
This morning as I anticipate putting the Ramipril container in the pile of discontinued medication that I have on a shelf in my closet, I realized just how big that pile is!
Pile of discontinued medication (excluding the Benedryl which was discontinued before I began eating low carb)
I am not “cured” of MCAD, or of my Type 2 Diabetes, or my hypertension (high blood pressure) or GERD, or my abnormal lipids (referred to in my 11 month update). I am reasonably certain that if I began eating a high carb diet again, all, if not most of the symptoms I experienced previously would resume. I am in remission from these conditions and likely will remain in remission, provided I continue to eat low carb and continue to lose weight (until I achieve a low-risk waist to height ratio). The discontinuation of my past medications serve as “sign-posts” of my journey.
If you would like to know how I can help you on your own health and nutrition journey, please send me a note using the ”Contact Me” form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
A week or two ago, there was some discussion on a Twitter thread that some “wouldn’t trust a fat Dietitian” and yesterday I was told “once you get in shape then you can dish out advice” – as if my past or current health status makes me less credible or competent to counsel others. Both of these got me thinking, is a ‘slim Dietitian’ really more credible? What is a Dietitian’s credibility and competency based on?
There is no question that there is a ‘fat bias’ and am not arguing whether there should be or shouldn’t be, but what makes any clinician credible is the scientific evidence on which we stand. What makes me credible in teaching others to follow a low carb / keto lifestyle has nothing to do with my body weight; it has to do with the 76 studies with almost 7000 subjects over the past 18 years which provides the scientific basis on which I base my practice. What makes me competent to counsel is my education, as well as my experience in clinical practice.
I have a post graduate degree in Human Nutrition, am a published researcher and have over a decade of experience in private practice and my learning didn’t stop there. If it had, I would not have made the transition in thinking that I did approximately 3 years ago. It took a huge amount of research and reading and very strong scientific evidence for me to come to the conviction that what constitutes best-practice in helping people address overweight, obesity and insulin resistance, including Type 2 Diabetes is following a low carb / keto lifestyle. I continue to spend most of my free time reading scientific studies in order to more fully understand the strength of the evidence on which my clinical practice is based.
Competence is the ability to achieve a desired result and my ability to help others lose weight and lower their metabolic markers is independent of my body mass. My competence is dependent on the scientific research.
My current body weight does not make me less competent to counsel others. I am a “sample set of one” (n=1) and my personal health and weight-loss journey is just that – personal, anecdotal evidence. It encourages my clients and those that read my articles that I actually understand what is involved in living a low carb / keto lifestyle, and when I say that it can be done fairly easily and over the long-term, I know this first-hand.
Someone pointing out that I am not skinny is not news, as my past and current health status is on my web page and plastered all over the internet in Technicolor, for all the world to see. But, eleven months ago, I was an obese Dietitian with a host of metabolic issues including Type 2 Diabetes, hypertension, dyslipidemia, high visceral adipose, etc.). I was the poster woman for Metabolic Syndrome. I started “practicing what I preach” and the results speak for themselves.
My progress is well documented, I’ve lost 35 pounds, 7½ inches off my waist and have only 2 ½ more inches to lose to achieve an ideal waist to height ratio. I am in partial remission from my Type 2 Diabetes, have almost normal blood pressure and have a lipid profile that is considered ‘ideal’, and no longer take medication for chronic gastroesophageal reflux disease (GERD) – something I have done for years.
If you want to read the technical details of my progress, you can read this article.
…and I have the mirror.
Eleven months ago (March 16 2017), this is what I looked like;
March 16 2017
Today, this is what I look like:
January 28 2018
Sure, I still have 15 pounds to lose to be in the normal weight category and probably closer to 25 pounds to lose to be at my ideal body weight and waist circumference, but eating low carb isn’t a ‘diet’ for me, but a permanent change in lifestyle. It has to be because of the degree to which I have become intolerant to more than a small amount of carbohydrate. I just need to keep doing what I am doing and continued improved health and appearance will come. This is my journey.
If you would like to know how I can help you on your own health and nutrition journey, please send me a note using the ”Contact Me” form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Sometimes a photo can say more than all the words in the world.
The two photos below are a comparison of me 11 months ago and today. I certainly haven’t “arrived”, but like any journey there are markers along the way – markers that you are headed in the right direction, markers as to how far you’ve come and markers as to how far you’ve left to go. This photo is such a marker.
Me – 11 months ago (left) and today (right)
Everybody’s road to better health is different and “A Dietitian’s Journey” tells mine. You can read my story from the beginning with all the ‘gory details’ – from my “fat pictures”, to my lab work, and everything in between. It tells the story of my struggle with denial and how the pain of remaining the same was greater than the pain of changing, and so I changed.
I keep making small, corrective changes in my path to ensure that it time I arrive at my ‘destination’ – which for me is to have a waist circumference (in inches) that is half my height (in inches). This is not an arbitrary goal based on vanity, but is based on me having the lowest risk of cardiovascular events (heart attack and stroke), given my lab work continues to improve, as time goes on.
A summary of where I am on this journey now is here.
If you have questions as to how I could help you achieve your own health and nutrition goals, please send me a note using the “Contact Me” form on the tab above.
My journey began on March 5, 2017 when I was a fat Dietitian with all the benchmark symptoms of Metabolic Syndrome including Type 2 Diabetes, high blood pressure, high LDL cholesterol and triglycerides, abdominal adiposity (i.e. “a belly”) and high BMI (high weight for height). Physically I was a mess but my biggest problem was that I was in denial. It had been months since I had monitored my own blood sugar or blood pressure even though I had been diagnosed with Type 2 Diabetes 10 years earlier. I knew better.
I would occasionally step on the scale and weigh myself, but how my clothes fit (or didn’t) already told the story. I was overweight. Actually, I was obese.
Shortly before my own turning point in March 2017, I had two girlfriends my own age – one who I knew since high school and one since university die of preventable diet-related disease within two months of each other. Both were in healthcare and took care of others practicing their profession, just as I do. I had two degrees on the wall but didn’t take care of myself.
March 5, 2017 all that changed. That was the day that the pain of remaining the same became greater than the pain of changing. So I changed. That story and the progress since then are in previous articles in A Dietitian’s Journey.
Like many others, I once believed that “Diabetes is a chronic, progressive, disease” and that it will only get worse in time. I realize now that if I had continued to eat more carbs than my body could handle, then it most certainly would have gotten worse but I have almost 11 month of evidence that supports that if I don’t, it CAN and DOES get better.
I am not “cured” by any means, but my symptoms are now in what the American Diabetes Association defines as partial remission and I may very well be able to achieve full remission, as I continue to eat a low carb diet. I will only know in time.
To achieve remission with Type 2 Diabetes (T2D) is like someone being in remission with Celiac disease; we can get well and stay well provided that we don’t eat the foods that we can’t tolerate; for a Celiac that’s gluten and for someone with T2D it is more carbohydrates than their body can handle.
I do eat some carbohydrate each day, mostly as non-starchy vegetables, the occasional berries or pomegranate seeds on a salad, as well as some nuts and seeds but I am careful to keep the amount at any one time below what my body can process while maintain blood glucose control as close to a ‘normal’ (non-Diabetic) level as possible.
This article explains how and why my body is no longer able to handle more than a small amount of carbohydrate at a time.
The good news is that I no longer meet the criteria for diagnosis with Type 2 Diabetes, as demonstrated by the Diagnostic Criteria[1] for the disease:
It does not appear that Diabetes Canada define these concepts, however the American Diabetes Association (ADA) defines “remission” as having test results below the range for Diabetes (i.e. Fasting Blood Glucose less than or equal to 5.5 mmol/L (100 mg/dL) without taking Diabetes medications or having bariatric surgery.
“Partial remission” according to the ADA is having test results lower than the range for Diabetes i.e. Fasting Blood Glucose less than or equal to 5.5 – 6.9 mmol/L (100—125 mg/dL) or HbA1C between 5.7 — 6.4% for at least 1 year.
my Fasting Blood Glucose is less than or equal to 7.0 mmol/L , so I no longer meet the diagnostic criteria and fall in the partial remission range. As you can see from the following picture, the average of my twenty-four Fasting Blood Glucose readings from January 1 2018 – January 24, 2018 has been 6.0 mmol/L. Out of the 24 glucometer readings (with a meter that I standardized with the lab when I had my tests done), only once was my blood sugar higher than the cutoff. This would indicate that I am in partial remission, by the ADA definition.
Self monitored blood glucose – January 1 2018 – January 24, 2018 – averages
I have taken seventy-five glucometer readings during the month of January so far (see photos at the bottom of this article) and none of them were greater than or equal to 11.1 mmol/L. Here is a graph of my January results:
Self monitored blood glucose – January 1 2018 – January 24, 2018 – graph
3. My 3 month glycated hemoglobin test, also known as a HbA1C (or “A1C” for short) is less than or equal to 6.5 % which means that I no longer meet the criteria for the disease and my results fall in the range for partial remission.
Glycated Hemoglobin below criteria for Type 2 Diabetes – January 23, 2018
Cholesterol and Lipids
My LDL was at the high-end cutoff two years ago, after only 4 months on a low carb high healthy fat diet, it was approaching what is considered by the existing / popular standards of ”optimal LDL” for someone who is high risk (family history of cardiovascular disease).
My LDL was 2.60 mmol/L (1.14 mg/dl), my triglycerides (TG) were 0.64 mmol/L and my HDL was 1.97 mmol/L.
Using more significant measures, my TG:HDL ratio was 0.32 (with <0.87 considered ideal). A very low TG:HDL ratio is associated with lots of large, fluffy LDL — the kind associated the lowest risk of cardiovascular disease (CVD) such as heart attack and stroke. It is the higher density, small LDL particles that are associated with CVD.
Blood Pressure
My blood pressure has been ranging from between just below the normal range to pre-hypertension for months, but to protect my kidneys I am continuing to take a ”baby dose” of Ramipril® (2.5 mg per day) that I asked the doctor to put me on until my blood pressure is consistently below normal and the meds need to be reduced or discontinued. The dose I’m on is the smallest it comes in and my doctor has switched me to tablets, which can be split if my blood pressure is consistently on the low side.
Weight and Waist Circumference
Weight
I’ve lost 35 pounds. I feel better about how I look than I have in many years, and I am a little more than half way there. I am celebrating my progress, but not letting it be ‘enough’ because health-wise, it isn’t. To truly reduce my risk of heart attack and stroke, I need to lose another 25 pounds, or whatever weight will actually put my waist circumference at half my height.
Waist Circumference
I’ve loss 7 inches off my waist. That’s more than 1/2 a foot! Crazy, eh? I only have another 3 inches to lose off my waist for me be in the low-risk category and I am guessing that will correlate to another 30 pounds of weight loss. Maybe it will be less, maybe more, but my weight loss goal is whatever it takes for my waist to be half my height. The scale won’t determine my goal, the tape measure will.
My hard earned success in achieving partial remission from Type 2 Diabetes and these significant improvements in metabolic markers would be very short-lived if I began to eat more carbohydrates than my body can handle. I am still learning how much of which kinds of foods I can eat while maintaining my blood glucose levels but my own “n=1 results” seems to indicate that full remission of Type 2 Diabetes may very well be possible. The literature seems to support that it is possible- but whether I can achieve that level has yet to be seen. I still have much more to achieve, but I am definitely on the road to better health!
If you would like to know how I can help you on your own health and nutrition journey, please send me a note using the “Contact Me” form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
P.S. For those that would like to see the “numbers” to understand my progress to date, below are 10 photographs showing all my glucometer readings since March 5, 2017 until today.
Blood Glucose Mar 5 2017 – January 24 2018 – pg 1
Blood Glucose Mar 5 2017 – January 24 2018 – pg 2
Blood Glucose Mar 5 2017 – January 24 2018 – pg 3Blood Glucose Mar 5 2017 – January 24 2018 – pg 4Blood Glucose Mar 5 2017 – January 24 2018 – pg 5
Blood Glucose Mar 5 2017 – January 24 2018 – pg 6
Blood Glucose Mar 5 2017 – January 24 2018 – pg 7Blood Glucose Mar 5 2017 – January 24 2018 – pg 8Blood Glucose Mar 5 2017 – January 24 2018 – pg 9Blood Glucose Mar 5 2017 – January 24 2018 – pg 10
References
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212, Chapter 3
As I wrote about in a recent article, there’s more than one way to eat a low carb ketogenic diet including (1) low carb high fat (2) low carb high protein and (3) a mixed approach of higher protein lower fat during weight loss, then a moderate protein high fat during weight maintenance. Up until very recently my approach with my own weight loss has been low carb high fat – with the focus on monounsaturated fats such as olive oil, avocado oil, nut and seeds (and their oils) and omega 3 fatty acids from fatty fish. The problem has been that the last while, my weight loss and the rate at which my blood sugars were coming down has been too slow. As I do with my clients, it was time for a different approach. Since both of the other two types of low carb diet involves higher protein and lower fat I knew this is what I needed to do, but how much protein? How much fat? Do I keep carbs the same or lower them? In answering these questions, I have achieved a major breakthrough in my own ‘journey’ to better health.
I started with carbs. In discussion with my endocrinologist, I knew she supported carbs at 10% or less of my intake so I calculated my needs based on my gender, height, weight, activity level and weight loss goal – just as I do for my clients, and then figured out how many grams of carbs I could have in a day at this level. It was even lower than the amount of carbohydrate that I had been eating (which had been lowered twice over the last 10 months – from moderate, to low and now to very low), but since this ‘very low’ limit was in line with what my endocrinologist recommended, I set my carb limit at that.
Protein, rather than fat had to be the second macronutrient I needed to set and since it was to be based on lean body mass and not my total weight, I determined my fat percentage. Then, I calculated how much protein I needed to eat per day based on the research studies. As it turned out, the lowest end of the range was considerably more than I had been eating, and only just slightly higher than what the average Canadian or American eats in a day. This was a bit of an obstacle for me, as I am not a big egg eater also not a big red-meat eater and there’s only so much chicken I can handle. I knew I wanted to continue to eat a few ounces of cheese every day as this is a major calcium source, but that meant factoring in the fat the cheese would add, which I did. Nuts again cropped up as a significant problem – not for their carb content, as much as their fat content. Eating lower fat and higher protein meant nuts and seeds were going to be limited to a sprinkle on a salad and cream in my coffee was limited to a little bit once a day. I needed to look at option that would work for me in terms of protein and since I don’t eat pork or shellfish, that left me focusing on freshwater and sea fishes as well as finding ways to include beef and lamb along with different kinds of poultry.
Even though I live on the West Coast, there are many kinds of fish available to me to eat besides the ubiquitous sockeye salmon and halibut. I began exploring what was available frozen and rediscovered sea fishes such as whole mullet, mackerel and milkfish, fresh water fish such as whitefish, as well as the bags of filleted cod for quick preparation (I avoid basa and talapia because they are high in omega 6 fat, which makes them pro-inflammatory). I cooked a whole salmon on Friday and have been eating the leftovers cold for breakfast, since I am not that fond of eggs.
I began to think of poultry beyond chicken and bought and roasted a turkey (which also left leftovers to eat for my early meal) and began to think of ways to cook quail and duck (minus all the fat).
Eating a wide variety of fish and poultry with some cheese thrown in there has provided me with sufficient protein on most days and for the occasional time that I just can’t handle eating more, I mix some cocoa powder with whey isolate and drink that.
I should add that when I eat, I am not trying to 'fulfill' my macronutrient distribution (gms of protein, carbohydrate and fat) but rather, I eat as much whole food protein at my two meals (one mid-morning and the other around supper time) then eat a good 2-3 cups of low carb veggies with the protein. I add a little bit of mayo, butter or cream to make things taste good, and don't "count" anything except carbs. In fact, I encourage my clients to do likewise. I focus on maximizing whole food protein within my Meal Plan and the fat that I end up with is what naturally comes with those. It's a very "easy" lifestyle to follow, once the calculations are done - and since I do those for my clients, it only makes sense for me to do them for myself, too. Leading by example, right?
The results have been astounding.
I’ve lost 4 pounds in 2 weeks and as significantly, I have seemingly lost most of it off my abdomen and not just the fat under the skin (sub-cutaneous fat), but the fat deep in my belly, around my organs (visceral fat).
This is HUGE because it visceral fat is most highly correlated to insulin resistance – which is what I am trying to reverse. Just look what’s happened to my blood sugar over the weekend:
My fasting blood sugar actually went down after it went up in the wee hours of the morning (the effects of Dawn Phenomena) which would seem to indicate that the loss of belly fat is indeed making me more insulin sensitive! When my early morning blood sugar goes up due to Dawn Phenomena, my cells are now more responsive to the resulting spike in insulin, and the excess sugar is now being taken into the cells, like it is supposed to!
This wasn’t a one-off thing either. This is what happened yesterday and this morning;
These changes cannot be attributed to the baby dose of Metformin that I’m taking before bed (which is lowering the magnitude of the Dawn Phenomena rise), but is reasonably related to the only other change that I have made which is the increase in the amount of protein I am eating (in grams) and the reduction in the amount of fat and carbs I am eating.
We do know that over time, the body gets adapted to the changes we make – whether dietary or exercise changes and that to continue to get results at the rate that we want, we need to change the approach. I do this in my follow-up approach with my client over their weight-loss and health journeys and it was necessary for me to this for myself, as well.
While it is much ‘easier’ for me to eat a lower protein, higher fat diet as these are the foods I prefer, my goal is to reverse the symptoms of Diabetes and put myself into remission (have normal fasting blood glucose and normal HbA1C long term).
”Let food be thy medicine and medicine be thy food.”
– Hippocrates
For me, while it is not the easiest of most natural way for me to eat, increasing the amount of protein, decreasing the amount of fat and limiting my carbs to those contained in non-starchy vegetables is allowing my body to heal in the ways in needs to – allowing food to be my medicine.
The question arises “was it the lower carbs or higher protein that has made the difference?”. I had tried a few times before to lower my carbs down to almost as low as I am now and to made up most of the extra intake (outside of my basic protein need) from fat, but this did not contribute as much to me not being hungry (i.e. satiety) as this higher ratio of protein with the rest from the same sources of fat (which is still “high” by most standards). So yes, it is partially due to the lower carb content, but reasonably to the higher protein content, as well.
My entire ‘journey’ has been (and is) about me doing whatever it takes to achieve my goals with a healthy and evidence-based diet and it’s hard to argue that with 30 years of combined research in this area that Phinney and Volek aren’t reliable in terms of evidence. It mades sense for me to do what they recommend, even it if isn’t the most “natural” way for me to eat.
My hope is that in time, when I am no longer insulin resistant, that I can switch over to a moderate protein high fat intake as Phinney and Volek recommend, but for now this is what is best because it is working and because it is in accordance with what my endocrinologist recommended, and under the supervision of my doctor.
The ironic thing is that most of my clients do really well on moderate to low carb restriction with a fairly high intake of monounsaturated and omega 3 fat and are content with their rate of progress which is great. For those that will need, in time, to make changes to the way they pursue a low carb lifestyle, I hope by me leading by example, it will be encouraging to them.
Tomorrow I am scheduled to have my HbA1C level checked which won’t factor in much of these new changes in blood sugar levels because the test looks at the amount of glucose which stays attached to hemoglobin (Hb) for the life of the red blood cell (i.e. glycated hemoglobin), which is normally about 120 days / 3-4 months. At my last test 3 months ago, my glycated hemoglobin was 7.0% and what I am ultimately aiming for is a HbA1C of <6.0%, which would be in the non-Diabetic range. Whether its this time or the next time isn’t really as significant is that it has been more than 10 months where I have diligently been working towards that goal.
I’ve successfully normalized my triglycerides and lipids and brought them into the ideal range and have substantially lowered my blood pressure – and both of these were done by diet alone. It will be interesting to see the effect of these diet changes on my HbA1C, as well as have some indication of how much more I have yet to do.
It’s all about progress, not perfection and significant progress is being made, as evidenced by this recent personal breakthrough.
If you’d like to know how I can help you achieve your health and nutrition goals, please send me a note using the “Contact Me” form on this web page.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Ten months ago, it was urgent. I had to make a choice between going on several types of medication to lower my crazy-high blood pressure, and high blood sugars, triglyceride and LDL cholesterol or to immediately change my lifestyle. I chose to change my lifestyle. This is a progress report, going into the final two months of my first year at this.
As with other changes we undertake, there are two ways to look at things; how far we’ve come or how far we have to go. I choose to look at my progress as both. I am certainly not “there” yet, but I am nowhere near where I was!
Back in early March of this year, when I faced my own personal health crisis, it had been two years since I had any lab work done and ages since I was monitoring my blood sugar myself, even though I was Diabetic for the previous 10 years. It really was a case of classic denial. I didn’t want to know how bad it was. That day because I didn’t feel well, I faced the truth. I took my blood pressure (multiple times, because I couldn’t believe the readings!!) and I took my blood sugar. My blood pressure was so high, for certain had I gone to see my doctor at that point, he would have prescribed at least one type of medication, maybe two. Suffice to say it was dangerously high.
My blood sugar back in March of this year was high, but what else could it be eating a carb-based diet. I had started eating low carb two years earlier, but life circumstances got in the way for a time and I failed to go back and pick up where I left off. As I could have predicted they would, things only got worse. My fasting blood sugar was between 13.0 mmol/L (234 mg/dl) and 9.0 mmol/L (162 mg/dl). That’s nuts!
I was obese (BMI > 30). I’d joke about being the “fat Dietitian” but it wasn’t funny. For the previous two years, I was teaching others to eat low carb high healthy fat in order to lower their weight and reduce their insulin resistance, but I was in classic denial when it came to myself. Yes, I knew I was fat, but I was in denial as to just how much risk I was at for a heart attack or stroke.
My LDL was high and even though my high HDL acted as a protective factor, in the context of me being Diabetic, obese and having very high blood pressure, the only place it was going to go was higher – unless I changed my lifestyle permanently. That day I did. For me, there really can’t be any turning back as it really is a matter of life and death. I am no longer in denial.
So how am I doing?
The weight has been coming off, slowly but surely. I haven’t made any major progress in the last month, but then again I didn’t gain anything of significance over the holidays. That’s a good thing. Okay, it’s a very good thing. Looking at it with the ‘glass’ being half empty I am still only 1/2 way to where I need to be to have my waist circumference 1/2 my height. Looking at it with the ‘glass’ being half-full, I’ve lost 30 pounds. I feel better about how I look than I have in many years, and I am only half way there. I am celebrating my progress, but not letting it be enough because health-wise, it isn’t. To truly reduce my risk of heart attack and stroke, I need to lose another 30 pounds, or whatever weight will actually put my waist circumference at half my height.
I’ve loss 6 inches off my waist. That’s 1/2 a foot! Crazy, eh? I only have another 4 inches to lose off my waist for me be in the low-risk category and I am guessing that will correlate to another 30 pounds of weight loss. Maybe it will be less, maybe more, but my weight loss goal is whatever it takes for my waist to be half my height. The scale won’t determine my goal, the tape measure will.
My blood pressure has been ranging from between just below the normal range to pre-hypertension for months, but to protect my kidneys I am continuing to take a “baby dose” of Ramipril® (2.5 mg per day) that I asked the doctor to put me on until my blood pressure is consistently below normal and the meds need to be reduced or discontinued. The dose I’m on is the smallest it comes in and my doctor has switched me to tablets, which can be split if my blood pressure is consistently on the low side.
As covered in an earlier update, my triglycerides and cholesterol are now in the ideal range simply from the dietary changes I have made.
My blood sugar has been a bit frustrating, because overall it isn’t going down nearly as fast as I thought it would, or as I’ve observed other people’s to do. Everybody’s different and mine is just taking this long despite all the things I am doing right. I started out eating “low carb” (50 gm carbohydrate per day) and as it turned out it wasn’t low carb enough, perhaps because of how long I’d been Diabetic and just how insulin resistant I really am. A few months ago, I added regular intermittent fasting (IF) – fasting 23 hours from the end of supper to the beginning of supper the following day (drinking ‘bone broth’ and tea and other appropriate beverages while fasting). I have done one slightly longer fast, with careful monitoring. Along with IF, a number of months ago I also lowered my carb intake to ≤ 35 gm of carbs per day and monitor my blood sugar 5-7 times per day to make sure it doesn’t dip too low. During the day time, towards the end of a 24 hour fast, my blood sugar will be in the low 4’s mmol/L (~81 mg/dl) just before I eat again, but in the morning, the lowest it has ever been is 5.8 mmol/L (105 mg/dl). No matter what I do the night before (i.e. exercise, eat very low carb) my blood sugar begins rising around 3 am and continues rising until 6 or 8 am, even though I am fasting. It is classic “dawn phenomenon” and it has been incredibly frustrating.
My HbA1C has dropped from ~9.0 % (at the beginning of March) to 7.5 % (July 25 2017) to 7.0 % (October 11 2017) in 7 months, but for the last 3 months it has remained stubbornly at 6.8 % – almost exclusively because my fasting blood sugarremains high. This led me to a decision to ask my doctor to trial me on a “baby dose” of Metformin® only at night to see if it will help bring down my fasting blood sugar and more importantly, the corresponding insulin resistance, while I continue to eat a very low carb (ketogenic) diet and practice intermittent fasting.
After reviewing the over 400 glucose readings I took from March 5, 2017 onward and seeing that my HbA1C remains only slightly lower the last 3 months despite all my lifestyle changes, my doctor agreed to trial me on the lowest dosage of Metformin® over the next 3 months (the dose given to youth with high blood sugar). It will be interesting to see its effect as of January 6, 2018. What many people may not realize is that while Metformin® is now a pharmaceutical (medication), it was initially derived from a plant called “goat’s rue” or the French lilac and has been used since the Middle Ages to treat the symptoms of Diabetes. It’s not unlike acetylsalicylic acid (ASA), which is the active compound in Aspirin® which was originally isolated from white willow bark. Aspirin® and Metformin® are both natural in origin.
In addition to its natural origins and long-standing safety record, studies indicate that people with Diabetes who take Metformin® have lower incidence of cancer and dementia and in animal models, increased longevity has also been reported. Given all of these factors, it seemed reasonable for me to ask my doctor to trial me on a small dose of Metformin® to see if it keeps my liver from manufacturing too much glucose in the early hours of the morning, thus lowering my overall insulin resistance, while I continue to eat ketogenically and practice intermittent fasting. My doctor agreed. While it is too soon to know how much impact this small dose will have, from January 6th until today, my blood sugar is averaging 6.5 mmol/L, yet still rising from 3 am until 6 am. I will give it a few more weeks and then possibly ask my doctor to try me on the same dosage of slow-release Metformin®, to see if my morning blood sugar is improved.
It may seem strange to some that I would add medication after successfully having lost so much weight, having brought my lipids into the ideal range for non-Diabetics, and having lowered my blood sugar to the ideal range for Diabetics (≤ 7.0%) solely by adopting a low carb lifestyle and practicing intermittent fasting. I view much it like wearing a brace or using a cane after injuring one’s knee. It’s not a permanent measure, but support and protection while the healing continues to take place.
This is my journey, and my progress and challenges are as individual as I am. Everyone is different and the degree of carb reduction and whether or not intermittent fasting may be helpful for you is something that will only be known it time as we work together. One thing is for certain is that unless one starts the process of working towards achieving their health and wellness goals, things will not improve on their own.
Have questions?
Please send me a note using the “Contact Me” form located on the tab above.
The photo on the left is what I looked like when I started my weight-loss and health ‘journey’ on March 16, 2017, 9 months ago. The photo on the right, is me today.
Based on my BMI, I was well into the Class I Obesity category 9 months ago. Based on my BMI today, I am just 15 pounds from my weight falling in the normal range.
At the beginning of March, my blood pressure ranged between Stage 2 Hypertension and Stage 1 Hypertension — sometimes being dangerously high. Now, my blood pressure hovers around 125/80 mmHg mark, and I am still on the ‘baby-dose’ of Ramipril for now, as it protects my kidneys.
My triglycerides and my LDL cholesterol (”bad cholesterol”) were high, certainly well above what it should have been for someone who has Type 2 Diabetes and had family risk factors. Thankfully, my HDL was good, offering some protection.
In the past 9 months, my morning fasting blood sugar has dropped from ±12 mmol/L (216 mg/dl) to anywhere from 5.8 mmol/L (105 mg/dl) to 6.5 mmol/L (117 mg/dl) – with the occasional 8.0 mmol/L (144 mg/dl) for seemingly no apparent dietary reason. For my fasting blood sugar to be in the non-diabetic range, it needs to be consistently below 5.5 mmol/L (99 mg/dl).
When I began this journey, my HbA1C was ~ 9.5% and during the last 30 days, I am averaging ~6.3% which is in the non-diabetic range. This has been entirely achieved without any medication to lower blood glucose.
I was determined to reverse the symptoms of Diabetes, high cholesterol and high blood pressure by changing how I ate and by introducing short periods of intermittent fasting and I have certainly made significant progress.
Weight and Body Measurements
I’ve lost ~25 lbs so far, but the changes in my body and face shape are even more noticeable, as evidenced by the photo above.
So far, I’ve lost;
1″³ off my upper arms
3″³ off my neck (!)
1″³ off my thighs
4 1/2″³ off my waist
This week, I reached the “goal weight” that I initially set for myself, but in order to attain an ideal waist circumference that is 1/2 my height, I probably have to lose another 20-25 pounds, which means I am half-way there.
I am entirely convinced that this is realistic and attainable.
Change only happens when the pain of staying the same is greater than the pain of changing.
Want to start your own weight loss and health journey? Why not send me a note using the “Contact Us” form above.
Wishing you and yours all the best for holiday season!
Note: I am a “sample-set of 1” – meaning my results may or may not be like anybody else’s that follows a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
INTRO: “Before” and “after” photos are often the source of encouragement, as I progress on my journey. This “before and since” photo serves as some Monday-morning motivation.
Yesterday, after ten days on crutches and a brace due to a torn MCL tendon, I had finally progressed to a cane and just had to get out for a bit. With a break in the rain, one of my sons and I headed for Indian Arm, an ocean inset nearby. It was mild and humid and I really didn’t want to wear a long sleeve jacket, so I reached for a down-filled vest that I bought a number of years ago that never zipped or snapped up, and headed out. When we arrived, there was a breeze off the salt water and instinctively, I zipped up the vest and snapped the outer snaps. Only in hindsight did I realize this was the first time I ever did that – and with a little room to spare.
We walked (actually, I hobbled on my cane) along the coast path and down to the pier and took in the fresh air and beautiful view. As we were leaving, I remembered the photo that was taken of me 2 1/2 years ago on the same pier, around the time I first learned about eating low carb high fat (LCHF) and asked my son to snap a photo of me on my phone, so I could compare them. In both photos, I was dressed in comfortable clothes, with no makeup and my hair however it was.
When we returned home, I dug out the old photo and here they are, side by side. Even with my puffy down-filled vest and knee brace, the difference is noticeable, even though it has only been 6 months that I have been “practicing what I preach” and eating low carb, myself. Since I am very much ‘in progress’ with my weight loss and achieving my health goals, I refer to this as before and since rather than before and after.
Me – summer 2015 (left), me fall 2017 (right)
It will be interesting to take an updated photo this time next year to see the progress.
Encouragement in our health journeys come in many forms; a number on the scale, new lab results, readings on a glucometer, or photos over time.
Today I celebrate this mid-point progress in this Dietitian’s Journey and I encourage you to celebrate yours!
Note: I am a “sample-set of 1” – meaning that my results may or may not be like any others who follow a similar lifestyle. If you are considering eating “low carb” and are taking medication to control your blood sugar or blood pressure, please discuss it with your doctor, first.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.




 Here is my “before” and “after” pictures now, at 21 months. I’ve lost the additional 4 inches off my waist – a foot in total! I lost a FOOT off my waist!!
Here is my “before” and “after” pictures now, at 21 months. I’ve lost the additional 4 inches off my waist – a foot in total! I lost a FOOT off my waist!!
 carb New York Style Cheesecake (also under Recipes).
carb New York Style Cheesecake (also under Recipes). I invent recipes for myself that my ethnic clients find really helpful, including things such as Low Carb Roti (Indian flatbread) and Low Carb Chow Mein Noodles because I believe that a low carb lifestyle is not a “one-sized-fits-all”.
I invent recipes for myself that my ethnic clients find really helpful, including things such as Low Carb Roti (Indian flatbread) and Low Carb Chow Mein Noodles because I believe that a low carb lifestyle is not a “one-sized-fits-all”.








 I’ve learned my ‘lesson’ the hard way but it need not have been so.
I’ve learned my ‘lesson’ the hard way but it need not have been so.







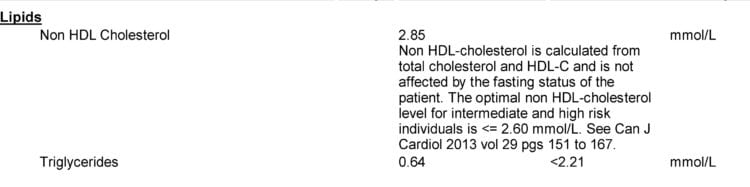


 The photo on the left was me before I began what I’ve called “my journey”, a Dietitian’s Journey.
The photo on the left was me before I began what I’ve called “my journey”, a Dietitian’s Journey.

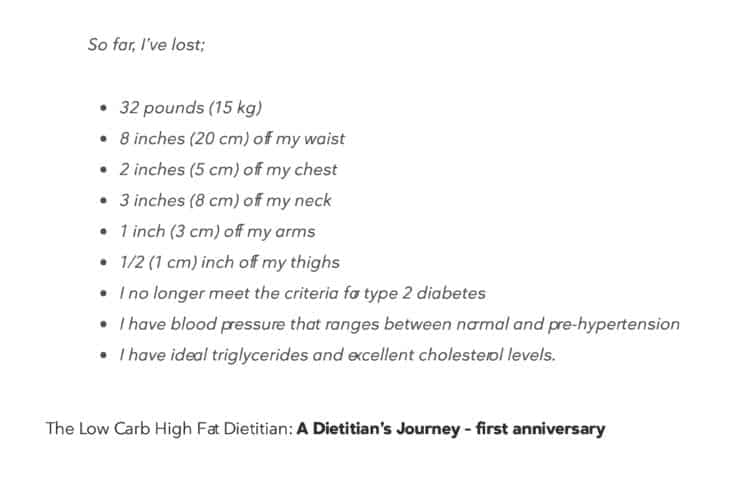
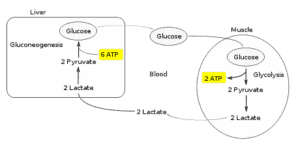 When I am doing High Intensity Training (lifting weights very slowly until muscle failure) my body first uses up all the glycogen stored in those muscles.
When I am doing High Intensity Training (lifting weights very slowly until muscle failure) my body first uses up all the glycogen stored in those muscles.





 To celebrate my one year anniversary, as a ‘present’ to myself, I bought a weight bench to use with my free weights and resistance bands, and have set it up in a corner of my room.
To celebrate my one year anniversary, as a ‘present’ to myself, I bought a weight bench to use with my free weights and resistance bands, and have set it up in a corner of my room. Are you at a fork in the road – having to choose between continuing to do the same things that haven’t worked previously or like me, ignoring it all and doing nothing?
Are you at a fork in the road – having to choose between continuing to do the same things that haven’t worked previously or like me, ignoring it all and doing nothing?









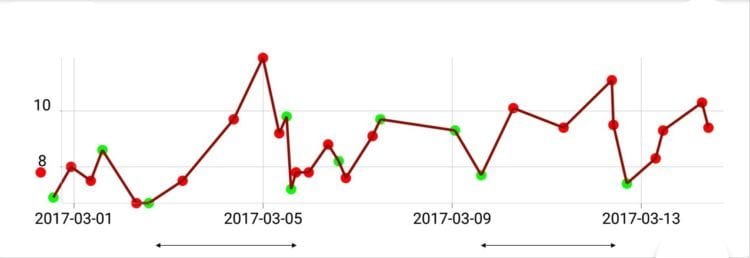
 As can be seen from the graph, my blood glucose was at lowest at 7.7 mmol/L (see photo to the left) and I had spikes well above 10 mmol/L, and I was averaging around 8.5 mmol/L over the course of the day – which is slightly higher than the average of those in the study.
As can be seen from the graph, my blood glucose was at lowest at 7.7 mmol/L (see photo to the left) and I had spikes well above 10 mmol/L, and I was averaging around 8.5 mmol/L over the course of the day – which is slightly higher than the average of those in the study.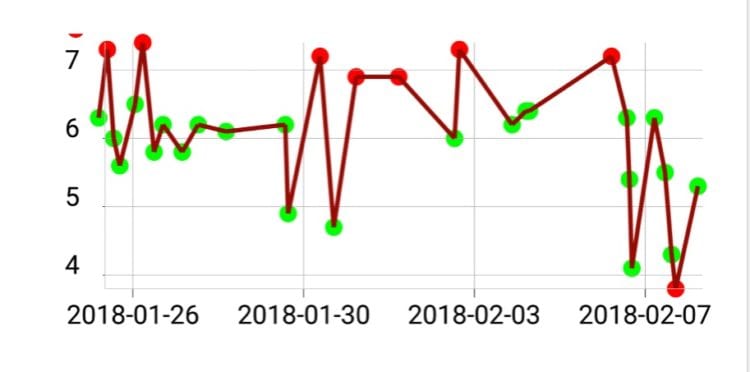
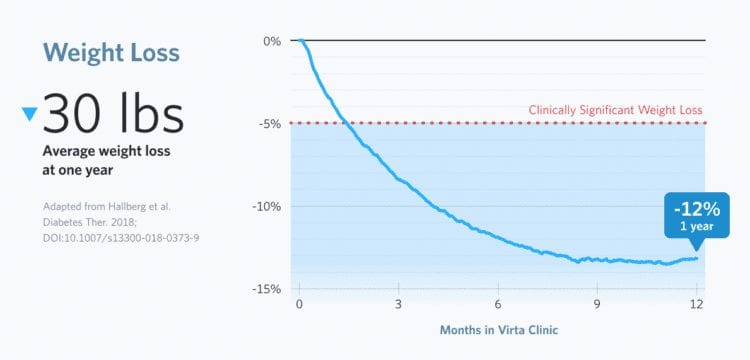
 Early this morning, my fasting blood glucose was 5.3 mmol/L (95 mg/dl) which is in the normal non-Diabetic range. This is a first! This was without taking Metformin.
Early this morning, my fasting blood glucose was 5.3 mmol/L (95 mg/dl) which is in the normal non-Diabetic range. This is a first! This was without taking Metformin.








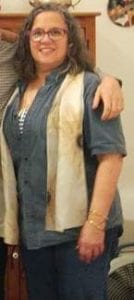 My journey began on March 5, 2017 when I was a fat Dietitian with all the benchmark symptoms of Metabolic Syndrome including Type 2 Diabetes, high blood pressure, high LDL cholesterol and triglycerides, abdominal adiposity (i.e. “a belly”) and high BMI (high weight for height). Physically I was a mess but my biggest problem was that I was in denial. It had been months since I had monitored my own blood sugar or blood pressure even though I had been diagnosed with Type 2 Diabetes 10 years earlier. I knew better.
My journey began on March 5, 2017 when I was a fat Dietitian with all the benchmark symptoms of Metabolic Syndrome including Type 2 Diabetes, high blood pressure, high LDL cholesterol and triglycerides, abdominal adiposity (i.e. “a belly”) and high BMI (high weight for height). Physically I was a mess but my biggest problem was that I was in denial. It had been months since I had monitored my own blood sugar or blood pressure even though I had been diagnosed with Type 2 Diabetes 10 years earlier. I knew better.