The most recent data available from 2011 indicates that the cost per person per year of having Type 2 Diabetes in Canada ranges from $1611 (Quebec) to $3427 (New Brunswick) based on an average income of $43,000 per year. Necessary medications, devices and supplies are expensive – costing more than 3% of income. While those with extended health benefits may not consider this cost now, a change in employment circumstances can affect this overnight.
As Type 2 Diabetes progresses, more medications are often added and the number of times blood sugar needs to be taken each day often increases, as well. Job loss or retirement suddenly results in Canadians being faced with bearing the burden of their disease, along with the chronic, progressive nature of poorly managed blood sugars.
A per-province breakdown using the 2011 figures from the Canadian Diabetes Association appears below;
Cost of Type 2 Diabetes per person per year by province (2011 figures) – from Canadian Diabetes Association
It doesn’t have to be so.
Long term studies that have been published in the last couple of years (reviewed in previous articles on this site) which demonstrate that a well-designed low carbohydrate or ketogenic diet can and does enable a significant improvement in Type 2 Diabetes symptoms.
After as little as 10 weeks, glycosylated Hemoglobin (HbA1C) has been reported to drop a full percentage point; from 7.6% to 6.6%. After a year, the average HbA1C was 6.3%, which is below the diagnostic criteria for Type 2 Diabetes. That is, in just a year of following a well-designed low carbohydrate diet, it has been demonstrated that people can get their average blood glucose in the non-Diabetic range.
Medication use drops substantially when people are able to control their blood sugar by limiting the amount and types of carbohydrates they eat. At the start of the study mentioned above published in Feb of 2018, 87% of people were taking at least one medication for Diabetes and at just 10 weeks, almost 57% had one or more Diabetes medications reduced or eliminated. After one year, Type 2 Diabetes medication prescriptions other than Metformin declined from 57% to below 30%. Insulin injections were reduced or eliminated in 94% of users and sulfonylurea medication was entirely eliminated.
For each one of these individuals, a simple change to a low carbohydrate diet resulted not only in significantly improved health and a reduction in Diabetes symptoms, but in significantly reduced cost, as well.
According to Virta Health who conducted the study referred to above, cost savings are as indicated in this diagram below.
The cost of “Diabetes Reversal” below reflects the estimated cost of an individual being cared for by the Virta Health multi-disciplinary team program, which appears to be an excellent program given the methods used in the studies they have published. It should be noted that the cost of working one-on-one with me over the course of a year (and as overseen by your GP) is substantially less. In fact, getting started by being assessed and having me design an individual Meal Plan just for you is significantly less than the yearly cost of achieving better blood sugar control in the graphic below.
Sometimes people are hesitant to invest in the cost of seeing a Registered Dietitian who can help them adopt a low carbohydrate lifestyle that can enable them to achieve significantly improved blood sugar control – even though the yearly costs of Diabetes supplies is far greater than the cost of being assessed and getting a Individualized Meal Plan. Such an estimate is at the level of health they are today, but waiting a few years, with longer Type 2 Diabetes, more medications, possibly including insulin injections, and the cost is closer to $3500 in 2011 Canadian dollars / $4000 in 2018 (US) dollars.
Does this make any sense?
The sooner someone changes their diet and lifestyle upon being diagnosed with Type 2 Diabetes, the more likely it seems they may be able to achieve full remission of symptoms. If you’ve followed my own story on “A Dietitian’s Journey” then you know how much harder it is for me, after being diagnosed 10 years ago.
If you have extended benefit coverage, then now is the time to invest some time in learning how to make lifestyle changes that will benefit your health and your finances for the years to come. Even for those without such coverage, the cost of an assessment package which will provide you with a Meal Plan designed specifically for you is substantially less than you are already paying for your medications, devices and supplies. I provide both in-person services in my Coquitlam, British Columbia office and via Skype Distance Consultations.
If you have questions about this package entails or about the flexible payment options that are available, why not send me a note using the “Contact Me” form located above? I’ll be happy to reply.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
One of the concerns raised by opponents of a very low carb or ketogenic diet is that it increases risk of cardiovascular disease such as heart attack and stroke, but does it?
Results of a peer-reviewed study of cardiovascular outcomes of people with Type 2 Diabetes (T2D) that was published at the beginning of May in the Journal of Cardiovascular Diabetology[1] found that those that followed a ketogenic diet significantly improved in 22 of 26 cardiovascular disease risk factors, including biomarkers of cholesterol / lipoproteins, blood pressure, inflammation, and carotid intima media thickness (cIMT).
Previous published results from the same researchers and published in February of 2018 demonstrated that reversal of T2D symptoms was able to be achieved and sustained long term using a ketogenic diet[2,3].
Simply by decreasing the amount of carbohydrate in the diet over the course of a year there was not only a significant decrease in blood sugar and weight, but a dramatic improvement in lipid and lipoprotein markers associated with markers of cardiovascular risk.
The results of this most recent study do much to dispel the myth that a therapeutic ketogenic diet puts individuals at increased risk for heart attack and stroke. In fact, it reduces their risk.
Methods
Continuous Care Intervention (CCI) Group Participants
At the beginning of the study, there were 238 participants enrolled in the continuous care intervention (CCI) group and all had a diagnosis of Type 2 Diabetes (T2D) with an average HbA1c of 7.6% ±1.5%. They ranged in age from 46 — 62 years of age, 67% were women and 33% were men. Weight of the subjects ranged from 200 pounds to 314 pounds (117±26 kg) with an average weight of 257 pounds (117 kg) and Average Body Mass Index (BMI) was 41 kg·m-2 (class III obesity) ±9 kg·m-2, with 82% categorized as obese. The majority of participants (87%) were taking at least 1 medication for glycemic control medication.
At the end of a year, 218 participants (83%) remained enrolled in the continuous care intervention (CCI) group.
Intervention and Monitoring of CCI Group
Each participant in the CCI group received an Individualized Meal Plan which enabled them to attain and maintain nutritional ketosis. They also received behavioral and social support, biomarker tracking tools, and ongoing care from a health coach with medication management by a physician.
Subjects typically required <30 g·day−1 total dietary carbohydrates.
Daily protein intake was targeted to a level of 1.5 g·kg−1 based on ideal body weight and participants were coached to incorporate dietary fats until they were no longer hungry.
Other aspects of the diet were individually tailored to ensure safety, effectiveness and satisfaction, including consumption of 3-5 servings of non-starchy vegetables and sufficient mineral and fluid intake.
Participants ability to achieve and maintain nutritional ketosis was determined by subjects monitoring their blood ketone level of β-hydroxybutyrate (BHB) using a portable, handheld device. Blood glucose and β-hydroxybutyrate (BHB) levels were initially tracked daily using a combination blood glucose and ketone meter and frequency of tracking was modified by the care team based based on each individual’s needs and preferences.
Participants with high blood pressure (hypertension) were provided with an automatic home blood pressure machine (sphygmomanometer) and they were instructed to record their readings daily to weekly in the supplied app, depending on recent blood pressure control. Antihypertensive medication prescriptions were adjusted based on home blood pressure readings and reported symptoms.
Downward Adjustment and/or Discontinuation of Medications
As blood pressure came down, diuretic medication was the first antihypertensive medication to be discontinued. This was followed by beta blockers (unless the participant had a history of coronary artery disease).
Angiotensin-converting-enzyme inhibitors (ACE inhibitors) and angiotensin II receptor blockers (ARBs) were generally continued due to their known protective effect on the kidneys in those with Type 2 Diabetes.
Statin medications were adjusted to maintain a goal of LDL-P under 1000 nmol L−1 (or based on participant preference after full risk/benefit discussion with the physician).
The Usual Care (UC) Group
For comparison purposes, an independent group of patients with Type 2 Diabetes were also recruited for the study and were referred to Registered Dietitians that provided dietary advice according to the American Diabetes Association Guidelines [4].
Laboratory Assessors
Since an abnormal lipid / cholesterol profile (“atherogenic dyslipidemia”) is a known risk factor for CVD [5] and is very common in people with Type 2 Diabetes, a number of laboratory tests were conducted at the beginning of the study and the end to determine if they improved, stayed the same or got worse.
Most common in people with Type 2 Diabetes is where there are increased triglycerides (TG), decreased high-density lipoprotein cholesterol concentration (HDL-C) and increased small low-density lipoprotein particle number (small LDL-P).
The authors of this study state that evidence suggests that increased very low-density lipoprotein particle number (VLDL-P) and a large VLDL-P in particular may be one of the key underlying abnormalities in this abnormal lipid / cholesterol profile (“atherogenic dyslipidemia”) associated with T2D.
The authors also outline how higher concentrations of small LDL are often associated with increased total LDL particle number (LDL-P) and increased ApoB which is the main protein constituent of very low-density lipoprotein (VLDL) and low-density lipoprotein (LDL). The authors provide previous study evidence that demonstrates that in people with insulin resistance and T2D, increased total LDL particle number (LDL-P) and increased ApoB may exist even with normal to low LDL-C concentrations values. For this reason, LDL-C alone was not relied on as a measure of abnormal lipid / cholesterol profile (“atherogenic dyslipidemia”) in this study as it could miss the impact of increased total LDL particle number (LDL-P) and/or ApoB.
The authors mentioned that in previous studies with carbohydrate restriction of up to 1 year, while triglycerides (TG) usually decrease and HDL-C often increase, LDL-C sometimes increased and other times decreases. The authors note that although higher LDL-C is a known risk factor for CVD, low LDL-C may also reflect higher small, dense LDL, total LDL particle number (LDL-P) or ApoB and thus be a risk factor, as well.
Since inflammation is involved at all stages of the atherosclerotic process, higher high-sensitivity C-reactive protein (CRP) and/or higher white blood cell count (WBC) were assessed as risk factors for CVD.
Finally, since high blood pressure (hypertension) is also an added risk factor for CVD in people with T2D, tighter blood pressure control was deemed to reduce the risk of DVD, stroke and other microvascular events.
Continuous Care Intervention (CCI) Group
Standard laboratory fasting blood draws of the CCI group were obtained at the start of the study (baseline), at 70 days (3 months) and at ~ 1 year follow-up.
Lipid/cholesterol-related tests included ApoB, ApoA1, total cholesterol, triglycerides, direct HDL-C concentrations and LDL was calculated using the Friedewald equation.
The LipoProfile3 algorithm was used to determine relationship of lipid subfractions to cardiovascular (CVD) risk – specifically the number of HDL particles (HDL-P) previously reported to be associated with death, Myocardial Infarction (MI), stroke and hospitalization, HDL-C (HDL cholesterol) which is the amount of cholesterol those particles are carying, which is not associated with these negative outcomes and HDL-P subclasses [6].
Risk was also determined using the lipoprotein insulin resistance score (LP-IR) which was proposed to be associated with the homeostasis model assessment of insulin resistance (HOMA-IR) and glucose disposal rate (GDR) [7].
Finally, risk was also determined using the 10-year atherosclerotic cardiovascular disease (ACSVD) risk score of the American College of Cardiology [8].
Carotid ultrasonography (cIMT) measure was performed at baseline and 1 year to characterize atherosclerotic risk.
The Usual Care (UC) Group
Body measurements, vital signs and fasting blood draws for the Usual Care (UC) group were obtained at the start of the study (baseline) and at 1 year using the same clinical facilities and laboratory and data collection methods. Carotid ultrasonography (cIMT) measure was also performed at baseline and 1 year to characterize atherosclerotic risk.
Results
There were no significant difference in the baseline characteristics of the two sub groups of CCI participants (web-based on onsite-based) and no significant difference at 1 year, so for the purpose of analysis, data from both groups were combined.
As well, there were no significant difference in the baseline characteristics of the Usual Care (UC) group (which served as an observational comparison group) and the Continuous Care Intervention Group (CCI) except mean body weight and BMI were higher in the CCI versus the UC group.
The within-Continuous Care Intervention group changes in the following lipids and lipoproteins were all statistically significant and were as follows; ApoA1 [a component of high-density lipoprotein (HDL)] increase by +”‰9.8%) ApoB / ApoA1 ratio decreased by −”‰9.5% Triglycerides (TG) decreased by −”‰24.4% LDL-C increased by +”‰9.9% but LDL-particle size also increased by +”‰1.1% (that is, large fluffy LDL increased compared with small, dense LDL) HDL-C increased by +”‰18.1% total HDL-P increased by +”‰4.9% large HDL-P increased by 23.5% Triglyceride/ HDL-C ratio decreased by −”‰29.1% large VLDL-P decreased by −”‰38.9% small LDL-P decreased by −”‰20.8% There were no significant changes in total LDL-P or ApoB.
These results are impressive!
Simply by decreasing the amount of carbohydrate in the diet over the course of a year there was a dramatic improvement in lipid and lipoprotein markers associated with markers of cardiovascular risk.
In addition, the Continuous Care Intervention group had a significant reduction in;
systolic blood pressure decreased −"‰4.8%
diastolic blood pressure decreased −"‰4.3%
C-Reactive Protein (CRP) decreased almost 40% (i.e. −"‰39.3%)
white blood cell (WBC) count decreased −"‰9.1%
Below are graphs of the changes in biomarkers for the Continuous Care Intervention (CCI) group (figure 1) and the Usual Care (UC) Group;
FIGURE 1: changes in biomarkers for the Continuous Care Intervention (CCI) group
FIGURE 2: changes in biomarkers for the Usual Care (UC) group
Below is a comparative graph of the two groups, the Continuous Care Intervention (CCI) Group and the Usual Care (UG) Group
FIGURE 3: changes in biomarkers for the Continuous Care Intervention (CCI) group compared to the Usual Care (UC) group
Some Final Thoughts…
This study demonstrates that a therapeutic ketogenic diet followed over the course of 1 year significantly improved 22 of 26 cardiovascular disease risk markers in those with Type 2 Diabetes. This is huge!
The size of the study group was large and had an 83% retention rate over the course of the year – which in and by itself demonstrates that the intervention diet was one that people had no difficulty staying with in their day-to-day lives, without the use of meal replacements (shakes or bars).
While not a randomized control trial between CCI and UG groups, this study supports that a ketogenic diet is both safe and effective for periods of up to a year (and in other studies has been documented to be safe and effective for up to two-years). Not only can a well-designed ketogenic diet reverse many of the symptoms of Diabetes (documented in this earlier article) it can also significantly improve risk markers for cardiovascular disease.
Do you have questions about how a carefully-designed low carbohydrate or ketogenic diet can help you improve symptoms of Type 2 Diabetes and lower markers of risk factors for cardiovascular disease?
Please send me a note using the ”Contact Me” form above to find out more about how I can provide you with in-person or Distance Consultation services (via Skype or long distance telephone).
Bhanpuri NH, Hallberg SJ, Williams PT et al, Cardiovascular disease risk factor responses to a type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: an open label, non-randomized, controlled study, Cardiovascular Diabetology, 2018, 17(56)
McKenzie AL, Hallberg SJ, Creighton BC, Volk BM, Link TM, Abner MK, Glon RM, McCarter JP, Volek JS, Phinney SD, A Novel Intervention Including Individualized Nutritional Recommendations Reduces Hemoglobin A1c Level, Medication Use, and Weight in Type 2 Diabetes, JMIR Diabetes 2017;2(1):e5, URL: http://diabetes.jmir.org/2017/1/e5, DOI: 10.2196/diabetes.6981
Hallberg SJ, McKenzie AL, Williams, PT et al. Diabetes Ther (2018). Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study.
America Diabetes Association, Lifestyle management. Diabetes Care. 2017;40 (Suppl 1):S33—S43
Fruchart J-C, Sacks F, Hermans MP, Assmann G, Brown WV, Ceska R, et al. The Residual Risk Reduction Initiative: a call to action to reduce residual vascular risk in patients with dyslipidemia. Am J Cardiol. 2008;102:1K—34K.
May HT, Anderson JL, Winegar DA, Utility of high density lipoprotein particle concentration in predicting future major adverse cardiovascular events among patients undergoing angiography, Clinical Biochemistry, 2016;49(15): 1122-1126
Shalaurova I, Connelly MA, Garvey WT, Otvos JD. Lipoprotein insulin resistance index: a lipoprotein particle-derived measure of insulin resistance. Metabol Syndr Relat Disord. 2014;12:422—9.
Goff DC, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, et al. ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;2014:S49—73 (tool: http://tools.acc.org/ASCVD-Risk-Estimator-Plus/#!/calculate/estimate/)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
In a recent article about why Waist Circumference and Waist-to-Height Ratio is so important, I explained that a meta-analysis from 2012 which pooled data from 300,000 adults of different races and ages found that the lowest risk of cardiovascular disease and shorter lifespan was associated with a Waist to Height Ratio (WHtR) of 0.5. That is, we are at lowest risk when our waist circumference is less than half our height (even if our BMI is in the normal range). I also explained exactly how to take waist circumference, so that the results are accurate.
There are other measures of cardiovascular risk that I think are worth considering.
A 2015 study of 3200 adults found that Waist-to-Hip Ratio (WHR) is more accurate in predicting 10-year cardiovascular risk than Waist to Height Ratio (WHtR), however whether this relationship would hold up in a sample as large as the meta-analysis above is unknown. I feel it is worth mentioning Waist-to-Hip Ratio (WHR) as an indicator of cardiovascular risk, as it is easy to do.
Another index this 2015 study found to accurately predict 10-year cardiovascular risk was something called Conicity Index which I will touch on even though it is not as easily determined as Waist-to-Hip Ratio (WHR) or Waist to Height Ratio (WHtR).
Determining Waist to Hip Ratio
As mentioned in the previous article, to use these indices requires waist measurements and hip measurements to be done accurately and at a specific place on the body. To make it easier, I will repeat how to measure waist circumference here and below, how to measure hip circumference.
Measuring Waist Circumference
For the purposes of calculating risk associated with increase abdominal girth, waist circumference needs to be measured at the location that is at the midpoint (i.e. half way) between the lowest rib and the top of the hip bone (called the ”iliac crest”). Below is a picture that should help.
Where to measure waist circumference
This measurement should be taken with a flexible seamstress-type tape measure, being sure that the tape measure is at the same height in the front and the back, when looking in front of a mirror. That is, the tape measure should be perpendicular to the floor (not higher in the back or the front).
It’s also important that the person’s abdomen (belly) is completely relaxed when taking the measurement, not sucked in. One way to do that is to taking a deep breath and let it out fully just as the measurement is taken.
If your Waist to Height ratio is greater than 0.5, then you are at increased risk for cardiovascular events and a shortened lifespan. Looking at the graph above, one can see that for every little bit over 0.5, the risk rises steeply.
Measuring Hip Circumference
Hip circumference needs to be measured at the widest portion of the buttocks (butt) and as with waist circumference, the tape measure needs to be parallel to the flood (same height in the front and the back, when looking in front of a mirror).
For both the waist and hip measurement, the tape measure should be snug around the body, but not pulled so tight that it is constricting and it is best if a stretch”resistant but flexible seamstress-type tape measure is used.
Assessing Waist-to-Hip Ratio
If the waist circumference is measured in inches, then the hip circumference needs to be as well – same if the measurement is in centimeters; both need to be in the same units.
To calculate the Waist-to-Hip Ratio take the waist circumference and divide it by the hip circumference.
Waist-to-Hip Ratio and Risk of Cardiovascular Disease
The following ratios are associated with low, moderate and high risk of cardiovascular risk;
Low Risk: For men, if the ratio is 0.95 or less, for women if the ratio is 0.80 or less
Moderate Risk: For men, if the ratio is 0.96 – 1.0, for women if the ratio is 0.81 – 0.85
High Risk: For men, if the ratio is 1.0 or more, for women if the ratio is 0.85 or more.
The Waist-to-Hip Ratio can also be thought of as people being shaped like “apples” or “pears”.
People who carry most of their excess weight around their middle (“apples”) have more visceral fat and this type of fat is much more dangerous than the fat under our skin (called “sub-cutaneous fat”) because it is found around the heart, liver, pancreas and other organs and increases the risk not only of cardiovascular disease, but also Type 2 Diabetes and hypertension.
People who’s hips are much wider than their waist (so-called “pears”) have less visceral fat and therefore lower risk of these weight-related health problems.
Conicity Index
Conicity Index(CI) is a little more cumbersome a calculation than either Waist-to-Hip (WHR) Ratio or Waist-to-Height (WHtR), but was found in the 2015 study mentioned above with 3200 subjects to be a strong predictor of cardiovascular risk.
Conicity literally means “cone-shaped” and determines how much our body fat distribution like two end-to-end cones.
In the first figure below, body weight is distributed evenly, however when someone has a conical distribution, their weight is more heavily distributed around the abdomen. As a result, it has increased conicity and is more highly correlated to increased cardiovascular disease (as well as Type 2 Diabetes and hypertension).
For those who are interested in calculating Conicity Index (CI), the formula is below along with the formula for Waist-to-Hip (WHR) Ratio, Waist-to-Height (WHtR).
Indices of central adiposity [1]
Final Thoughts…
Given the sample size of the data on which Waist-to-Height (WHtR) is based (300,000 adults) and that it is an easy to determine and robust measure of cardiovascular risk, this is the one I tend to favour. That said, Waist-to-Hip (WHR) Ratio was previously used for years and found to be a simple and accurate predictor of risk. From that point of view, either could be used, but why not both?
In my clinical experience, I have encountered many people with much wider hips than waist (so-called “pears”) but whose Waist-to-Height (WHtR) is considerably greater than 0.5, and for this reason I tend to put more credence on Waist-to-Height (WHtR) than Waist-to-Hip (WHR) Ratio as a measure of visceral fat and increased cardiovascular risk.
Since both Waist-to-Height (WHtR) and Waist-to-Hip (WHR) Ratio are very easy to determine, for those with a family risk of cardiovascular disease, Type 2 Diabetes or hypertension, I think it makes sense to aim for a waist measurement that is within both of these easily obtained measures.
Do you have questions about how I can help you lower your risk of cardiovascular disease, Type 2 Diabetes or hypertension? I provide both in-person and Distance Consultation services via Skype or telephone (and remember, many extended benefits plans will reimburse for visits with a Registered Dietitian).
Please feel free to send me a note using the “Contact Me” form on the tab above to find out more.
Rabiee B, Motamed N, & Perumal D, et al. Conicity index and waist-hip ratio are superior obesity indices in predicting 10-year cardiovascular risk among men and women. Clin. Cardiol. 38, 9, 527—534 (2015)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Most of us know that obesity is where a person has high levels of body fat, but at what point does overweight become obese? There are different ways of determining this and one way that many people are familiar with is the Body Mass Index.
Body Mass Index (BMI) classifies whether a person is overweight or obese by looking at their weight to height ratio. It is calculated by taking a person’s weight (in kilograms) and dividing it by their height (in meters squared).
BMI= weight (kg) / height (m) x height (m).
People are considered overweight if their BMI is between 25 and 29.9 and obese if it is above 30.
There are different levels of obesity, too. For Caucasians*:
Class I obesity is a BMI between 30 and 34.9.
Class II obesity is a BMI between 35 and 39.9.
Class III obesity (also called morbid obesity) is a BMI is greater than 40.
*There is a different scale for those of Asian and South Asian ancestry, which is approximately 5% lower.
Research has found that waist-to-height ratio is a much better predictor than Body Mass Index (BMI) of cardiovascular health risk such as heart attack and stroke, as well as a shorter lifespan due to other illnesses.
A meta-analysis from 2012 pooled data from multiple studies, and examined Waist to Height Ratio (WHTR) in more than 300, 000 adults from several different ethnic groups and found that was a far better predictor of cardiovasular of metabolic risk factors in both men and women, than BMI [1].
A 2014 study found a correlation between Year of Life Lost (YLL) for different values of Waist to Height Ratio (WHtR) and found that YLL increased dramatically in both males and females when above 0.52 – a waist circumference of just over half one’s height [2].
Waist-to-Height Ratio Is More Predictive of Years of Life Lost than Body Mass Index [2]These two studies found that the least amount of years of life lost is associated with a Waist to Height Ratio of 0.5. That is, our waist circumference should be less than half our height, even if our BMI is in the “normal range”*.
*Both males and female non-smokers have a slightly increased Years of Life Lost at waist circumference > 0.50, even when their BMI was in the normal range (18.5 to to 22) – which means that waist circumference is a more important predictor of shortened lifespan due to cardiovascular disease, than BMI.
Determining Waist to Height Ratio
If you’re a male and 5’10” tall (70″ tall), then to be in the lower risk category, your waist circumference should be 35 inches or less.
If you’re a female and 5’6″ tall (66″ tall), then your waist circumference should be 33 inches or less.
But where should we measure waist circumference?
Is it where we wear our pants? Is it at the smallest part of our belly, where it dips in? Is it where our navel (belly button) is? Each one of these will produce very different results.
Measuring Waist Circumference
For the purposes of calculating risk associated with carrying excess weight around the middle, waist circumference and hip circumference need to be taken at very specific locations, as described below.
Using a flexible seamstress tape measure, stand in front of a mirror so that you can see both the front and back of where you are placing the tape measure.
It is also important that your belly is completely relaxed when taking the measurement, not sucked in. One way to do that is to taking a deep breath and let it out fully just as the measurement is taken.
Where to measure waist circumference
Take your waist circumference at the midpoint (i.e. half way) between your lowest rib and the top of your hip bone (called the ”iliac crest”) — being sure that the tape measure is perpendicular to the floor (i.e. not higher in the back or the front).
Looking at the graph above, one can see that for every little bit over 0.5, the risk rises steeply.
Where to Measure Hip Circumference?
Hip circumference is also needed for other assessors, including the waist to hip ratio. Measuring hips should be done at the widest part, making sure the tape measure is the same height in the front and the back.
How Much Should I Weigh?
People often ask me “how much should I weigh” – wanting me to provide them with a specific weight in pounds, or kilos. My usual answer is that when your waist circumference is half your height and your lab test results are optimal, everything else is aesthetics (what you look like). While I can provide a ball-park figure based on height and weight, how much people should weigh is better determined by them having the lowest risk of heart attack or stroke (cardiovascular disease) and the lowest amount of Years of Life Lost.
Health is not a number on the scale. Its the measurement of the amount of fat in our abdomen, around our liver, kidneys, pancreas and heart.
If your waist circumference is greater than 0.5 you are at risk. If you have been diagnosed with type 2 diabetes or pre-diabetes, high blood pressure or high cholesterol, then this risk is compounded. Add to that a family history of these metabolic diseases, and your risks are even higher.
While we can’t change our family history, we can change our diet and lifestyle and lower our risk.
Attaining a waist to height ratio of 0.5 is often associated with lower blood sugars, lower blood pressure and better cholesterol – even more so when the diet to achieve the weight loss is intentionally designed for these outcomes.
If you would like help getting on your own road to better health, please send me a note using the Contact Me form on this web page, and let me know how I can help.
Ashwell M, Gunn P, Gibson S (2012) Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev 13: 275—286
Ashwell M, Mayhew L, Richardson J, Rickayzen B (2014) Waist-to-Height Ratio Is More Predictive of Years of Life Lost than Body Mass Index. PLoS ONE 9(9)
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
There are some things that people should not do on their own and one of them is to begin a low carb or ketogenic diet without first consulting with their doctor, especially if they take certain types of medication. Medical supervision is absolutely required before a person changes the level of their carbohydrate intake if they are taking;
(1) insulin
(2) medication to lower blood glucose such as sodium glucose co-transporter 2 (SGLT2) medication including Invokana, Forxiga, Xigduo, Jardiance, etc. and other types of glucose lowering medication such as Victoza, etc.
(3) medication for blood pressure such as Ramipril, Lasix (furosemide), Lisinopril / ACE inhibitors, Atenolol / β-receptor antagonists
(4) mental health medication such as antidepressants, medication for anxiety disorder, and mood stabilizers for bipolar disorder and schizophrenia.
I don’t provide low carbohydrate dietary services those taking insulin (either Type 1 Diabetes or Type 2 Diabetes), but encourage those considering adopting this type of lifestyle to first consult with a healthcare professional with CDE certification, as well as their family doctor. This is very important because clinical studies indicate that insulin levels need to be adjusted downward very soon after beginning a low carbohydrate or ketogenic diet and this must be medically supervised.
I also recommend to those taking medication for mental health conditions that they consult with their psychiatrist and/or family practice physician before changing their diet. A low carb or ketogenic diet may have an effect on the dosage of medication required, especially with mood stabilizing medications such as Lithium. (A recent article written by Psychiatrist Georgia Ede, MD related to a ketogenic diet appeared in Psychology Today and appears here.)
Why do I advise people coming to me to implement a low carbohydrate or ketogenic lifestyle and taking medication to control their blood sugar or blood pressure first consult with their doctor before changing how they eat? It is because eating less carbohydrate can result in blood sugar levels and blood pressure coming down fairly soon afterward and this can have serious consequences if dosages of these medications are not monitored and adjusted downward (and often being discontinued entirely). For example, a sudden drop in blood pressure could result in people becoming dizzy or confused and could even result in injury to themselves or others if they ‘blacked out’ while walking or driving a car.
Some medications which lower blood sugar such as sodium glucose co-transporter 2 (SGLT2) medication including Invokana, Forxiga, Xigduo, Jardiance, etc. can result in life-threatening and even fatal cases of a very serious condition called “Diabetic ketoacidosis (DKA)” even with no change in diet, but these risks can be increased for patients on a very low carbohydrate diet as the combination of the medication and the low carb diet may increase the amount of ketone production (see Health Canada’s Safety Review here).
Those with significant alcohol consumption who are taking these medications are at risk for DKA, so it is very important that if you drink alcohol on a regular basis and take these medications to tell your doctor. If you are taking any of these medications and come to me, I will ask you about your alcohol consumption because alcohol and these medications together could potentially result in this serious and potentially life-threatening condition.
People taking any of the above medications (or any medications for other conditions) should not adopt a low carb or ketogenic lifestyle on their own without first checking with their doctor.
Another thing that people should never do on their own is adjust the dosage of any of their prescribed medication without first discussing it with their doctor. The consequences of doing so can be very serious, even life-threatening. Medication dosages and timing must be adjusted by a doctor.
Another condition which is less common than DKA but is very serious is Hyperosmolar Hyperglycemia State (HHS). It is life-threatening and has a much greater death rate than DKA, reaching up to 5-10%. It is most commonly seen in people with Type 2 Diabetes (T2D) that have some illness which results in reduced fluid intake, and them becoming seriously dehydrated. Being sick with an infection is one such situation where it is very important for you to see your doctor if you have T2D, so they can monitor you for HHS. You can read more about HHS here.
If you come to see me to adopt a low carb or ketogenic diet, I will work with you to coordinate dietary and lifestyle changes with your doctor, as they monitor your health and adjust the levels of prescribed medications. In more complex cases, I may ask for written consent to coordinate care with your doctor because depending on those medications, your doctor may need to know in advance what level of carbohydrates you have been advised to eat so that they can monitor your health and make adjustments in your medication dosage.
Your health is important and your diet and the medications need to be coordinated and overseen by your doctor. The potential risks are too great to attempt to do this on your own.
Do you have questions as to how I could work with you and your doctor as they oversee you adopting a low carb lifestyle? Feel free to drop me a note using the Contact Me form on the tab above.
To your good health!
Joy
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
For those who are curious about my background and how I came to practice and support the use of a therapeutic low carb and ketogenic diet, here is the interview that was done by Brian Williamson, from Ketovangelist just this past week (May 1 2018).
The interview lasts just over an hour (there’s a short commercial at the beginning and end of the interview) and begins with discussing my research, findings and publication in a peer-reviewed journal in the area of mental health nutrition (specifically micronutrient intake and dietary intake in ADHD) and how that research background contributed to my approach to using a low carbohydrate and ketogenic diet in therapeutic nutrition.
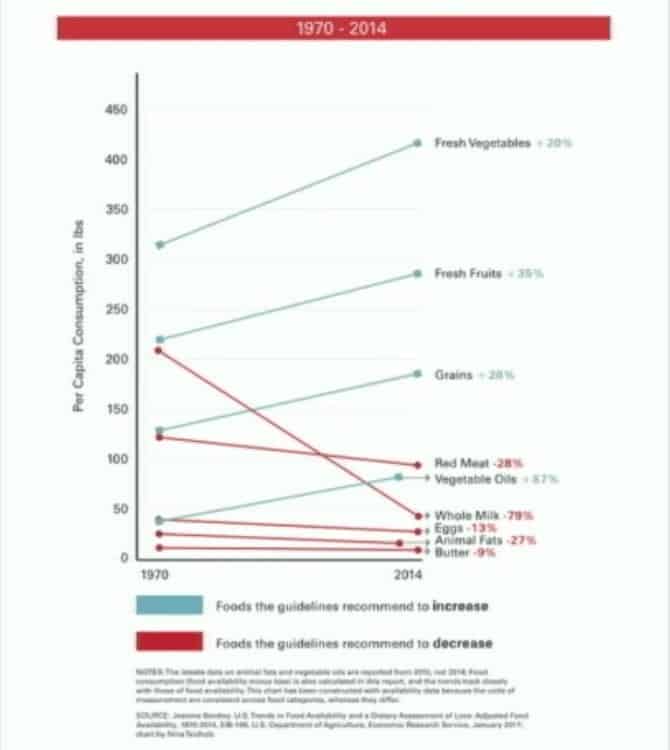
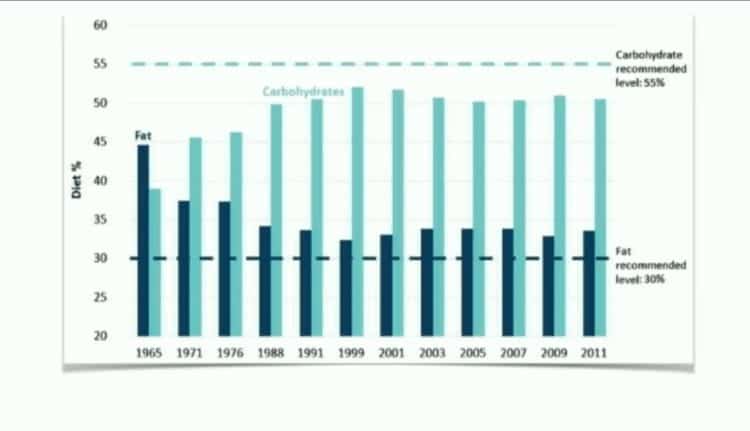
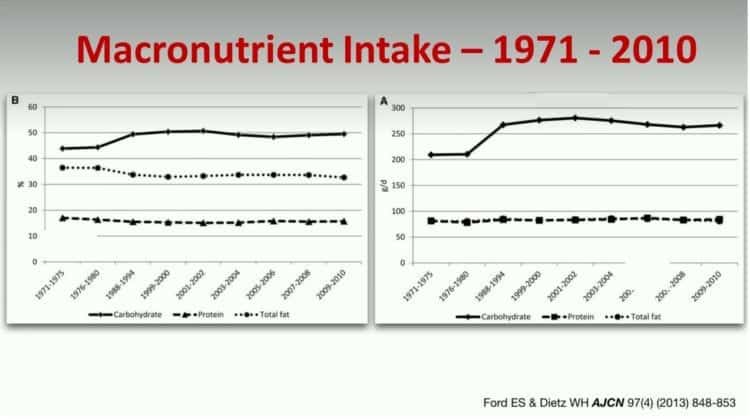
During the interview, Brian and I discussed several areas, including the politics of nutrition, changes in Dietary Guidelines in both the US and Canada in 1977, the obesity epidemic and the role that I see for individual nutrition in helping those with Type 2 Diabetes and insulin resistance and many of the associated conditions of high blood pressure, high triglycerides / abnormal cholesterol levels and obesity.
Special thanks to Brian Williamson for inviting me and to Chris, his editor for his post-production work.
I hope you enjoy the interview, and feel free to drop me a note through the Contact Me form, if you have any questions on how I can help you, either in-person or via Distance Consultation on Skype.
To our good health!
Joy
Keto 153 – Joy Kiddie interview on Ketovangelist
Please click the MP3 player bar above to listen to the interview.
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
When people are diagnosed with Type 2 Diabetes they are often sent for Diabetes education which teaches them, among other things to “choose starchy foods such as whole grain breads and cereals, rice, noodles, or potatoes at every meal” and that “good management of diabetes includes healthy eating, staying active and taking required medication [1]”. There is certainly a need for medication when blood sugar levels are not being controlled but what if in other cases, as Hippocrates has said food could be our medicine?
Food As Medicine
A therapeutic diet is involved in the management and treatment of many diseases and conditions. When someone is diagnosed with Celiac disease, for instance they are taught by a Dietitian to avoid gluten-containing foods because these cause damage to their intestines. A therapeutic diet for someone with Celiac disease involves them avoiding gluten-containing foods and beverages because eating them causes damage to their body.
A therapeutic diet for someone that is diagnosed with a food allergy often involves them avoiding eating that food and related foods that may also cause an adverse reaction. If a person is allergic to banana, for instance they may also react to pineapple, papaya or chestnuts. Except in the case of serious (anaphylactic) allergies, after a person has avoided those foods for a long time, a “food challenge” may be done to determine whether the person is later able to tolerate the foods in question, or not. Sometimes foods are able to be reintroduced later and other times, such as the case of Celiac disease, they cannot because to do so will result in damage to their body.
A therapeutic diet in someone diagnosed with Type 2 Diabetes involves limiting foods that result in too much insulin being released and/or that results in their blood sugar rising too high and too often. This may be for a period of time – after which something that can be likened to a ‘food challenge’ can be performed to determine whether there has been significant improvement or not and if so, which kinds of carbohydrate may be able to be re-introduced, in what quantities and with what frequency. More on that below.
Evidence Base for Using Dietary Carbohydrate Restriction in Diabetes Management
A Critical Review Article written by 26 authors and researchers appeared in the Journal of Nutrition in 2015 provided 12 points of evidence to support the use of low-carbohydrate diets as the first approach to treating Type 2 Diabetes. The summary of these points include that;
Hyperglycemia is the most salient feature of Diabetes and that dietary carbohydrate restriction has the greatest effect on decreasing blood glucose levels.
During the epidemics of obesity and Type 2 Diabetes, caloric increases have been due almost entirely to increased carbohydrates.
Benefits of dietary carbohydrate restriction do not require weight loss.
Although weight loss is not required for benefit, no dietary intervention is better than carbohydrate restriction for weight loss.
Adherence to low-carbohydrate diets in people with Type 2 Diabetes is at least as good as adherence to any other dietary interventions and is frequently significantly better.
Replacement of carbohydrate with protein is generally beneficial.
Dietary total and saturated fat do not correlate with risk for cardiovascular disease.
Plasma saturated fatty acids are controlled by dietary carbohydrate more than by dietary lipids.
The best predictor of microvascular and, to a lesser extent, macrovascular complications in patients with Type 2 Diabetes, is glycemic control (HbA1c).
Dietary carbohydrate restriction is the most effective method (other than starvation) of reducing serum TGs and increasing high-density lipoprotein.
Patients with Type 2 Diabetes on carbohydrate-restricted diets reduce and frequently eliminate medication (and people with Type 1 usually require lower insulin).
Intensive glucose lowering by dietary carbohydrate restriction has no side effects comparable to the effects of intensive pharmacologic treatment.
The authors provided strong support of the 12 points, concluding that there is a need for “reappraisal of dietary recommendations” which stems from;
1. The general failure to halt the epidemic of Diabetes under current
guidelines,
2. The specific failure of low-fat diets to improve obesity, cardiovascular
risk, or general health (points 1 and 4),
3. Constant reports of side effects of commonly prescribed
Diabetes medications, some quite serious (points 12),
4. Most importantly, the continued success of low carbohydrate
diets to meet the challenges of improvement in the features of Diabetes and metabolic syndrome in the absence of side effects.
The authors underscore that
“the benefits of carbohydrate restriction are immediate and well-documented.”
and that
“Concerns about the efficacy and safety of carbohydrate restriction are long term and conjectural rather than data driven. Most objections stem from the proposed dangers of total or saturated fat embodied in the so-called diet—heart hypothesis. At this point, the diet—heart hypothesis has had a record of very limited clinical or experimental success to support its position.”
As I’ve mentioned in past articles, a low carbohydrate diet is not new, but may in fact represent the diet followed by humans for much of our evolutionary history, prior to the rise of agriculture. Given the very positive outcomes of carbohydrate restricted diets, the authors conclude that people with Type 2 Diabetes should not be discouraged from following such a diet as is often the case, but rather that the strength of the evidence is that;
“current knowledge dictates that carbohydrate restriction should be a default treatment for Type 2 Diabetes and a default adjunct therapy for Type 1.”
The authors state that the insistent by those that object to the use of low carbohydrate diets on the basis that long-term randomized controlled trials are the only kind of data that will be accepted “is without precedent in science.”
“The seriousness of diabetes requires that we evaluate all of the evidence that is available. The 12 points are sufficiently compelling that we feel that the burden of proof rests with those who are opposed.’
Authors of this Review included:
Richard D. Feinman Ph.D, Department of Cell Biology, State University of New York
Wendy K. Pogozelski Ph.D, Department of Chemistry, State University of New York
Arne Astrup M.D., Department of Nutrition, Exercise and Sports, Copenhagen University
Richard K. Bernstein M.D., New York Diabetes Center, Mamaroneck, NY
Eugene J. Fine M.S., M.D., Department of Radiology (Nuclear Medicine), Albert Einstein College of Medicine, Bronx, New York
Eric C. Westman M.D., M.H.S., Duke University Medical Center, Durham, NC
Anthony Accurso M.D., Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore, MD
Lynda Frassetto M.D. Department of Medicine, University of California San Francisco, San Francisco, CA
Barbara A. Gower Ph.D. Department of Nutrition Sciences, University of Alabama at Birmingham, Birmingham, Alabama
Samy I. McFarlane M.D., Departments of Medicine and Endocrinology, State University of New York Downstate Medical Center, Brooklyn, NY
Jí¶rgen Vesti Nielsen M.D., Karlshamn, Sweden
Thure Krarup M.D. Department of Endocrinology I, Bispebjerg University Hospital, Copenhagen, Denmark
Laura Saslow Ph.D. University of California San Francisco, San Francisco, CA
Karl S. Roth M.D. Department of Pediatrics, Creighton University, Omaha, NE
Mary C. Vernon M.D. Private Practice, Lawrence, KS
Jeff S. Volek R.D., Ph.D. Department of Human Sciences (Kinesiology Program) Ohio State University, Columbus, OH
Gilbert B. Wilshire M.D. Mid-Missouri Reproductive Medicine and Surgery, Columbia, MO
Annika Dahlqvist M.D. Hí¤lsocentralen Centrum, Sundsvall, Sweden
Ralf Sundberg M.D., Ph.D. Private Practice, Malmí¶, Sweden
Ann Childers M.D. Private Practice, Lake Oswego, OR
Katharine Morrison M.R.C.G.P., Ballochmyle Medical Group, Mauchline, East Ayrshire, Scotland
Anssi H. Manninen M.H.S. Metabolia Oulu, Oulu, Finland
Hussain M. Dashti M.D., Ph.D., F.A.C.S., F.I.C.S., Faculty of Medicine, Department of Surgery, Kuwait university, Kuwait
Richard J. Wood Ph.D. Springfield College, Springfield, MA
Jay Wortman M.D. First Nations Division, Vancouver, BC, Canada
Nicolai Worm Ph.D. German University for Prevention and Health Care Management, Saarbrí¼cken, Germany
Blood Sugar Response in Healthy People vs Actual Responses in Individual Diabetics
We have the Glycemic Index (GI) which tells us how easily specific foods raise blood sugar in healthy people; specifically how much blood sugar will rise when a healthy person eats 50 g of that food and Glycemic Load (GL) tells us how healthy people respond to the carbohydrate in one serving of that food.
As outlined in the previous two articles titled “Not All Carbs Are Created Equal“, while brown rice and whole grain spaghetti may have a lower GI or GL than their white counterparts, they still result in a rapid rise in blood sugar even in healthy people. Would we expect brown rice or whole grain spaghetti to have any better a response in those with Type 2 Diabetes? Of course not, yet the recommendations are for those with Type 2 Diabetes to eat “starchy foods such as whole grain breads and cereals, rice, noodles, or potatoes at every meal“.
Given that the symptom of Type 2 Diabetes is that body can’t properly use the insulin that is released and as a result “sugar builds up in the blood instead of being used as energy” [1] – how does it make sense to recommend to someone with Type 2 Diabetes to “eat starchy foods such as whole grain breads and cereals, rice, noodles, or potatoes at every meal” because these “starchy foods are broken down into glucose, which your body needs for energy”[1]? Either the body can’t use the food as energy because of the dysfunction in insulin or it can.
In Type 2 Diabetes, the mechanism in which the body effectively uses carbohydrates for energy is ‘broken’ and body keeps making and releasing more and more insulin to try and bring glucose into the cells. Common sense would indicate that a therapeutic diet for someone with an intolerance to more than very small amounts of carbohydrate would be to limit foods that are high in carbohydrate, particularly those that cause a rapid spike in blood glucose even in healthy people.
We don’t need to guess how much a person with Type 2 Diabetes’ blood sugar is going to rise when they eat a food based on the GI or GL (which is based on healthy people) because we can test it in THEM!
As mentioned in the previous article, without spending any additional money on testing equipment, someone with Type 2 Diabetes can eat 25 g or 50 g of a carbohydrate-based food, test their blood sugar every half hour and know exactly how their body responds to it!They can seetheir blood sugar rise to 11 mmol/L(200 mg/dl) or 14 mmol/L(250 mg/dl) or 16.5 mmol/L(297 mg/dl) or higher in the first hour and KNOW. No guess work is required!
With the availability of relatively inexpensive Continuous Glucose Monitors (CGM) such as the FreeStyle Libre ($50 CDN) and one sensor worn for 2 weeks ($90), someone with Type 2 Diabetes can test 25 g or 50 g of specific carbohydrate-based food and KNOW exactly how their body responds!
Continuous Glucose Monitor (CGM) readings
People with Type 2 Diabetes can KNOW that 1/2 cup of whole grain rice or 1/2 of a baked potato (or some other food) resulted in their blood sugar spiking to 16.5 mmol/L(297 mg/dl) and know that this is not a food they tolerate even when eaten with a mixed meal that includes protein-based foods and non-starchy vegetables.
Guess work based on Glycemic Index or Glycemic Load – the blood sugar response of healthy people is no longer needed.
Role for a Therapeutic Low Carb Diet
Just as there is a role for a therapeutic diet in other food-related conditions such as food intolerance and Celiac disease, there is a role for a therapeutic diet in Type 2 Diabetes.
A person diagnosed with Type 2 Diabetes has (1) the inability to handle more than a very small carbohydrate load and (2) has cells which are insulin resistant, therefore it makes good clinical sense to design a therapeutic diet which enables them to lower their overall blood glucose response in order to enable the pancreatic beta cells that remain to begin to recover (these are the cells that produce insulin) and to allow their body cells which have become insulin resistant to become insulin sensitive again.
A Dietitian is knowledgeable to design such an therapeutic diet in such a ways as to include a wide variety of foodsthat supplies all the essential amino acids, fatty acids, vitamins and minerals that a person requires while containing only small amounts of carbohydrate at any given time.
Lab test results such as fasting insulin and fasting blood glucose (to calculate HOMA-IR) and tests of insulin response to a known glucose load (3 hour challenge) could be performed in time to monitor the degree of improvement in insulin sensitivity and pancreatic function or simply use existing routine lab tests such as TG:HDL ratio as a proxy, along with HbA1C and fasting blood glucose. This way, once a person’s body has begin to heal and restore some beta-cell function, a Dietitian can then design a customized therapeutic diet around each individual’s actual tolerance or intolerance to specific carbohydrates! We don’t need to rely on glycemic response data such as the GI or GL (which are based on healthy people) but can use an individual’s own blood sugar response!
We do this in other types of food intolerance by means of a “food challenge” and it is time we do this in Type 2 Diabetes as well.
With the advent of relatively inexpensive Continuous Glucose Monitors, we have the technology for individuals to do this easily with the help of a Dietitian, such as myself. It is more labour-intensive, but it can certainly be done using the standard blood glucose monitor that Diabetics already own and use by standardizing the size of the test food and testing blood sugar every 1/2 an hour for 3 hours.
It is long overdue for those with Type 2 Diabetes to be able to have therapeutic diets which are designed to improve their symptoms, rather than to expect them to eat carbohydrate loads they can’t handle, getting worse in time, then turning to medication to manage the disease. Type 2 Diabetes does not have to be “a chronic, progressive disease”.
Do you have questions how a low carb diet may be able to help you manage and improve the symptoms of Type 2 Diabetes?
Please send me a note using the ”Contact Me” form on this web page and I will respond shortly.
To our good health!
Joy
If you would like to read well-researched, credible ”Science Made Simple” articles on the use of a low carb or ketogenic diet for weight loss, as well as to significantly improve and even reverse the symptoms of Type 2 Diabetes, high cholesterol and other metabolic-related symptoms, please click here.
Richard D. Feinman, Wendy K. Pogozelski, Arne Astrup, Richard K. Bernstein, Eugene J. Fine, Eric C. Westman, Anthony Accurso, Lynda Frassetto, Barbara A. Gower, Samy I. McFarlane, Jí¶rgen Vesti Nielsen, Thure Krarup, Laura Saslow, Karl S. Roth, Mary C. Vernon, Jeff S. Volek, Gilbert B. Wilshire, Annika Dahlqvist, Ralf Sundberg, Ann Childers, Katharine Morrison, Anssi H. Manninen, Hussain M. Dashti, Richard J. Wood, Jay Wortman, Nicolai Worm,
Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base,
Nutrition,
Volume 31, Issue 1,
2015,
Pages 1-13,
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
INTRODUCTION: In the first article in this series on carbohydrates, I explained that Glycemic Index (GI) is a way to rate carbohydrates based how easily they raise the blood sugar of healthy people and that some carbohydrates are better than others when they cause much less of a rise in blood sugar. I wanted to know how would I react to carbohydrate-based foods now that I have been eating low carb for so long (>1 year) and have seen a partial reversal of symptoms of the Type 2 Diabetes that I’ve had for more than 10 years.
I decided to conduct some impromptu ‘experiments’ and the results led to some reading in the literature. The information I discovered is VERY exciting for me and for others with Type 2 Diabetes or Insulin Resistance.
Once people have achieved significant reversal of symptoms following a therapeutic low carb or ketogenic diet, there is a way to begin to re-introduce carb-based foods in a way that does not cause their blood sugar to spike.
As you may recall from the first article in this series on Carbohydrates, the Glycemic Index of a food is determine by having healthy people eat 50 grams of digestible carbohydrate of a given food, and then measure their blood glucose response over a 2 hour period (30 minutes, 60 minutes, 90 minutes, 120 minutes), plotting the curve then measuring the area under the curve (AUC) and comparing it to the AUC of pure glucose, the reference food.
The problem with the Glycemic Index or even the Glycemic Load (based on individual serving sizes) is that this data does not apply to those with Diabetes or Insulin Resistance.
Since I have been Diabetic for a long time, I decided to go about conducting my own sample-set-of-one (n=1) ‘experiment’, and one thing led to another…
The ‘Test Food’
I ate 1/2 cup of chickpeas (cooked from dried) which has 25 g of carbohydrate and measured my blood sugar response with the same meter at 30 minutes, 60 minutes, 90 minutes, 120 minutes, 180 minutes and 210 minutes.
blood glucose response to 25 g of chickpeas, cooked from dried
At the time I did this, I hadn’t eaten in 8 hours (considered a fasted state) and my starting blood sugar was 4.8 mmol/L (86 mg.dl). The chickpeas were part of a mixed meal with some chicken (high biological value protein) and a cucumber salad with olive oil.
At the highest point, my blood sugar went up to 5.8 mmol/L (105 mg/dl), stayed there, then started to drop at 2 hours.
I was amazed.
When I first began changing my lifestyle a year ago, even eating low GI foods such as chickpeas caused my blood sugar to jump dramatically. I recall the first few months when I would eat 1 cup of hummus, which is chickpeas with tahini (ground sesame seeds) and has even more fiber than chickpeas alone and also has only 25 g of carbs, my blood sugar would always go up to ~ 8.6 – 8.9 mmol/L (155- 160 mg/dl).
This was a HUGE improvement after not eating more than 30 g of carbohydrate per day (i.e. a ketogenic diet) for the last 6 months!
The ‘Reference Food’
Two weeks ago, I was at a social occasion where a milk-chocolate covered cracker was served and I decided (in the interest of science, of course!) to read the nutritional label, measure out exactly 25 g of carbohydrate of this food and eat it, measuring my blood sugar at 0 minutes, 60 minutes, 90 minutes, 120 minutes, and 180 minutes.
This ‘reference food’ (high GI) was eaten after a dinner that had a fair amount of high biological value protein (steak) as well as some healthy fats (olive oil on vegetables) and fiber in the vegetables, and my starting blood sugar was 6.7 mmol/L (121 mg/dl).
Just look at the blood sugar spike!
When I ate 25 gm of carbohydrate as the cracker and chocolate, my blood glucose went from 6.7 mmol/L to 9.8 mmol/L (121 mg/dl -177 mg/dl)! That is, I had eaten the SAME amount of carbohydrate (25 g of carbs) as when I ate the cooked chickpeas and had THREE TIMES the blood sugar response!!
Both the meals I ate just before the ‘reference food’ (high GI, highly refined cracker with chocolate) and the ‘test food’ (low GI, intact chickpeas) had a high biological value protein (chicken, steak) which slows the blood sugar response of the body, and both had the same amount of fiber (the exact same salad).
Below is a graph of the two responses (chickpeas in blue, chocolate covered cracker, orange) over 3+ hours.
It is quite evident that 25 g of carbs as white flour with milk chocolate (refined carbs) is processed VERY differently by my body than 25 g of carbs such as whole, intact chickpeas!!
Comparison of blood glucose response of 25 g of carbohydrate as chickpeas and white flour cracker with chocolate (special thanks to Phil Thompson of the “Lower Insulin” Facebook group for the graph and calculations of area under the curve)
The area under the curve (AUG) was determined by lowering the cracker and chocolate curve down to sit just above the chickpea curve (grey curve) and then assessing where the respective points were and running the AUG formula relative to baseline.
The AUG of 25 g of carbs as chickpeas was 129.
The AUG of 25 g of carbs as white flour cracker with chocolate was 381.
The difference was 2.95.
The blood sugar response of the cracker with chocolate was THREE TIMES GREATER than the blood sugar response of the chickpeas – and both contained 25 g of carbs!
Some carbs are quite clearly better than others for this Type 2 Diabetic.*
* As I will elaborate on below, people’s blood sugar response to different carbohydrate-based food is quite individual.
Objective Data
Facsimile for Glycemic Index of Cracker with Chocolate
I was able to find for purposes of estimation, that 25 g of carbohydrate as white bread with 5 g of margarine (a pretty good facsimile for 25 g of carbohydrate as white flour cracker covered with milk chocolate made with palm oil) has a GI of 70.1 when compared to the reference which was 25 g glucose in 125 ml water [1].
Studies of Effect of Eating Legumes (Pulses) Alone
A meta-analysis of 10 studies on the effect of pulses (legumes) eaten alone on blood sugar control in people with and without Diabetes [2] provided some helpful information. The pulses in the meta-analysis included chickpeas, black-eyed peas and various other beans (including red and white kidney, black, pinto, fava and white navy).
Seven of the 10 trials that looked at the effect of eating pulses alone had a crossover design (five had a washout period), studied a total of 253 participants, of which only 21 had Type 2 Diabetes, and 232 that had normal blood sugar.
Background diets were largely high-carbohydrate, low-fat diets (carbohydrate 52% of energy, protein 18% of energy, fat 29% of energy).
Due to the length of time I have had Type 2 Diabetes and the very high degree of persistent insulin resistance over the first 6 months of eating low carb but not ketogenic, the last 6 months my diet has been very low in carbohydrate (5-10% of energy), moderate in protein ~23% and 67-77% healthy fats.
It was found that fasting blood glucose following the eating of pulses alone was decreased by 0.82% (95% CI ), but there was no long term effect on HbA1C (3 month average blood sugar) or on HOMA-IR (fasting blood glucose: fasting insulin).
[Of interest, in low GI diets, eating of pulses lowered HbA1C (3 month average blood sugar) by 0.28% but had no change on fasting blood sugar or HOMA-IR. The average GI of the pulse-containing low-GI diets was 67 and as compared to the GI value of bread alone.]
The conclusions of the meta-analysis found that the strongest modifiers of benefit were in Type 2 Diabetes and that the legumes that modified blood sugar the most were black beans, white/navy beans, pinto beans, red and white kidney beans, chickpeas and fava beans.
“Specific to the pulses alone analysis, pulse species including Phaseolus vulgaris (black, white, pinto, red and white kidney beans), Cicer arietinum (chickpeas) and Vicia faba (fava beans) were also identified as significant modifiers.” [2]
Individual Glycemic Response – role for personalized nutrition
A 2015 study from Israel[3] with 800 people who were monitored with continuous glucose monitors indicates that there isn’t a ‘universal’ blood sugar response to low GI foods or high GI carbs –that glycemic (blood sugar) response is very individual.
“We continuously monitored week-long glucose levels in an 800-person cohort, measured responses to 46,898 meals, and found high variability in the response to identical meals, suggesting that universal dietary recommendations may have limited utility.
The study also found that an individual’s blood sugar response to different foods was able to be predicted by type and amounts of bacteria in their intestines (the ‘gut biome’ / ‘microbiome’ / ‘microbiota’) .
Based on the data they collected, the team has since created and validated a machine-learning algorithm that combines blood parameters, dietary habits, anthropometrics (height, weight data), physical activity and gut microbiota data that they say accurately predicts a person’s individual post meal blood sugar response to actual meals.
Applications in Dietetic Practice for Personalized Nutrition
There is a tremendous opportunity for Dietitians such as myself to help individuals with Type 2 Diabetes or pre-diabetes determine which carbohydrate-based foods cause the lowest, most gradual rise in blood sugar.
This is huge!
This means that after individuals have had significant reversal of Type 2 Diabetes / Insulin Resistance following a therapeutic low carb or ketogenic diet for a period of time, I can help them re-introduce carb-based foods into their diet by selecting ones that have the least impact on their blood sugar!
There are two ways this can be done;
USING EXISTING BLOOD GLUCOSE METER – I can help those with Type 2 Diabetes eat a specific amount of a ‘test food’ that contains 50 g of carbohydrate (I will calculate this for them) and have them test their blood sugar every 30 minutes for 2 or 3 hours with the blood glucose meters they already have. Then, I can take that data, enter it into an Excel sheet just as was done with my data above, and determine their blood sugar response.
USING A CONTINUOUS GLUCOSE MONITOR – continuous glucose monitors (CGMs) such as the FreeStyle Libre have become relatively inexpensive and would be ideal for this kind of testing. Test strips for most standard home blood glucose monitors are $1 a piece, so testing every 30 minutes for 3 hours costs $6. The FreeStyle Libre costs $50 for the unit, and while test patches are $90 and last only two weeks, huge varieties of carbohydrate-based foods can be tried and measured in a short time, with no effort.
As a Dietitian I can not only help individuals carry out this kind of individual testing of carbohydrate-based foods, I can help them interpret the results as we begin to re-introduced some foods back into the diet once significant reversal of insulin resistance has been accomplished through the therapeutic use of a low carbohydrate or ketogenic diet.
Have questions how I can help you reverse insulin resistance by following a therapeutic low carb diet? Have you been following a low-carb or ketogenic diet for a while and want to begin determining which carb-based foods don’t spike your blood sugar? I can help.
Please send me a note using the “Contact Me” form on this web page and I will respond shortly.
Aston LM, Gambell JM, Lee DM, Bryant SP, Jebb SA. Determination of the glycaemic index of various staple carbohydrate-rich foods in the UK diet. European journal of clinical nutrition. 2008;62(2):279-285.
Sievenpiper, J.L., Kendall, C.W.C., Esfahani, A. et al. Effect of non-oil-seed pulses on glycaemic control: a systematic review and meta-analysis of randomised controlled experimental trials in people with and without diabetes. Diabetologia (2009) 52: 1479.
Zeevi D, Korem T, Zmora N, et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell. 2015 Nov 19;163(5):1079-1094.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
In the introduction to this series on Carbohydrates, I explained that Glycemic Index (GI) is a way to rate carbohydrates based how easily they raise blood sugar. If you recall, low GI foods (those with a value of 55 or less) are more slowly digested, absorbed and metabolized and cause a lower and slower rise in blood glucose levels and very high GI foods (>70) are digested very rapidly, casing a large spoke in blood sugar. High GI foods (>55) are result in a fairly rapid rise in blood sugar.
The GI value of a food is determined comparing how healthy people’s blood sugar responds over a two hour period to a food containing 50 grams of digestible carbohydrate from that food compared to 50 grams of glucose (pure sugar). The drawback to this rating scale is that the values are only known for a serving that has 50 grams of carbs in it. That is, they compare the ability for different foods containing the SAME amount of carbohydrate it (50 g) to raise blood sugar. The problem with the Glycemic Index is that its hard to compare foods because a serving size may have considerably less than 50 g of carbs in it. For example, the Glycemic Index of watermelon is 76, which is as high as the Glycemic Index of a doughnut, but one serving of watermelon (1/2 a cup) has 11 g of carbohydrate in it, while a medium doughnut (one serving) has 23 g of carbs.
This is where the concept of Glycemic Load (GL) is much more helpful, because it tells us how a healthy person’s body will respond to the carbs in one serving of a food. One usual serving of a food would be considered to have a very high Glycemic Load if it is ≥20, a high Glycemic Load if it is between 11-19 and a low Glycemic Load if it is ≤10.
How to Determine Glycemic Load
To determine Glycemic Load (GL) of a serving of a food, what needs to be known is:
The Glycemic Index (GI) of that food (found by referring to a table of Glycemic Indexes)
The number of grams of carbohydrate in the quantity of food considered to be one serving.
GL = GI x (amount of carbohydrate per serving) / 100
For purposes of comparison, let’s look at the Glycemic Load of the same foods we looked at the Glycemic Index for in the first article.
One slice of white bread has a Glycemic Load of 10 and so does one slice of whole wheat bread, which is considered low. Both have 15 g of carbs per slice.
One 1 cup of cooked white spaghetti has a Glycemic Load of 25 which is considered very high and while 1 cup of whole grain spaghetti only has a Glycemic Load of 14, this is still not low, just lower than white spaghetti.
A cup of boiled white rice has 53 g of carbs in it and has a very high Glycemic Load = 35. A cup of white spaghetti has 44 g of carbs in it and also has a very high Glycemic Load at 25. These foods are high in carbohydrate and will cause a rapid rise in blood sugar in healthy people. To those who are already Diabetic or pre-Diabetic this is a big problem.
One cup of cooked whole grain spaghetti has a Glycemic Load of 14 which is still not low and has 37 g of carbs in it.
A cup of boiled brown rice has a Glycemic Load of 20 which is still considered very high and has 42 g of carbs. These foods are high in carbohydrate and will cause a fairly rapid rise in blood sugar in healthy people, let alone those who are already having problems.
So what’s the problem?
Eating a high Glycemic Load diet over a period of years and years will result in blood sugar after meals (called post prandial blood glucose) to be high. This puts a huge demand on the body to keep releasing insulin to try to move all that glucose into the body’s cells and get it out of the blood. Over time, a high Glycemic Load diet causes the body’s pancreas β-cells (beta cells) to decrease in function or in many cases, to die, resulting in a diagnosis of Type 2 Diabetes. As can be seen above, even eating the “whole grain” version of favourite foods does not necessarily reduce the insulin demand on our pancreas. Our β-cells are under continual pressure to release insulin every time we eat – from our breakfast toast or cereal, to our mid-morning muffin, to our pasta lunch. Eating a low carb diet is a very effective way to lower the demand on our pancreas to keep producing and releasing insulin to deal with the constant spikes in our blood sugar from carbohydrate containing foods. But does that mean we need to remain eating a low carb diet forever? More on that in future articles in this series.
Glycemic Load will tell us how much a serving of food will increase our blood sugar but it doesn’t tell us how much insulin our body releases as a result of eating a food – that is, the demand we are putting on our pancreatic β-cells.
For those that have been eating a high carbohydrate diet for years and years or have a family history of Type 2 Diabetes, knowing how much insulin is needed to process the carb -based foods we eat is hugely important, because we need to eating foods that do not put a large demand on our pancreatic β-cells. For those that already have Type 2 Diabetes, it is especially important to eat in such a way as to preserve whatever β-cell function we have left! Referring to the Insulin Index enables us to choose between carb-based foods based on the demand they put on our β-cells.
If you have questions as to how I can help you choose foods that result in much less glucose being released and also put much less demand on your β-cells to keep producing and releasing insulin, please send me a note using the “Contact Me” form located on the tab above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
INTRODUCTION: Not all carbs are created equal; some are broken down very quickly into simple sugars and others are broken down very slowly. In the past the terms “simple sugar” and “complex carbohydrate” were used to imply this concept there are newer terms that enable us to know how much eating these foods will raise blood glucose in healthy people. The “in healthy people” is important, as the ability to tolerate carbohydrate in those with insulin resistance (“pre-diabetes”) or Type 2 Diabetes is significantly affected.
This is the first article in a new series on carbohydrate.
Glycemic Index
The Glycemic Index (GI) is a way of rating carbohydrates based on their ability to raise blood sugar.
Low GI foods (those with a value of 55 or less) are more slowly digested, absorbed and metabolized and cause a lower and slower rise in blood glucose levels and very high GI foods (>70) are digested very rapidly, casing a large spoke in blood sugar. High GI foods (>55) are result in a fairly rapid rise in blood sugar. Keep in mind that Glycemic Index only indicates how slowly or quickly foods will increase blood sugar, not how much higher blood sugar will go
Many of the foods people eat lots of in our society, such as bread, rice, pasta and cereal, even vegetables, are high GI foods. As once healthy people continue to eat these foods on a regular basis, they put a high demand on their body to produce and release insulin, which brings all that glucose into their cells. This insulin is released from the beta cells in the pancreas and people eating these high GI foods means that their beta cells have to release insulin over and over all day long and this constant demand on the beta cells, over time, results in the cells throughout their body becoming insulin resistant (no longer responding to insulin’s signal) or burning out their beta cells, resulting in Type 2 Diabetes.
Many people don’t realize that by the time they are diagnosed with Type 2 Diabetes, they already have beta cell dysfunction, beta cell death and/or a decrease in beta cell mass. Once beta cells die, they’re gone. Our once healthy body is no longer healthy. When we eat foods with significant carbohydrate – especially high GI carbohydrates, our ability to release insulin is significantly impacted and as a result, we can no longer tolerate carbs like we used to. While the mechanism is different, it’s similar to someone that becomes intolerant to gluten; once they’re celiac, they can no longer tolerate foods that contain gluten without causing damage to their body. Depending how long someone had Type 2 Diabetes when they were finally diagnosed, or how long they had it before they changed their eating habits will all factor in to how much carbohydrate they can process. For this reason, each person is different.
It’s not that carbs are inherently “bad”. It’s that our bodies are no longer able to process some of them they way we could when we were still healthy – so in those cases the sugar stays in our blood, damaging tissues throughout our body.
Knowing which carbs are high GI is important, because these are the foods that tax our already overtaxed beta cells if we are not Diabetic and limiting these foods significantly, or avoiding may be the best way for healthy people to remain healthy.
The good news is that there are some types of carbohydrates that some people can not only tolerate, but may actually improve their blood sugar control, and that’s the topic of an upcoming article.
How the GI of a Food is Determined
The GI value of a food is determined by feeding a group of healthy people the amount of a food that contains 50 grams of digestible (available) carbohydrate and then measuring the effect on their blood glucose levels over the next two hours. The area under their two-hour blood glucose response (glucose AUC) for this food is then measured.
At another time, the same group of healthy people eat 50 grams of glucose, (which is the reference food) and their two-hour blood glucose response is also measured.
The GI value for the test food is calculated for each person in the group by dividing their glucose AUC for the test food by their glucose AUC.
The final GI value for the test food is the average GI value all the people in the group.
In summary to determine the Glycemic Index of a food healthy (non-diabetic) people;
(a) eat 50 grams of digestible carbohydrate of a particular food
(b) measure their blood glucose response over a 2 hour period
(c) plot the curve and measure the area under the curve (AUC)
(d) compare that AUC of the test food to the AUC of pure glucose (i.e. produced when the same people eat 50 g of glucose, which is the reference food.
Too Much of a ‘Good’ Thing
Many of the foods that people in the West enjoy and eat a lot such as bread, rice and noodles are High GI foods – these are ones that are rated at ≥ 55 (compared to pure glucose, which is rated at 100).
White bread has a GI of 75 ± 2 and whole wheat bread isn’t much better, at 74 ± 2.
Boiled white rice is high GI at 73 ± 4, and while somewhat better boiled brown rice is still high GI at 68 ± 4.
White spaghetti has a GI of 49 ± 2 and whole grain spaghetti has a GI of 48 ± 5.
Rice noodles, such as those in Pho (Vietnamese Beef Noodle soup) are even higher, at 53 ± 7.
Breakfast cereals, whether boxed or cooked are also high GI. Here is a table that summarizes some of these [1];
BREAKFAST CEREALS
Glycemic index (glucose = 100)
Cornflakes
81 ± 6
Wheat flake biscuits
69 ± 2
Porridge, rolled oats
55 ± 2
Instant oat porridge
79 ± 3
Muesli
57 ± 2
Many people include vegetables such as potato, sweet potato and squash such as pumpkin in their “vegetable quota” for the day, but let’s look at the Glycemic Index for these;
VEGETABLES
Glycemic index (glucose = 100)
Potato, boiled
78 ± 4
Potato, instant mash
87 ± 3
Potato, french fries
63 ± 5
Carrots, boiled
39 ± 4
Sweet potato, boiled
63 ± 6
Pumpkin, boiled
64 ± 7
People in our culture eat a lot of bread, rice, pasta, starchy vegetables and cereal but one of the things we know is that eating them with good source of protein slows down how quickly they affect blood sugar. Oftentimes bread and cereal form the basis of breakfast, perhaps with a high GI glass of juice and frequently, people eat pasta with a tomato sauce for supper (or leftovers for lunch), and this kind of meal will spike their blood sugar. We also know that the fiber content of a mixed meal will also slow down the rate at which blood sugar rises from these carbs, so there are ways to ‘tone down’ the response.
Some Final Thoughts…
If you have a family history of Type 2 Diabetes, are overweight or have high blood sugar, it’s important to understand that what you eat matters and to eat in a way that does not put high demand on your beta cells to keep releasing insulin to process all that glucose.
The time to consider the effect on your body is now – before you get sick by having overtaxed your pancreas’ beta cells and experience beta cell death or mass loss and are diagnosed with Type 2 Diabetes.
Once we’ve crossed that threshold; once our once healthy body is no longer healthy, we need to learn to eat in a way that does not put high demand on our beta cells, that does not require our body to process large amounts of glucose at a time, in order to preserve whatever beta cell mass and function we have left.
Determining which carb-containing foods we can tolerate and in what quantities will enable us to eat in a way that keeps us from getting worse and keeps us from developing the very serious consequences of not doing so, which can include blindness, toe and food amputations and more.
In coming articles, I’ll explain Glycemic Load and the Insulin Index and I’ll also touch on a role for legumes (pulses) such as chickpeas and sources of “resistant starch” in a moderate carb ‘Mediterranean-style’ diet.
If you just found out you are pre-diabetic, now is the time to do something about it. Waiting will not make it better.
If you’ve been recently be diagnosed with Type 2 Diabetes, it’s not too late. Studies have shown that changing eating habits and lifestyle soon after diagnosis makes it possible for some people to reverse their symptoms and to have their Diabetes go into remission. One thing is known, that doing nothing will bring needless firsthand understanding to the phrase that “Diabetes is a chronic, progressive disease”. It doesn’t have to be.
If you want to know how I can help you, please send me a note using the “Contact Me” form located on the tab above.
Also see: Atkinson FS, Foster-Powell K, Brand-Miller JC, “International tables of glycemic index and glycemic load values”, Diabetes Care 31(12); 2281-2283
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
The recently released 2018 Clinical Practice Guidelines (CPG) Guidelines of Diabetes Canada recommend that those with Diabetes continue to eat 45% to 65% of their daily calories as carbohydrate, 10% to 35% of their daily calories as protein and only 20% to 35% of their daily calories, yet affirm that there is “evidence to support a number of other macronutrient-, food- and dietary pattern-based approaches” and that “evidence is limited for the rigid adherence to any single dietary approach”[1] .
One of the dietary patterns they recommend is a “Mediterranean-style dietary pattern” in order to “reduce major cardiovascular events and improve glycemic (blood sugar) control.”
So what is a “Mediterranean-style dietary pattern”?
According to the Clinical Practice Guidelines,
A ”Mediterranean diet” primarily refers to a plant-based diet first described in the 1960s. General features include a high consumption of fruits, vegetables, legumes, nuts, seeds, cereals and whole grains; moderate-to-high consumption of olive oil (as the principal source of fat); low to moderate consumption of dairy products, fish and poultry; and low consumption of red meat, as well as low to moderate consumption of wine, mainly during meals”
Countries with coastlines on the Mediterranean Sea include Albania, Algeria, Bosnia and Herzegovina, Croatia, Cyprus, Egypt, France, Greece, Israel, Italy, Lebanon, Libya, Malta, Morocco, Monaco, Montenegro, Slovenia, Spain, Syria, Tunisia and Turkey and the diets of these countries vary considerably, so there isn’t only ONE “Mediterranean Diet”.
What is the Mediterranean Diet that the Clinical Practice Guidelines are referring to?
It would seem that they are referring to dietary intake based of southern Italy from the 1960s from when rates of chronic disease were reported to be amongst the lowest in the world and adult life expectancy was reported to be amongst the highest. That is, the health benefits of “The Mediterranean Diet” came out of Ancel Keys’ Six Country Study (1953) and later his Seven Countries Study (1970). More on that below.
One of the academic papers that the Guidelines cites as the basis for a “Mediterranean diet” makes the direct link to Ancel Keys clear;
“Ecologic evidence suggesting beneficial health effects of the Mediterranean diet has emerged from the classic studies of
Keys.” [2]
In 1953, Ancel Keys published the results of his ”Six Countries Study”[3], where it is said he demonstrated that there was an association between dietary fat as a percentage of daily calories and death from degenerative heart disease.
Four years later, in 1957, Yerushalamy published a paper with data from 22 countries [4], which showed a much weaker relationship between dietary fat and death by coronary heart disease than was suggested by Keys’s six country data (see below).
from [3].Keys, A. Atherosclerosis: a problem in newer public health. J. Mt. Sinai Hosp. N. Y.20, 118—139 (1953).from [4] Yerushalmy J, Hilleboe HE. Fat in the diet and mortality from heart disease. A methodologic note. NY State J Med 1957;57:2343—54
Nevertheless, in 1970, Keys went on to publish his Seven Countries Study in which he maintained that there was an associative relationship between increased dietary saturated fat and Coronary Heart Disease – ignoring the data presented in Yerushalamy’s 1957 study and failing to study countries such as France, in which the relationship did not hold.
In Keys’ paper published in 1989 [5] which was based on food consumption patterns in the 1960s in the seven countries, he found that the average consumption of animal foods (with the exception of fish) was positively associated with 25 year Coronary Heart Disease deaths rates and the average intake of saturated fat was strongly related to 10 and 25 year CHD mortality rates. Keys published this study 32 years after Yerushalamy’s 1957 paper which showed a significantly weaker relationship, yet it seems that people only remember Key’s data.
Countries with coastlines on the Mediterranean Sea on which there was known dietary and disease data in 1957 and that Keys later ignored in 1970 included France (labelled #8 on Yerushalamy’s graph above) and Israel (labelled #11). France is known for the “French paradox” (a term which came about in the 1980s) because of their relatively low incidence of coronary heart disease (CHD) while having a diet relatively rich in saturated fats. According to a 2004 paper about the French Paradox, there was diet and disease data available from the French population that was carried out in 1986—87 and which demonstrated that the saturated fat intake of the French was 15% of the total energy intake, yet such a high consumption of saturated fatty acids was not associated with high Coronary Heart Disease incidence in France [6]. Nevertheless, Keys published his 1989 study [5] ignoring the French dietary and disease data that was available from 1986-1987 [6]. Was it because it didn’t fit his hypothesis?
The diet of the French in the 1960’s was every bit a “Mediterranean Diet” as that of southern Italy, but since Ancel Keys ignored (or did not study) the French data in the 1960s, that “Mediterranean Diet” remains ignored in the guidelines of today.
According to the French Paradox paper, high saturated fat intakes combined with low Coronary Heart Disease rates were also observed in other Mediterranean countries, including Spain and that rates in other non-Mediterranean Europeans countries such as Germany, Belgium are similar [6].
Perhaps then, a ‘true’ Mediterranean Diet which is protective of Coronary Heart Disease ought not to be defined as being largely “plant-based” and “low in consumption of red meat and dairy” – which the French diet clearly is not, but rather should focus on being a diet high in consumption of specific types of vegetables and fruit, nuts and seeds, abundant in the use of olive oil and that includes regular consumption of wine with meals.
As outlined in a recent article, eight recent meta-analysis and systemic reviews which reviewed evidence from randomized control trials that had been conducted between 2009-2017 did not find an association between saturated fat intake and the risk of heart disease. As well, recently published results from the Prospective Urban and Rural Epidemiological (PURE) Study, the largest and most global epidemiological study carried out to date and published in the Lancet in December 2017 found that those who ate the largest amount of saturated fats had significantly reduced rates of mortality (death) and that low consumption of saturated fat (6-7% of calories) was actually associated with increased risk of stroke.
Also as described in a recent article, a study published at the end of March 2017 in Nutrients and which examined health and nutrition data from 158 countries worldwide found that total fat and animal fat consumption were least associated with the risk of cardiovascular disease, and that high carbohydrate consumption, particularly as cereals and wheat was most associated with the risk of cardiovascular disease – with both of these relationships holding up regardless of a nation’s average national income.
Final Thoughts…
The 2018 Clinical Practice Guidelines continue to recommend the health benefits of a “Mediterranean style diet” defined based on the 60-year-old-data of Ancel Keys’ Six Countries Study / 50 year old Seven Countries Study- when we now know that Keys excluded data that was available from countries including France, which did not fit his hypothesis.
Given that there seems to be increasing evidence that Keys’ Diet-Heart Hypothesis (the belief that dietary saturated fat causes heart disease) has been significantly challenged by newer data, is it not time to study the factors in the diet of this region that ARE protective against cardiovascular disease, and to redefine a Mediterranean diet in these terms?
Would you like to have a Meal Plan that emphasizes the foods of this region, including meat and cheese, fish and seafood, vegetables and fruit, nuts and seeds, olive oil and wine and which may play a protective role in heart heath?
Please send me a note using the Contact Me form located on the tab above, and I will reply as soon as possible.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Diabetes Canada has released their long-awaited 2018 Clinical Practice Guidelines [1] which affirms that nutrition therapy is an integral part of people’s self-management of their Diabetes, as well as part of the treatment for the disease. One of the main goals of nutrition therapy is to maintain or improve the quality of life and nutritional and physical health of those with the disease, while preventing the need to treat both sudden (acute) and long term complications. Effective nutrition therapy can improve blood sugar control, including reducing three-month average blood glucose (i.e. HbA1C, glycated hemoglobin) by 1.0% to 2.0%.
Diabetes Canada 2018 Clinical Practice Guidelines
The new Guidelines mention that since Canada has wide ethnic and cultural diversity, with each group having their distinct foods, preparation methods, and dietary patterns and lifestyles. Effective nutritional therapy needs to take these cultural variations into account and needs to be individualized; specific to the individual, their age, the duration they’ve had type 2 diabetes, their goals, personal values and preferences, along with their individual need, lifestyle and economic situation. They recognize that nutrition therapy for those with Diabetes is not “one-size-fits-all”.
“Nutrition therapy should be individualized, regularly evaluated, reinforced in an intensive manner and should incorporate self-management education. A registered dietitian (RD) should be involved in the delivery of care wherever possible.”
The Nutrition Therapy Guidelines recommend that those with Diabetes follow the recommendations of Eating Well with Canada’s Food Guide;
“The starting point of nutrition therapy is to follow the healthy
diet recommended for the general population based on Eating Well With Canada’s Food Guide.”
They recommend that those with Diabetes continue to eat 45% to 65% of their daily calories as carbohydrate, 10% to 35% of their daily calories as protein and only 20% to 35% of their daily calories as fat, yet at the same time say that “the ideal macronutrient distribution for the management of diabetes can be individualized”;
“The ideal macronutrient distribution for the management of diabetes can be individualized. Based on evidence for chronic disease prevention and adequacy of essential nutrients, the DRIs (Dietary Reference Intakes) recommend acceptable macronutrient distribution ranges (AMDRs) for macronutrients as a percentage of total energy. These include 45% to 65% energy for CHO, 10% to 35% energy for protein and 20% to 35% energy for fat.”
They recommend that those with Diabetes continue to follow the same macronutrient distribution (percent of carbs, protein and fat) as the general population because it
“may help a person attain and maintain a healthy body weight while ensuring an adequate intake of carbohydrate (CHO), fibre, fat, protein, vitamins and minerals.”
What is encouraging is that they also have said that there is evidence to support a number of other macronutrient-, food- and dietary pattern-based approaches and advise against any rigid adherence to any one approach;
“There is evidence to support a number of other macronutrient-, food- and dietary pattern-based approaches. As evidence is limited for the rigid adherence to any single dietary approach, nutrition therapy and meal planning should be individualized.”
These Guidelines leave it open to individuals to choose other dietary approaches and outline a number of those approaches in the body of the text and in a summary table (Table 1). Figure 1 and Figures 2 and Table 1 in the Clinical Practice Guidelines (below) present an algorithm that summarizes the approach to nutrition therapy for diabetes which includes;
“allowing for the individualization of therapy in an evidence-based framework”.
Table 1: Properties of Dietary Intervention – Diabetes Canada 2018 Clinical Practice Guidelines
The new Diabetes Canada guidelines recognize that the ideal macronutrient distribution (the ratio of carbs, protein and fat) may vary and depend on, amongst other things, the individual’s values and preferences;
“The ideal macronutrient distribution for the management of diabetes may vary, depending on the quality of the various macronutrients, the goals of the dietary treatment regimen and the individual’s values and preferences.”
That is, they recognize that a person’s individual preference for the amount and type of protein (animal-based, plant-based, both), fat (from animal or plant based sources), as well as the amount and type of carbohydrate in their diet factors into their personal decision for how they choose to manage their diabetes.
The Clinical Practice Guidelines for Nutrition Therapy mentions that based on the 3 systematic and meta-analysis of controlled trials of carbohydrate restricted diets that they looked at (mean carbohydrate intake from 4% to 45% of total daily energy) that consistent improvements in HbA1C, lipids and blood pressure weren’t shown.
“As for weight loss, low-carbohydrate diets for people with type 2 diabetes have not shown significant advantages for weight loss over the short term. There also do not appear to be any longer-term advantages.”
So while they do not believe based on the few studies that they examined that there is any advantage to someone following a low carbohydrate diet, there are no clear disadvantages. It comes down to individual preference.
The Guidelines also highlight that there may be a benefit of substituting monounsaturated fat (MUFAs) such as is found in olive oil for carbohydrate (something I regularly do when I design Meal Plans) and that systematic review and meta-analysis of randomized controlled trials found that monounsaturated fat substituted calorie for calorie for carbohydrate did not reduce HbA1C, but did improve fasting blood glucose, body weight, systolic BP, triglycerides and HDL (so-called “good cholesterol”) in people with type 2 diabetes over an average follow up of 19 weeks.
Another finding they reported is that replacement of refined high glycemic index carbohydrates with monounsaturated fat (up to 14.5% total energy) or nuts (up to 5% total energy) has been shown to improve HbA1C and lipids in people with type 2 diabetes over a 3 month period.
Together, these findings provide support to those who prefer to replace high glycemic carbs in their diet (such as white bread, pasta and rice) with monounsaturated fat sources such as olives, avocado as well as some nuts.
The new Clinical Practice Guidelines outline several popular weight-loss diets highlighting that there are a “range of macronutrient profiles are available to people with diabetes”;
“Numerous popular weight-loss diets providing a range of macronutrient profiles are available to people with diabetes. Several of these diets, including the Atkins™, Zone™, Ornish™, Weight Watchers™ and Protein Power Lifeplan™ diets, have been subjected to investigation in longer-term, randomized controlled trials in participants with overweight or obesity that included some people with diabetes, although no available trials have been conducted exclusively in people with diabetes.
They say that a systematic review and meta-analysis of four trials of the Atkins™ diet and 1 trial of the Protein Power Lifeplan™ diet showed that these diets were no more effective than conventional energy-restricted, low-fat diets in inducing weight loss, or with improvements in triglycerides and HDL for up to one year and have been reported to increase total cholesterol and LDL. As mentioned in an earlier article, without differentiating between particle size of LDL (small, dense versus large, fluffy), LDL and total cholesterol going up has not real meaning.
The Guidelines also mentioned that “The Dietary Intervention Randomized Controlled Trial (DIRECT) showed that the Atkins™ diet produced weight loss and improvements in the lipid profile compared with a calorie-restricted, low-fat conventional diet; however, its effects were not different from that of a calorie-restricted Mediterranean-style diet at two years.”
They add that “another trial comparing the Atkins™, Ornish™, Weight Watchers™ and Zone™ diets showed similar weight loss and improvements in the LDL:HDL ratio without effects on fasting blood sugar at one year in participants with overweight or obesity, of whom 28% had diabetes.
So again, it comes down to a matter of choice as to whether someone would prefer to do a calorie-restricted weight loss diet or a well-designed low carb one.
At the end of the paper, the authors make their final recommendations, some of which include that;
“People with diabetes should receive nutrition counselling by a registered dietitian to lower A1C levels and to reduce hospitalization rates”.
“Individuals with diabetes should be encouraged to follow Eating Well with Canada’s Food Guide in order to meet their nutritional needs.”
“In people with overweight or obesity with diabetes, a nutritionally balanced, calorie-reduced diet should be followed to achieve and maintain a lower, healthier body weight”.
“An intensive healthy behaviour intervention program, combining dietary modification and increased physical activity, may be used to achieve weight loss, improve glycemic control and reduce CV risk.”
“In adults with diabetes, the macronutrient distribution as a percentage of total energy can range from 45% to 60% carbohydrate, 15% to 20% protein and 20% to 35% fat to allow for individualization of nutrition therapy based on preferences and treatment goals.”
“People with type 2 diabetes should maintain regularity in timing and spacing of meals to optimize glycemic control.”
“To reduce the risk of cardiovascular disease, adults with diabetes should avoid trans fatty acids and consume less than 9% of total daily energy from saturated fatty acids, replacing these fatty acids with polyunsaturated fatty acids, particularly mixed n-3 / n-6 sources, monounsaturated fatty acids from plant sources, whole grains or low glycemic index carbohydrates”
“Adults with diabetes should select carbohydrate food sources with a low-GI to help optimize glycemic control to improve LDL and to decrease cardiovacular risk.”
“The following dietary patterns may be considered in people with type 2 diabetes, incorporating patient preferences, including:
(a) Mediterranean-style dietary pattern to reduce major cardiovascular events and improve glycemic control.
(b) Vegan or vegetarian dietary pattern to improve glycemic control and reduce myocardial infarction risk.
(c) DASH dietary pattern to improve glycemic control and reduce major cardiovascular events.
(d) Dietary patterns emphasizing dietary pulses (e.g. beans, peas, chickpeas, lentils) to improve glycemic control, systolic BP and body weight.
(e) Dietary patterns emphasizing fruit and vegetables to improve glycemic control and reduce CV mortality.
(f) Dietary patterns emphasizing nuts to improve glycemic control and LDL cholesterol.
Funding sources for the three authors of the Nutrition Therapy guidelines were as follows; Dr. John L. Sievenpiper, MD, PhD; Canadian Institutes of Health Research (CIHR), Calorie Control Council, INC International Nut and Dried Fruit Council Foundation, The Tate and Lyle Nutritional Research Fund at the University of Toronto, The Glycemic Control and Cardiovascular Disease in Type 2 Diabetes Fund at the University of Toronto (a fund established by the Alberta Pulse Growers), PSI Graham Farquharson Knowledge Translation Fellowship, Diabetes Canada Clinician Scientist Award, Banting & Best Diabetes Centre Sun Life Financial New Investigator Award, and CIHR INMD/CNS New Investigator Partnership Prize; grants and non-financial support from American Society for Nutrition (ASN), and Diabetes Canada; personal fees from mdBriefCase, Dairy Farmers of Canada, Canadian Society for Endocrinology and Metabolism (CSEM), GI Foundation, Pulse Canada, and Perkins Coie LLP; personal fees and non-financial support from Alberta Milk, PepsiCo, FoodMinds LLC, Memac Ogilvy & Mather LLC, Sprim Brasil, European Fruit Juice Association, The Ginger Network LLC, International Sweeteners Association, Nestlé Nutrition Institute, Mott’s LLP, Canadian Nutrition Society (CNS), Winston & Strawn LLP, Tate & Lyle, White Wave Foods, and Rippe Lifestyle, outside the submitted work; membership in the International Carbohydrate Quality Consortium (ICQC) and on the Clinical Practice Guidelines Expert Committees of Diabetes Canada, European Association for the study of Diabetes (EASD), Canadian S74 J.L. Sievenpiper et al. / Can J Diabetes 42 (2018) S64—S79 Cardiovascular Society (CCS), and Canadian Obesity Network; appointments as an Executive Board Member of the Diabetes and Nutrition Study Group (DNSG) of the EASD, Director of the Toronto 3D Knowledge Synthesis and Clinical Trials foundation; unpaid scientific advisor for the Food, Nutrition, and Safety Program (FNSP) and the Technical Committee on Carbohydrates of the International Life Science Institute (ILSI) North America; and spousal relationship with an employee of Unilever Canada. Dr. Chan reports grants from Danone Institute, Canadian Foundation for Dietetic Research, Alberta Livestock and Meat Agency, Dairy Farmers of Canada, Alberta Pulse Growers, and Western Canada Grain Growers. Dr. Catherine B Chan has a patent No. 14/833,355 pending to the United States. Dr. Catherine Freeze, MEd, RD reports personal fees from Dietitians of Canada and Government of Prince Edward Island.
Some Final Thoughts…
Much of the same wording regarding supporting individual preference was previously embodied in the 2013 Clinical Practice Guidelines of the Canadian Diabetes Association. While not “recommended”, there was previously the same option for individuals to choose to follow a low carb lifestyle, based on personal preference.
As a Dietitian, I keep reading and reviewing the literature in order to provide the most current, evidence-based low carbohydrate diet to support those that choose to follow a low carb lifestyle — or who’s doctors recommend that they do, and in this way allow for the individualization of nutrition therapy in an evidence-based framework.
Do you have questions as to how I can help support your preference to follow a low carb lifestyle? Please send me a note using the “Contact Me” form on this web page and I’ll reply as soon as possible.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This article is Part 2 in a two-part series on concerns with Polyunsaturated Vegetable Oils.Part 1 can be read here.
There are a few key things about polyunsaturates vegetable oils that need to be understood to understand this article, so I’ll keep the science simple.
There are two class of polyunsaturated fats; (PUFAs); omega 3 (ρ‰-3 also written n-3) and omega 6 (ρ‰-6 / n-6) which compete with each other for enzymes, and which becomes significant at one branch point (marked with the red and green box).
At that junction point (where the red box is at Arachidonic acid and green box is at Eicosapentanoic acid) if there is more n-6 fats than n-3 fats, then the pathway will favour the n-6 pathway. If there are more n-3 fats than n-6 fats, then the pathway will favour the n-3 pathway. The issue, as I will elaborate on below, is that in the Western diet, the n-6 pathway is always favoured.
Of significance, the n-6 polyunsaturated fats are pro-inflammatory and the n-3 polyunsaturated fats are anti-inflammatory. This is important to understand why eating lots of foods high in n-6 fats can lead to health consequences.
When people take low-dose Aspirin® for example, to lower the risk of heart attack or stroke, it acts on Arachidonic acid in the n-6 polyunsaturated fat pathway, to keep it from making certain inflammatory products that can lead to heart attack or stroke.
In our evolutionary history it was thought that n-6 fats (from nuts and seeds that were gathered in the wild) and n-3 fats (from the fish and meat we hunted) were eaten in close to a 1:1 ratio – providing the two essential fatty acids from both classes. When man began domesticating grain and growing beans and lentils and nuts and seeds for food (all high in n-6 fats), the shift towards a diet higher in n-6 fats occurred. The modern Western diet is estimated to have an omega-6 to omega-3 fatty acids of 15—20:1 in favour of n-6 fats [6].
Many people take omega-3 fish oil capsules in an effort to protect their body from inflammation, but because the amount of n-6 fats in the diet is so much higher than the amount of n-3 fats, the n-6 pathway is still favoured.
Unless we significantly lower the amount of n-6 fats in the diet, taking fish oil doesn’t really help as the n-6 pathway will always be favoured.
Changing the Makeup of Cell Components
Industrial seed oils have very high levels of linoleic acid which is at the top of the n-6 pathway. These industrial seed oils are pro-inflammatory and will elongate to Arachidonic acid, resulting in many pro-inflammatory products being produced.
When we eat a lot of food made with soybean oil or fried in soybean oil we eat way more linoleic acid then our body has evolved to handle.
A major problem with polyunsaturated fatty acids such as linoleic acid are that they are very unstable fats that are easily oxidized (similar to a fat becoming ‘rancid’ or a metal ‘rusting’). Even if we never buy these industrial seed oils to cook with at home, when we buy French fries at restaurants they are fried in either soybean or canola oil. When we pick up a donuts, same thing. Bottle salad dressing and mayonnaise (even the one that is called ‘olive oil mayonnaise’) are made with one of these industrial seed oils. These oils are found in products one would never expect to find them, including peanut butter! Start reading labels and you will be shocked how many products they are in – or rather, how few products they are NOT in.
Industrial seed oils are in most of the prepared food we buy and almost all of the food we eat out in fast-food restaurants.
According to a 2011 journal article published in the American Journal of Clinical Nutrition;
“The most striking modification of the US food supply during the 20th century was the >1000-fold increase in the estimated per capita consumption of soybean oil from 0.006% to 7.38% of energy.” [7]
When the linoleic acid content of the diet is high because we are eating foods made with industrial seed oils, important components of our cells membranes incorporate higher amount of linoleic acid into them.
For example, cardiolipin is a phospholipid component found in the inner mitochondrial membrane, which is where all energy metabolism in our body occurs. Cardiolipin plays an important role in the function of several enzymes involved in mitochondrial energy metabolism.
When we eat a lot of pre-made and processed foods and food made in fast-food restaurants, cardiolipin ‘s fatty acid content becomes 90% linoleic acid, making it easily oxidized, affecting its function. If the diet is high in coconut oil and olive oil, cardiolipin will be higher in stearic and oleic acids and these fats are more stable fats than linoleic acid.
Literally, we are what we eat!
Cooking with Industrial Seed Oils
When industrial seed oils are heated such as they are in the making of commercial foods using them, they undergo rapid oxidation which means that they react with oxygen in the air to form toxic substances, including aldehydes and lipid peroxides. Aldehydes are known neurotoxins and carcinogens, and are documented to contribute to DNA mutations, inflammation and hypersensitivity [8].
Heating polyunsaturated vegetable oils for just 20 minutes produces 20 times the permitted levels of aldehydes recommended as a maximum limit by the World Health Organization [8].
Keep in mind that at fast-food restaurants and in the preparation of commercial donuts and other fried food products, these industrial seed oils are used for frying everything from French fries to donuts and are heated over and over for extended periods of time, creating alarming levels of aldehydes and lipid peroxidation products.
When heated, industrial seed oils produce oxidized metabolites known as oxidized linoleic acid metabolites (OXLAMs) which have been also been implicated in the development of non-alcoholic fatty liver disease (NAFLD)[9].
In the body cell components such as cardioleptin with high amounts of linoleic acid are easily oxidized producing an oxidation product known as 4-hydroxynonenal (4-HNE) which has been implicated in the development of cancer [10].
Increasing Appetite
The high linoleic acid content of industrial seed oils also act on two endo-cannibinoids in the body (2-AG and Anandamide) which results in us feeling hungry, even when we have recently eaten – in much the same way as cannabis (marijuana) does [11-12]. As a result, these industrial seed oils are believed to contribute to obesity and the associated health risks such as Type 2 Diabetes and high blood pressure.
Final Thoughts…
For fifty years, the public ate industrially-created trans fats in place of natural saturated fats and we only found out later that they were a major contributor to heart disease.
For the last forty years we have been eating industrial seed oils in greater and greater quantities place of natural saturated fat, but (a) given how these industrial seed oils are produced (solvents, high heats for extended period of time, bleach, etc.) and (b) given what is known about the very toxic products they produce when heated in production and how they are oxidized in the body and oxidized through heating when cooking, it is warranted to be very cautious about eating prepared foods made with them.
To avoid these industrial seed oils will take a concerted effort as they are in virtually everything we buy ready-made and many of the foods we eat out, but one solution is to cook real food using healthy sources of fat and to avoid these industrial seed oils that were created and marketed to us as supposedly healthy substitutes for natural fats.
The butter, lard and tallow of years gone by were made from animals that were pasture raised, not fed soybeans and corn as commercial animals are now, but in light of the mounting number of studies that indicate that saturated fat is not associated with increased risk of cardiovascular disease, perhaps it might be preferable to buy grass fed butter or render tallow or lard from the fat of pasture-raised animals for some cooking applications – rather than use these industrial seed oils that were created as substitutes. Butter, lard and coconut oil (a vegetarian saturated fat) are all very low in linoleic acid and thus are very stable. They are not easily oxidized in the body or by heating and produce very low levels of aldehyde and lipid peroxidation products when heated, compared with many of the industrial seed oils.
These are all factors we need to consider when deciding which fats our food should be made with.
The chart below shows the linoleic content of some common fats in blue. Keep in mind that fats with the smallest amount of linoleic acid are the most stable and the least prone to oxidation (either in the body or when heated).
Comparison of Dietary Fats – linoleic acid content
A personal note: For non-heating uses, I use natural sources of monounsaturated fat such as cold pressed macadamia nut oil, hazelnut oil, avocado oil, and extra virgin olive oil and for cooking and heating uses I use a mixture of olive oil and coconut oil (to raise the smoke point), clarified butter (ghee) at higher temperatures and butter at lower temperatures and for baking. I read labels of all products I buy and deliberately avoid purchasing any food products that contain soybean oil, canola oil or sunflower oil and when I eat out, I ask that my food be prepared with coconut oil, butter or ghee.
While the jury is still “out” when in comes to saturated fat, it is my opinion that with the mounting evidence that eating saturated fat does not contribute to heart disease, using moderate use of butter, ghee (clarified butter) and coconut oil seems to me to be a more acceptable risk than eating foods made with, or fried in industrial seed oils.
I trust having the information contained in this article will help you make an informed choice for yourself and for those you cook for.
If you have questions about how I might be able to help you follow a low carb lifestyle -including selecting appropriate fats for use in your own cooking, please feel free to send me a note using the “Contact Me” form located on the tab above.
6. A.P. Simopoulos, Evolutionary aspects of the dietary omega-6:omega-3 fatty acid ratio: medical implications,World Rev Nutr Diet, 100 (2009), pp. 1-21
7. Tanya L Blasbalg, Joseph R Hibbeln, Christopher E Ramsden, Sharon F Majchrzak, Robert R Rawlings; Changes in consumption of omega-3 and omega-6 fatty acids in the United States during the 20th century, The American Journal of Clinical Nutrition, Volume 93, Issue 5, 1 May 2011, Pages 950—962.
8. Grootvelt M, Rodada VR, Silwood CJL, Detection, monitoring, and
deleterious health effects of lipid oxidation products generated in culinary oils during thermal stressing episodes, Lipid Oxidation, November/December 2014, Vol. 25 (10)
9. Maciejewska, Dominika & Ossowski, Piotr & Drozd, Arleta & Karina, Ryterska & Dominika, Jamioł & Banaszczak, Marcin & Małgorzata, Kaczorowska & Sabinicz, Anna & Wyszomirska, Joanna & Stachowska, Ewa. (2015). Metabolites of arachidonic acid and linoleic acid in early stages of non-alcoholic fatty liver disease-A pilot study. Prostaglandins & other lipid mediators.
10. Zhong H, Yin H. Role of lipid peroxidation derived 4-hydroxynonenal (4-HNE) in cancer: Focusing on mitochondria. Redox Biology. 2015;4:193-199. doi:10.1016/j.redox.2014.12.011.
11. Alvheim AR, Malde MK, Hyiaman DO et al; Dietary Linoleic Acid Elevates Endogenous 2-AG and Anandamide and Induces Obesity, Obesity (2012) 20;1984-1994
12. Alveim AR, Torstensen BE, Lin YH et al, Dietary Linoleic Acid Elevates the Endocannabinoids 2-AG and Anandamide and Promotes Weight Gain in Mice Fed a Low Fat Diet, Lipids (2014) 49:59—69
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
INTRODUCTION: Both the US and Canadian Dietary Guidelines encourage us to limit saturated fat in order to reduce the risk of heart disease and to eat unsaturated fat, including polyunsaturated fats and oils instead but what are these fats, where do they come from and what role might these play in development of obesity, Type 2 Diabetes, non-alcoholic fatty liver disease and even cancer? This article is part 3 in the series titled Bad Fats and Enduring Beliefs.
Part 1 titled the Vilification of Saturated Fat can be read here and Part 2 titled Saturated Fat and Heart Disease can be read here.
“Polyunsaturated vegetable oils” is really a misnomer, as neither soybeans nor rapeseed / Canola are “vegetables”. More accurately these should be called “industrial seed oils”, as they are seed crops that have been deliberately engineered for food use. These are created oil products which are quite unlike natural oils that can be easily expressed from nuts, seeds and fruit using a millstone, as has been done since the Bronze Age [1].
Ancient olive oil press
If you simply press olives, almonds, sesame or poppy seeds between your fingers you will be able to express a little bit of their oil on your fingers.
Not so with soybeans!
You can squeeze a soybean as hard as you like and for as long as you like and you are not going to get any oil out of it!
The first attempt at trying to express oil from soybeans occurred in the United States, a few years after the creation of Crisco® shortening in 1911. For 3 long years (1922 – 1925) scientists tried over and over again to extract oil from soybeans imported from Manchuria using hydraulic presses, and time and time again they failed. Finally, in 1925 scientists turned to the use of chemical solvents to get oil from soybeans and solvent extraction of soybean oil has been used ever since.
Trans Fats and Industrially Produced Shortening
In days gone by, deep-fat frying in restaurants (e.g. for French fries) was done in beef tallow, sometimes in lard. Pastry crusts were made with lard or butter, and baked goods such as cakes and brioches were usually made with butter – that is until 1911 when Crisco® shortening was invented. When it was noticed that hardened cottonseed oil used in the soap-making industry had an appearance like lard, scientists decided to further process it to remove the strong odor inherent with cottonseed oil, and market it to housewives as the ‘modern’ way to bake. You can read more about that here.
Beginning in the 1950s, trans fats (which occurs naturally in very small quantities) were industrially produced from other industrial seed oils such as soybean oil for use in other natural fat substitutes, including margarine, fat for commercial baked goods and fat for deep-fat frying in the fast food industry [2]. Unfortunately, it was only in the late 1990s and early 2000s that it became widely-accepted by the scientific community that eating foods made with trans fats or fried in trans fats raised LDL-cholesterol while lowering protective HDL cholesterol, and also raised triglycerides; promoting systemic inflammation and contributing to the development of heart disease.
How ironic that the fats that were created to replace naturally-occurring saturated fats ended up being so detrimental to health!
After trans fats were discontinued due to their adverse health effects, industrial seed oils such as soybean oil and canola oil became the number one and number two oils of the food industry. These unsaturated (liquid) industrial seed oils have replaced saturated (solid) trans fat industrial oils in our food supply, however there is considerable evidence emerging which should cause us to question whether these fats are any safer (more on that below).
The Created Market for Industrial Seed Oils
The market for industrial trans fats and liquid industrial seed oils was itself created based a belief that ‘dietary saturated fat led to heart disease’. Much of what we have come to believe about this originated with a pathologist named Ancel Keys who proposed his ‘diet-heart hypothesis’ in the 1950s.
In 1970, Keys published his “Seven Country Study” that reported that populations that consumed large amounts of saturated fats in meat and dairy had high levels of heart disease but when data from 22 countries that was available since 1957 was plotted, it was a great deal more scattered, indicating a much weaker association than Keys’ Seven Country Study data indicated.
In August of 1967, Stare, Hegsted and McGandy, 3 Harvard researchers paid by the sugar industry published their reviews inthe New England Journal of Medicine which vindicated sugar as a contributor of heart disease and laid the blame on dietary fat and in particular, saturated fat and dietary cholesterol (previous article on that topic here). Sponsorship of this research by the sugar industry certainly casts a dark shadow over their findings.
These 3 researchers insisted in their conclusion that there was a link between dietary cholesterol and heart disease and that there was “major evidence” which suggested that there was “only one avenue for diet to contribute to hardening of the arteries and the development of heart disease”, but as covered in the previous article, it is known that a year after their publications (1968), the report of the Diet-Heart Review Panelof the National Heart Institute made the recommendation that a major study be conducted to determine whether changes in dietary fat intake prevented heart disease because such a study had not yet been done.
Just 10 years after the sugar industry paid Stare, Hegsted and McGandy to write their reviews, Hegsted was directly involved with developing and editing the 1977 US Dietary Guidelines which recommended that Americans decrease intake of saturated fat and cholesterol and increase dietary carbohydrate – entrenching the belief that saturated fat caused heart disease into American public health policy. That same year (1977), based on the same body of literature, Canada adopted very similar dietary guidelines around saturated fat…and the rest is history.
Public Health Policy Based Rooted in a Belief
For the last forty years Americans and Canadians have shunned natural fats such as butter, cream and lard in place of man-made margarine, non-dairy creamer and Crisco® – all in the enduring belief that ‘saturated fat is “bad” and leads to heart disease’. Given that published reports vilifying saturated fat were funded by the sugar industry and that Ancel Keys study left out 2/3 of the nutrition and health data available at the time, it has become evident that public health policy was founded on what is now questionable data.
In addition, more and more current peer-reviewed published studies are concluding that saturated fat is not associated with an increased risk of developing cardiovascular disease. In the recent article titled Saturated Fat and Heart Disease, I outlined the findings of 8 recent meta-studies and systematic reviews and one worldwide epidemiological study which call into question the enduring belief that dietary saturated fat increases the risk of developing heart disease.
In a follow up to the above article, titled More Animal Fat Consumption Less Cardiovascular Disease, I also summarize the findings of a newly published worldwide study which found that total fat and animal fat consumption were least associated with the risk of cardiovascular disease.
If saturated fat is not associated with increased risk of heart disease then should we be eating industrial seed oils that were created and marketed as a replacement for them?
Creation of Industrial Seed Oils
Inexpensive soybean oil has been the leading oil used in food production in the United States since 1945 [3]. It was previously made into a hard fat through hydrogenation and sold to consumers as trans-fat based shortening and margarine and came into wide-spread use as both synthetic hard fat and as a food-based oil product in the late-1960s.
In Canada, soybean oil is just behind canola oil in terms of the most used, and canola is another industrial seed oil that was created by science. In 1978 rapeseed, a prairie weed was specially bred in Canada to produce a novel plant that was lower in erucic acid (a toxin found in rapeseed) and this new plant was named “canola” (‘Canadian Oil’).
A 2015 study on Canadian vegetable oil purchased and eaten in Canada found that in 2013, 42% was canola oil (a Canadian bio-engineered industrial seed oil) and 20% was soybean oil, an industrially-engineered seed oil developed in the US [4]. Keep in mind this figure excludes food products available in Canada that are manufactured in the US, which uses predominantly soybean oil.
Soybean Oil is a Modern, Industrial Product
According to an article titled “Soybeans Are Ancient; Oil Is Not” published in the Wall Street Journal in 2011 [5], soybeans as the basis for tofu and soy sauce is an ancient food in China, but soybean oil was virtually unknown until global food oil shortages during World War I created an interest to extract the fatty part of the soybean for oil. Soybean oil is a modern creation.
How is oil made from seeds such as soybean and canola?
“Soybeans are first crushed into crude oil and then refined to remove impurities like free fatty acids. Over days, the crude is ”neutralized” of acidity with phosphoric acid, ”winterized” through filters that remove wax, bleached at high heat to lighten the color and finally vacuum ”deodorized” to eliminate impurities.” [5]
The extraction of soybean oil involves the industrial processing of soybeans with solvents at very high heats over an extended length of time in order to have the soybean give up its small amount of oil.
Solvent extraction of canola oil occurs in a similar method, beginning with an hour or more ‘wash’ of the rapeseed with a hexane solvent, then a sodium hydroxide wash. Bleach is then used to lighten the cloudy color of the processed oil and then it is steamed injected at high temperatures to
remove the bitter smell.
Yummy! Now this oil is ready to sell to the public to cook with and eat!
Should we even be eating these industrial seed oils?
Are they any safer than trans fats that were approved for consumption for 50 years and later found to contribute to heart disease?
Part 2 of this article will continue in Concerns with Polyunsaturated Vegetable Oils – Part 2.
If you have questions about how I might be able to help you follow a low carb lifestyle -including selecting appropriate fats for use in your own cooking, please feel free to send me a note using the “Contact Me” form located on the tab above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Special thanks to Tucker Goodrich for getting me thinking in this regard.
INTRODUCTION: A brand new study published last week in Nutrients looked at health and nutrition data from 158 countries worldwide and found that total fat and animal fat consumption were least associated with the risk of cardiovascular disease. As well, the study found that high carbohydrate consumption, particularly as cereals and wheat was most associated with the risk of cardiovascular disease. Significantly, both of these relationships held up regardless of a nation’s average national income.
Data from this study adds to the mounting evidence from 8 recent meta-analyses and systemic reviews of randomized control trials (RCT) summarized in this article that did not find an association between saturated fat intake and the risk of heart disease[1-8]. It also supports evidence from the recent global PURE (Prospective Urban and Rural Epidemiological) study published in The Lancet this past December which found that those who ate the largest amounts of saturated fats had significantly reduced death rates, and that those that ate the lowest amounts of saturated fat (6-7% of calories) had increased risk of stroke [9].
Global Correlates of Cardiovascular Risk: a comparison of 158 Countries
This new study compared the average intake of 60 food items with obesity rates and life expectancy in 158 countries and found that a relationship existed between eating specific foods and raised blood pressure, death from cardiovascular disease and raised blood glucose (high blood sugar) — all of which are associated with cardiovascular disease. The study examined nutritional data from 1993-2011 and found that total fat consumption and animal fat consumption were the dietary factors least associated with the risk of cardiovascular disease and that high carbohydrate consumption, especially as cereals and wheat was the dietary factor most associated with the risk of cardiovascular disease [10].
These findings add to the mounting evidence which calls into question whether dietary saturated fat is related to heart disease.
Total Cholesterol and Cardiovascular Risk
The present study found that eating animal fat and animal protein raised total cholesterol, however total fat and animal protein consumption were found to have a very impressive negative relationship with cardiovascular death in the European data, and a moderately negative relationship to cardiovascular death, worldwide. That is, the more total fat and animal protein eaten, the lower cardiovascular death rates were.
Often in studies, the assumption is that high LDL is linked to risk of cardiovascular disease – not that there is a direct relationship between animal / saturated fat and cardiovascular disease. That is, high LDL is a surrogate marker of cardiovascular disease. But does that assumption hold weight?
Perhaps a better question is “which LDL”? Small, dense LDL cholesterol which easily penetrates the artery wall is associated with heart disease [11,12,13,14], but the large, fluffy LDL cholesterol is not [15,16], so studies seeking to impute LDL as the cause of cardiovascular diseasee need to differentiate between these LDL particles.
As well, total cholesterol is made up of the different sub-particles of LDL cholesterol, HDL cholesterol, VLDL cholesterol and triglycerides (TG), so lumping them all in together as ‘total cholesterol’ doesn’t tell us anything about risk of cardiovascular disease. We know that dietary saturated fat consistently raises the ”good” HDL-cholesterol — which moves cholesterol away from the arteries and back to the liver where it can either be re-used or eliminated [17,18], so higher saturated fat intake will raise “good” HDL cholesterol, which in turn will raise total cholesterol. Total cholesterol going up is not a ‘bad’ thing.
What is important is not that total cholesterol went up but that along with increased total cholesterol, cardiovascular disease went down.
Higher Blood Sugar Associated with Higher Consumption of Cereals and Wheat
One finding of this study was that higher blood sugar (a known risk factor for cardiovascular disease) was most strongly associated with indicators of obesity such as high body mass index (BMI). What was new however is that higher consumption of cereals, especially cereals and wheat was associated with higher cardiovascular disease.
Researchers remarked that such results were not surprising “because the links between raised blood glucose, obesity, type 2 diabetes and cardiovascular disease are well established [19]”.
“…regardless of the statistical method used, the results always show very similar trends and identify high carbohydrate consumption (mainly in the form of cereals and wheat, in particular) as the dietary factor most consistently associated with the risk of CVDs.
High carbohydrate consumption, particularly as cereals and wheat was the dietary factor most consistently associated with the risk of cardiovascular disease.
Researchers looked at a maximum number of potentially significant variables and compared them to results across different regions and time periods and while they acknowledged that the accuracy of the data from developing countries may be lower, the global results that they found confirmed their earlier 2016 study data from European data only which found a significant link between cardiovascular disease and high carbohydrate consumption [20].
Of significance, the above associations held up regardless of a nation’s average national income.
Given these finding support those of the PURE epidemiological study [9] would lend support the notion that one can compare data between countries of substantially different level of income (as the PURE study did) and that high-carbohydrate and low-fat diets are not necessarily associated with poverty, as claimed [21].
The PURE study findings and those of this present study challenge the very basis of the long-standing ‘diet-heart hypothesis’ and it certainly results in some uncertainty as to what constitutes a healthy diet.
In my view, what is needed are some well-designed randomized controlled trials to determine if saturated fat intake is directly associated with cardiovascular disease – and not associated with a surrogate marker, such as LDL cholesterol.
Purported Weakness of the Data
Self-reported food-frequency questionnaires on which this study is based have long been criticized as being unreliable, however it is important to note that in the United States the NHANES Dietary Data and the Continuing Survey of Food Intakes by Individuals (USA) has also collected data using food-frequency questionnaires and such data is used as the “cornerstone to inform nutrition and health policy” [22].
In Canada, the Canadian Community Health Survey (CCHS) relies on a 24-hour recall data which is known to researchers to result in under-reporting of food intake, especially among those with a high BMI and with adolescents [23]. Given that the 2017 Obesity Update found Canada among its most overweight countries — with 25.8% of the population aged 15 and over considered obese [24], the CCHS data becomes less and less reliable, as obesity rates continue to climb.
Enduring Belief – despite recent evidence
The results of this most recently published study embody the same findings as the recent global PURE (Prospective Urban and Rural Epidemiological) study [9] publish this past December in The Lancet which found a link between raised cholesterol and lower cardiovascular risk.
This study also confirms the findings of the eight recent meta-analysis and systemic reviews of randomized control trials (RCT) summarized in the previous article which did not find an association between saturated fat intake and the risk of heart disease [1-8].
Yet, in spite of recent robust evidence there is an enduring belief that ‘saturated fat causes heart disease’ — a belief which has influenced nutrition guidelines in both the US and Canada for 40 years (since 1977).
As elaborated on in a recent article, it is now known that the ‘diet-heart hypothesis’ originated by Ancel Keys and supposedly confirmed in his ‘Seven Countries Study’ omitted known data from 22 available countries and that when all countries were factored in there was a great deal more scatter showing a much weaker relationship between dietary fat and death by coronary heart disease than was suggested by Keys’s data.
Also as covered previously, it has been known since December 2016 that the three Harvard researchers who vindicated sugar as the cause of heart disease and blamed dietary fat — were funded by the sugar industry and that one one of those 3 researchers, Dr. DM Hegsted contributed to and edited the 1977 US Dietary Guidelines which embodied his findings of 10 years earlier, advising Americans to reduce their intake of saturated fat and cholesterol in order to reduce their risk of heart disease.
Also covered in a previous article, Canadian Dietary Recommendations regarding dietary intake of saturated fat were based on ‘health claim assessments’ conducted by Health Canada in 2000 (18 years ago) titled Dietary Fat, Saturated Fat, Cholesterol, Trans Fats and Coronary Heart Disease which was based on the US literature available from 1993-2000 and which concluded that a health risk exists between saturated fat and heart disease.
Given all of the factors mentioned above, it is my conviction that before the American and Canadian governments revise their respective national Dietary Guidelines what is needed is for them to conduct a long-overdue external, independent scientific review of the current evidence for the enduring belief that saturated fat contributes to heart disease.
If you have questions as to how I can help you live a low carb lifestyle, please send me a note using the “Contact Me” form located on the tab above.
Skeaff CM, PhD, Professor, Dept. of Human Nutrition, the University of Otago, Miller J. Dietary Fat and Coronary Heart Disease: Summary of Evidence From Prospective Cohort and Randomised Controlled Trials, Annals of Nutrition and Metabolism, 2009;55(1-3):173-201
Hooper L, Summerbell CD, Thompson R, Reduced or modified dietary fat for preventing cardiovascular disease, 2012 Cochrane Database Syst Rev. 2012 May 16;(5)
Chowdhury R, Warnakula S, Kunutsor S et al, Association of Dietary, Circulating, and Supplement Fatty Acids with Coronary Risk: A Systematic Review and Meta-analysis, Ann Intern Med. 2014 Mar 18;160(6):398-406
Schwingshackl L, Hoffmann G Dietary fatty acids in the secondary prevention of coronary heart disease: a systematic review, meta-analysis and meta-regression BMJ Open 2014;4
Hooper L, Martin N, Abdelhamid A et al, Reduction in saturated fat intake for cardiovascular disease, Cochrane Database Syst Rev. 2015 Jun 10;(6)
Harcombe Z, Baker JS, Davies B, Evidence from prospective cohort studies does not support current dietary fat guidelines: a systematic review and meta-analysis, Br J Sports Med. 2017 Dec;51(24):1743-1749
Ramsden CE, Zamora D, Majchrzak-Hong S, et al, Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-73), BMJ 2016; 353
Hamley S, The effect of replacing saturated fat with mostly n-6 polyunsaturated fat on coronary heart disease: a meta-analysis of randomised controlled trials, Nutrition Journal 2017 16:30
Dehghan M, Mente A, Zhang X et al, The PURE Study – Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. Lancet. 2017 Nov 4;390(10107):2050-2062
Grasgruber P, Cacek J, Hrazdira E, et al, Global Correlates of Cardiovascular Risk: A Comparison of 158 Countries, Nutrients2018, 10(4), 411.
Tribble DL, Holl LG, Wood PD, et al. Variations in oxidative susceptibility among six low density lipoprotein subfractions of differing density and particle size. Atherosclerosis 1992;93:189—99
Gardner CD, Fortmann SP, Krauss RM, Association of Small Low-Density Lipoprotein Particles With the Incidence of Coronary Artery Disease in Men and Women, JAMA. 1996;276(11):875-881
Lamarche B, Tchernof A, Moorjani S, et al, Small, Dense Low-Density Lipoprotein Particles as a Predictor of the Risk of Ischemic Heart Disease in Men, Circulation. 1997;95:69-75
Packard C, Caslake M, Shepherd J. The role of small, dense low density lipoprotein (LDL): a new look, Int J of Cardiology, Volume 74, Supplement 1, 30 June 2000, Pages S17-S22
Genest JJ, Blijlevens E, McNamara JR, Low density lipoprotein particle size and coronary artery disease, Arteriosclerosis, Thrombosis, and Vascular Biology. 1992;12:187-195
Siri-Tarino PW, Sun Q, Hu FB, Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease, The American Journal of Clinical Nutrition, Volume 91, Issue 3, 1 March 2010, Pages 502—509
Mensink RP, Zock PL, Kester A, Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials, The American Journal of Clinical Nutrition, Volume 77, Issue 5, 1 May 2003, Pages 1146—1155
Toth PP, The “Good Cholesterol” – High Density Lipoprotein, Circulation 2005;111:e89-e91
Després, J.P.; Lemieux, I.; Alméras, N. Abdominal obesity and the metabolic syndrome. In Overweight and the Metabolic Syndrome; Springer: New York, NY, USA, 2006; pp. 137—152
Grasgruber, P.; Sebera, M.; Hrazdira, E.; Hrebickova, S.; Cacek, J. Food consumption and the actual statistics of cardiovascular diseases: An epidemiological comparison of 42 European countries. Food Nutr. Res.2016, 60, 31694.
Sigurdsson, AF, The Fate of the PURE Study — Fat and Carbohydrate Intake Revisited, Doc’s Opinion, October 16 2017, www.docsopinion.com/2017/10/16/pure-study-fats-carbohydrates/
Ahluwalia N, Dwyer J, Terry A, et al; Update on NHANES Dietary Data: Focus on Collection, Release, Analytical Considerations and Uses to Inform Public Policy, Advances in Nutrition, Volume 7, Issue 1, 1 January 2016, Pages 121—134
Health Canada, Reference Guide to Understanding and Using the Data – 2015 Canadian Community Health Survey – Nutrition, June 2017
OECD Health Statistics 2017, June 2017, http://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This is Part 2 in the series which examines the enduring belief that dietary saturated fat causes heart disease.
INTRODUCTION: The ”diet-heart hypothesis” is the belief that saturated fat and dietary cholesterolcause heart disease was first proposed by Ancel Keys in the 1950s. He encouraged Americans to reduce their fat intake by a third, while at the same time openly admitted as late as 1967 that there was little direct evidence that a change in diet would reduce the risks of arteriosclerosis [1]. As covered in the first part of this article, three Harvard researchers, Stare, Hegsted and McGrady were paid generously by the sugar industry to publish their review inthe New England Journal of Medicine vindicating sugar as a cause of heart disease and laying the blame squarely on dietary fat; and in particular on saturated fat. These researchers concluded that there was “only one avenue” by which diet contributed to the development and progression of “hardening of the arteries” (atherosclerosis), resulting heart disease and that was due to how much dietary cholesterol people ate and its effect on blood lipids [2]. This sounds like a very certain claim, however it is known that they lacked evidence because a year later (1968) a report from the Diet-Heart Review Panel of the National Heart Institute made the recommendation that a major study be conducted to determine whether changes in dietary fat intake prevented heart disease – because such a study had not yet been done (see Part 1) [3].
Fast forward ten years and in 1977, one of the three researchers who was paid by the sugar industry, Dr. DM Hegsted contributed to and edited the 1977 US Dietary Guidelines [4], which embodied his findings 10 years earlier. Americans were told they should reduce their intake of saturated fat and cholesterol to reduce their risk of heart disease.
The rest, they say, is history.
The same year (1977), Canada’s Food Guide recommended that Canadians limit fat to <30% of daily calorieswithno more than 1/3 from saturated fat, but did not specify an upper limit for dietary cholesterol. This was based on the belief that total dietary fat and saturated fat were responsible blood levels of LDL cholesterol levels and total serum cholesterol, not dietary cholesterol [5].
Recommendations for the continued restriction of dietary fat continued in both the US and Canada in 2015 are based on the enduring belief that lowering saturated fat in the diet will lower blood cholesterol levels and reduce heart disease.
The question is does it?
NOTE TO CANADIANS: Canadian Dietary Recommendations regarding dietary intake of saturated fat are based on ‘health claim assessments’ conducted by Health Canada which are directly tied to American research and recommendations. Eighteen years ago, Health Canada reviewed the ‘health claim’ regarding Dietary Fat, Saturated Fat, Cholesterol, Trans Fats and Coronary Heart Disease and based on the US literature available from 1993-2000 and concluded that a health risk exists between saturated fat and heart disease, as stated here; “The effectiveness of lowering dietary saturated fat in reducing plasma cholesterol, especially low-density lipoprotein (LDL)- cholesterol, the major risk factor for CHD, is well established.” Since Health Canada’s review in 2000 (18 years ago), the link between dietary saturated fat and heart disease remains public health policy.
While it has been shown that saturated fats can raise LDL-cholesterol such a finding is meaningless unless it is specifiedwhich typeof LDL-cholesterol goes up. There is more than one type of LDL-cholesterol, small, dense LDL cholesterol which easily penetrates the artery wall is associated with heart disease [6,7,8,9], whereas the large, fluffy LDL cholesterol is not [10, 11].
Another factor that needs to be considered is that dietary saturated fat also consistently raises the ”good” HDL-cholesterol which moves cholesterol away from the arteries and back to the liver, where it can either be re-used or eliminated [12,13].
What are the findings of current scientific literature?
Eight recent meta-analysis and systemic reviews which reviewed evidence from randomized control trials (RCT) that had been conducted between 2009-2017 did not find an association between saturated fat intake and the risk of heart disease [14-21].
Furthermore, recently published results of the largest and most global epidemiological study published in December 2017 in The Lancet [23] found that those who ate the largest amount of saturated fats had significantly reduced rates of mortality and that low consumption (6-7% of calories) of saturated fat was associated withincreased risk of stroke.
Here is a synopsis of the findings of the eight meta-analysis and systemic reviews;
”Intake of saturated fatty acids was not significantly associated with coronary heart disease mortality” and “saturated fatty acid intake was not significantly associated coronary heart disease events”
Skeaff CM, PhD, Professor, Dept. of Human Nutrition, the University of Otago, Miller J. Dietary Fat and Coronary Heart Disease: Summary of Evidence From Prospective Cohort and Randomised Controlled
“There were no clear effects of dietary fat changes on total mortality or cardiovascular mortality”.
Hooper L, Summerbell CD, Thompson R, Reduced or modified dietary fat for preventing cardiovascular disease, 2012 Cochrane Database Syst Rev. 2012 May 16;(5)
“Current evidence does not clearly support cardiovascular guidelines that encourage high consumption of polyunsaturated fatty acids and low consumption of total saturated fats.”
Chowdhury R, Warnakula S, Kunutsor S et al, Association of Dietary, Circulating, and Supplement Fatty Acids with Coronary Risk: A Systematic Review and Meta-analysis, Ann Intern Med. 2014 Mar 18;160(6):398-406
“The present systematic review provides no moderate quality evidence for the beneficial effects of reduced/modified fat diets in the secondary prevention of coronary heart disease. Recommending higher intakes of polyunsaturated fatty acids in replacement of saturated fatty acids was not associated with risk reduction.”
Schwingshackl L, Hoffmann G Dietary fatty acids in the secondary prevention of coronary heart disease: a systematic review, meta-analysis and meta-regression BMJ Open 2014;4
“The study found no statistically significant effects of reducing saturated fat on the following outcomes: all-cause mortality, cardiovascular mortality, fatal MIs (myocardial infarctions), non-fatal MIs, stroke, coronary heart disease mortality, coronary heart disease events.”
Note: The one significant finding was an effect for saturated fats on cardiovascular events however this finding lost significance when subjected to a sensitivity analysis (Table 8, page 137).
Hooper L, Martin N, Abdelhamid A et al, Reduction in saturated fat intake for cardiovascular disease, Cochrane Database Syst Rev. 2015 Jun 10;(6)
“Epidemiological evidence to date found no significant difference in CHD mortality and total fat or saturated fat intake and thus does not support the present dietary fat guidelines. The evidence per se lacks generalizability for population-wide guidelines.”
Harcombe Z, Baker JS, Davies B, Evidence from prospective cohort studies does not support current dietary fat guidelines: a systematic review and meta-analysis, Br J Sports Med. 2017 Dec;51(24):1743-1749
“Available evidence from randomized controlled trials (1968-1973) provides no indication of benefit on coronary heart disease or all-cause mortality from replacing saturated fat with linoleic acid rich vegetable oils (such as corn oil, sunflower oil, safflower oil, cottonseed oil, or soybean oil).”
Ramsden CE, Zamora D, Majchrzak-Hong S, et al, Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-73), BMJ 2016; 353
“Available evidence from adequately controlled randomised controlled trials suggest replacing saturated fatty acids with mostly n-6 PUFA is unlikely to reduce coronary heart disease events, coronary heart disease mortality or total mortality. These findings have implications for current dietary recommendations.”
Hamley S, The effect of replacing saturated fat with mostly n-6 polyunsaturated fat on coronary heart disease: a meta-analysis of randomised controlled trials, Nutrition Journal 2017 16:30
Only one recent meta analysis conducted by the American Heart Association (by the authors of the Diet-Heart Policy for Americans, mentioned above) found a relationship between saturated fat intake and coronary heart disease, yet failed to examine cardiovascular mortality (death) or total mortality [22].
NOTE: In 1961, the American Heart Association was the author of the original policy paper recommending to limit saturated fats to protect against heart disease and therefore has a significant interest in defending its longtime institutional position.
With the exception of the American Heart Association review, the conclusion of 9 different meta-analysis and review papers of randomized control trials conducted by independent teams of scientists worldwide do not support the belief that dietary intake of saturated fat causes heart disease.
The PURE (Prospective Urban Rural Epidemiology) was the largest-ever epidemiological study and was published in The Lancet in December 2017 [23]. It recorded dietary intake in 135,000 people in 18 countries over an average of 7 1/2 years, including high-, medium- and low-income nations. It found;
“High carbohydrate intake was associated with higher risk of total mortality, whereas total fat and individual types of fat were related to lower total mortality. Total fat and types of fat were not associated with cardiovascular disease, myocardial infarction, or cardiovascular disease mortality, whereas saturated fat had an inverse association with stroke. Global dietary guidelines should be reconsidered in light of these findings.”
Dehghan M, Mente A, Zhang X et al, The PURE Study – Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. Lancet. 2017 Nov 4;390(10107):2050-2062
Those critical of the study say that it has methodological problems, including problems related to the authors dividing consumption of macronutrients (protein, fat and carbohydrate) into 4 groups (quintiles). Some say that this is reason the data showed an inverse relationship between saturated fat and cardiovascular disease [24]. Criticisms also include that one cannot compare data between countries of substantially different level of income because “low fat consumption is very uncommon in high income countries” and that ‘the ability to afford certain foods may change the dietary pattern (e.g. high-carbohydrate and low-fat diets may be associated with poverty) [24].
Final thoughts…
Both the American and Canadian governments are currently in the process of revising their Dietary Guidelines and I feel that what is needed now is an external, independent scientific review of the current evidence-base for the belief that saturated fat contributes to heart disease.
Have questions or need support following a low carb lifestyle in a way that makes sense for you?
Please send me a note using the “Contact Me” tab above and I will reply shortly.
Keys A, Aravanis C, Blackburn HW et al. Epidemiological studies related to coronary heart disease: characteristics of men aged 40—59 in seven countries Acta Med Scand 1967 460: 1—392.
McGandy, RB, Hegsted DM, Stare,FJ. Dietary fats, carbohydrates and atherosclerotic vascular disease. New England Journal of Medicine. 1967 Aug 03; 277(5):242—47
The National Diet-Heart Study Final Report.” Circulation, 1968; 37(3 suppl): I1-I26. Report of the Diet-Heart Review Panel of the National Heart Institute. Mass Field Trials and the Diet-Heart Question: Their Significance, Timeliness, Feasibility and Applicability. Dallas, Tex: American Heart Association; 1969, AHA Monograph no. 28.
Introduction to the Dietary Goals for the United States — by Dr D.M. Hegsted. Professor of Nutrition, Harvard School of Public Health, Boston, MASS., page 17 of 130, https://naldc.nal.usda.gov/naldc/download.xhtml?id=1759572&content=PDF
McDonald BE, The Canadian experience: why Canada decided against an upper limit for cholesterol, J Am Coll Nutr. 2004 Dec;23(6 Suppl):616S-620S.
Tribble DL, Holl LG, Wood PD, et al. Variations in oxidative susceptibility among six low density lipoprotein subfractions of differing density and particle size. Atherosclerosis 1992;93:189—99
Gardner CD, Fortmann SP, Krauss RM, Association of Small Low-Density Lipoprotein Particles With the Incidence of Coronary Artery Disease in Men and Women, JAMA. 1996;276(11):875-881
Lamarche B, Tchernof A, Moorjani S, et al, Small, Dense Low-Density Lipoprotein Particles as a Predictor of the Risk of Ischemic Heart Disease in Men, Circulation. 1997;95:69-75
Packard C, Caslake M, Shepherd J. The role of small, dense low density lipoprotein (LDL): a new look, Int J of Cardiology, Volume 74, Supplement 1, 30 June 2000, Pages S17-S22
Genest JJ, Blijlevens E, McNamara JR, Low density lipoprotein particle size and coronary artery disease, Arteriosclerosis, Thrombosis, and Vascular Biology. 1992;12:187-195
Siri-Tarino PW, Sun Q, Hu FB, Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease, The American Journal of Clinical Nutrition, Volume 91, Issue 3, 1 March 2010, Pages 502—509
Mensink RP, Zock PL, Kester A, Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials, The American Journal of Clinical Nutrition, Volume 77, Issue 5, 1 May 2003, Pages 1146—1155
Toth PP, The “Good Cholesterol” – High Density Lipoprotein, Circulation 2005;111:e89-e91
Skeaff CM, PhD, Professor, Dept. of Human Nutrition, the University of Otago, Miller J. Dietary Fat and Coronary Heart Disease: Summary of Evidence From Prospective Cohort and Randomised Controlled Trials, Annals of Nutrition and Metabolism, 2009;55(1-3):173-201
Hooper L, Summerbell CD, Thompson R, Reduced or modified dietary fat for preventing cardiovascular disease, 2012 Cochrane Database Syst Rev. 2012 May 16;(5)
Chowdhury R, Warnakula S, Kunutsor S et al, Association of Dietary, Circulating, and Supplement Fatty Acids with Coronary Risk: A Systematic Review and Meta-analysis, Ann Intern Med. 2014 Mar 18;160(6):398-406
Schwingshackl L, Hoffmann G Dietary fatty acids in the secondary prevention of coronary heart disease: a systematic review, meta-analysis and meta-regression BMJ Open 2014;4
Hooper L, Martin N, Abdelhamid A et al, Reduction in saturated fat intake for cardiovascular disease, Cochrane Database Syst Rev. 2015 Jun 10;(6)
Harcombe Z, Baker JS, Davies B, Evidence from prospective cohort studies does not support current dietary fat guidelines: a systematic review and meta-analysis, Br J Sports Med. 2017 Dec;51(24):1743-1749
Ramsden CE, Zamora D, Majchrzak-Hong S, et al, Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-73), BMJ 2016; 353
Hamley S, The effect of replacing saturated fat with mostly n-6 polyunsaturated fat on coronary heart disease: a meta-analysis of randomised controlled trials, Nutrition Journal 2017 16:30
Sachs FM, Lichtenstein AH, Wu JHW et al, Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association, Circulation. 2017 Jul 18;136(3)
Dehghan M, Mente A, Zhang X et al, The PURE Study – Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. Lancet. 2017 Nov 4;390(10107):2050-2062
Sigurdsson, AF, The Fate of the PURE Study — Fat and Carbohydrate Intake Revisited, Doc’s Opinion, October 16 2017, www.docsopinion.com/2017/10/16/pure-study-fats-carbohydrates/
Note: References 11-23 were from a document prepared by the Nutrition Coalition
Special thanks to Dr. Carol Loffelmann and Dr. Barbra Allen Bradshaw of The Canadian Clinicians for Therapeutic Nutrition for their tireless research.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Some people imagine that a low carb lifestyle involves plates laden with bacon and eggs, huge steaks and meals devoid of vegetables, dairy foods, and nuts or seeds, but this is a misconception.
While there are individuals that choose to eat ”zero-carb” for a variety of personal reasons, it is not something I promote outside of being prescribed by a physician for therapeutic management of a specific medical condition.
I encourage people to eat a wide variety of low carb vegetables, some fruit and dairy products, as well as nuts and seeds — all of which have some carbohydrate in them. There is no one-size-fits-all low carb diet, but there are a few low carbohydrate approaches which can be chosen from depending on a person’s medical and metabolic conditions, any medications they may be taking, as well as stage of life and lifestyle factors.
Another fallacy is that low carb diets involve ”lots of meat for dinner” and “eggs every morning for breakfast” but people eating low carb can eat a wide variety of food for breakfast and meals can be vegetarian or pescatarian (include fish and seafood) and involve no meat whatsoever. This makes a low carb suitable for those that don’t eat meat or eggs for religious or ethical reasons.
Three main low carb approaches are;
(1) low carb higher protein
(2) low carb higher healthy fat
(3) higher protein / lower fat intake during weight loss, then a moderate protein / high healthy fat intake during weight maintenance.
What makes a low carb diet ketogenic is the low amount of carbohydrate that is eaten relative to the overall caloric intake, so not all low carb diets are ketogenic.
Low carbohydrate and therapeutic ketogenic diets have a variety of clinical applications. For example, a ketogenic diet may be prescribed by a person’s physician for management of epilepsy or seizure disorder, for treatment of some kinds of cancer, or for weight loss before and after bariatric surgery. Different types of low carb diets may be used for improving insulin sensitivity in Type 2 Diabetics or those with pre-diabetes, improving fatty liver disease, for reducing symptoms of Polycystic Ovarian Syndrome (PCOS) or for gradual weight loss.
[Another misconception is that low carb diets are used for ”rapid weight loss”, which is not the case.]
For each type of low carb diet the ratio of protein to fat is specific to the clinical condition and person’s requirements. Everybody’s macronutrient needs (the amount of protein, carbs and fat they require) as well as overall energy needs are different and are dependent on several factors including their gender, age, height, weight, clinical conditions and any medications they’re taking.
Our body requires essential amino acids found in the protein foods we eat, as well as essential fatty acids found in the different types of fat we eat, along with essential vitamins and minerals however there is no essential requirement for dietary carbohydrate – provided that ”adequate amounts of protein and fat are consumed” (Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids, 2005). This article will elaborate, but explaining it in simple terms, it means is that our body does not need to have carbohydrate in food if we eat sufficient protein with all the essential amino acids and sufficient fat with the essential fatty acids.
That doesn’t mean that I recommend that people without a clinical reason eat food with no carbohydrate in it (I don’t), as they wouldn’t be able to eat any vegetables, fruit, dairy, nuts or seeds – as these all of these have some carbohydrate in them.
I encourage people to eat a wide range of food from a variety of categories to ensure they have adequate dietary intake. I recommend whole, unprocessed foods that are naturally low in carbohydrate, including non-starchy vegetables, plant fats (such as olive oil, avocado oil, macadamia or walnut oil, coconut oil), low sugar fruit (such as tomato, lemon, lime, cucumber), meat, fish, poultry and seafood of all varieties, and small amounts of animal fat such as butter and cream.
If people working toward losing weight then the fat that is naturally found in meat is okay, but I would encourage them to trim excess visible fat.Unless there is a compelling reason not to, folks can add a bit of cream to their coffee or some butter on top of their cooked vegetables if they like it (especially if they’ll eat more veggies that way) but I don’t encourage people to ‘add fat’ to foods for the sake of adding fat (e.g. ‘bulletproof’ coffee or ‘fat bombs’). That said, there is nothing intrinsically ‘dangerous’ about eating fat, even saturated fat but what needs to be considered is “how much” and “how often”.
High blood cholesterol and high triglycerides is the result of eating too much carbohydrate, not eating too much saturated fat, or dietary cholesterol.
A healthy person that eats more carbohydrate than their body can use will move the excess carbohydrate they eat off to their liver and will make triglyceride and LDL cholesterol and store the rest as fat. A person who is insulin resistant or has Type 2 Diabetes may have high blood sugar levels but even if a person has normal blood sugar levels, their high carbohydrate intake may be reflected in their “cholesterol tests”. Often what we see in such cases is high triglyceride results or high LDL cholesterol results or both. This easy-to-understand article titled Understand High Blood Sugar & High Cholesterol will explain the process in more detail. If eating excess carbohydrates continues for an extended period of time, it ‘s possible that non-alcoholic fatty liver disease (NAFL) may develop.
Each person’s ability to tolerate carbohydrate is different — depending whether they are insulin sensitive, insulin resistant or Type 2 Diabetic. Someone who is insulin sensitive for example can eat considerably more carbohydrate without causing a spike in their blood glucose level than someone who is insulin resistant. For those who are Type 2 Diabetic, both the degree of insulin resistance and the length of time they’ve been Type 2 Diabetic will affect the amount of carbohydrates they can tolerate. To explain this, I like to use the analogy of ‘lactose intolerance’. Some people who are lactose intolerant can manage to drink and eat milk products, provided the quantities are small and the person doesn’t have it too often. Others who are lactose intolerant can’t even tolerate a small amount of lactose without symptoms. Ability to tolerate carbohydrate is similar. People who are insulin sensitive or only mildly insulin resistance will be able to tolerate more carbohydrate than those who are very insulin resistant or have had Type 2 Diabetes a long time.
The average intake of carbohydrate in the Canadian diet is ~ 300 g per day, which is a lot. People who are insulin sensitive or mildly insulin resistance may do well lowering their carbohydrate amount to a moderate level whereas those who are insulin resistant or Type 2 Diabetic will likely need to eat considerably less carbohydrate in order to begin to see their blood sugar levels or cholesterol / triglyceride levels come down.
Factors that can affect how much carbohydrate a person can tolerate include gender, whether or not they are insulin sensitive or insulin resistant (and to what degree) and whether they have Type 2 Diabetes and if so, for how long.
What some people find challenging about deciding to follow a low carb lifestyle is knowing how much protein they need to eat, the amount and types of fat they can use, as well as the total amount of carbohydrate they can tolerate, as well as how those carbohydrates should best be distributed throughout the day.
Where it becomes particularly challenging is when people have Type 2 Diabetes or high blood pressure and are prescribed medications for these conditions. In such cases, it’s not as simple as them just “cutting carbs” because by not doing so gradually it could result in a sudden drop in blood sugar or blood pressure which could be dangerous. People taking medications for these conditions (or for some other conditions) need to be monitored by their doctors and the reality is that not all doctors have more than a few minutes to see patients and may not feel equipped to counsel them on diet. This is where working with a Dietitian that’s knowledgeable and familiar with the use low carb diet is very helpful as they can coordinate dietary and lifestyle changes with your doctor while they monitor your health and adjusts the levels of prescribed medications, as needed.
Another situation where it can be very helpful to have a Dietitian’s support is when youth or teenagers need to lose weight, or bring down their blood sugar, cholesterol or blood pressure levels, because a there’s a need to ensure that they have adequate intake to support healthy growth.
Have questions?
Please send me an note using the “Contact Me” form on the tab above and I will reply as I am able.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
It occurred to me that the time frame for an epidemic to occur is absolutely critical in determining public response. If rates of a disease went from 1 in 10 people to 1 in 3 people in only 10 years, there would be public outcry for scientists to determine the cause and to find a cure quickly. If the disease caused debilitating metabolic effects such as very high blood pressure that resulted in heart attacks or strokes and people of all ages were getting this disease, with many dying – the outcry would be even more urgent.
But what if rates of the same disease went from 1 in 10 people to 1 in 3 people over a period of 40 or 50 years? The current generation would have no recollection of what it was like ‘before’ because things had always been this way since they were kids. The older generation would remember what it was like ‘before’ and concluding that for whatever reason, that is the way it is now. Doctors and scientists of the older generation that might be able to apply their knowledge and skill to find the cause and a cure would be at the end of their working lives.
The disease is obesity.
Debilitating metabolic side effects of obesity include very high blood pressure that can lead to heart attacks and strokes and Type 2 Diabetes which can result in blindness, amputations and organ failure.
Once a rare disease, obesity has now reached epidemic proportions and the metabolic side effects are not just for the old, but are rampant among youth and young adults.
This disease epidemic has taken place over 50 years but few are noticing because it has fallen between the cracks of time.
Obesity Rates Then and Now
Photographs and videos of what people looked like fifty years ago are widely available, and a simple Google search will provide an abundance of them. Movies, documentaries and TV shows from the mid-1960s also provide a glimpse of what the average American and average Canadian looked like then.
In the 1960s only 10.7% of the US population and 10.2% of the Canadian population were obese; that’s approximately 1 in 10 people.
Below is a US sorority photo of a Sigma Iota Chi chapter from West Virginia from 1967. Look how slim most of the women are compared to today’s young adults.
Sigma Iota Chi Sorority – West Virginia – 1967 (https://sororityhistories.wordpress.com/tag/sigma-iota-chi/)
West Virginia now has one of the highest adult obesity rate in the US.
1967 Kappa Alpha Fraternity Party Photograph – Cornell University
To the left is another photo from a 1967 Fraternity party at Cornell University. For the most part, the young men and their girlfriends are slim and lean – certainly much slimmer than university students today.
Below is what the average city-dwelling Canadian looked like in 1967, riding the subway in Toronto. Young adults, middle aged adults and older people were very slim compared to today’s standards – especially when compared to what the average public transit rider looks like today.
Most recent international data from 2015 found that 38.2% of the US population and 25.8% of the Canadian population are obese; that’s more than 1 in 3 people in the US and more than 1 in 4 people in Canada [1].
People in both countries are now some of the most obese in the world;
OECD Health Statistics 2017, June 2017
When one compares what university students looked above to what they look like now in a current photo of Fraternities and Sororities below, the difference in average body weight of the students from 50 years ago to today is quite apparent – despite the fact that university students come from families where the average family income is significantly higher than the national average.
Given this, their higher body weights cannot be dismissed due to low income, socioeconomic status or lack of education. So what is going on?
University of Nevada’s Fraternity and Sorority Community
What changed in the last 50 years that contributed to this obesity epidemic?
As written about in a previous article, in 1967 (fifty years ago) the sugar industry paid three Harvard researchers (Stare, Hegsted and McGandy) very handsomely to critique studies that vindicated sugar as contributing to abnormal fat metabolism and heart disease, and who instead laid the blame on dietary fat, and in particular saturated fat and dietary cholesterol [2,3].
They concluded;
”Since diets low in fat and high in sugar are rarely taken, we conclude that the practical significance of differences in dietary carbohydrate is minimal in comparison to those related to dietary fat and cholesterol…the major evidence today suggests only one avenue by which diet may affect the development and progression of atherosclerosis. This is by influencing the levels of serum lipids [fats], especially serum cholesterol.” [4]
These researchers who were sponsored by the sugar industry concluded that there was “major evidence” which suggested that there was only ONE avenue for diet to contribute to hardening of the arteries and the development of heart disease – and that was dietary fat and cholesterol…yet only a year later in 1968, the Diet-Heart Review Panel of the National Heart Institute recommended that a major study be conducted to determine whether changes in dietary fat intake prevented heart disease – because such a study had not yet been done[5].
No major study had yet been done to find out whether changing the types of fat we ate prevented heart disease, yet these researchers were SO certain that there was “only one avenue” for diet to contribute to hardening of the arteries and the development of heart disease. How much was their certainly impacted by their sponsors?
Their influence didn’t end there.
Only ten years later, one of the three Harvard researchers (Hegsted) was directly involved with developing and editing the 1977 US Dietary Guidelines [6] which recommended a decrease in saturated fat and cholesterol consumption, and an increase in dietary carbohydrate. While Canadian Dietary Guidelines are distinct from the US ones, much of the research on which they are based is the same.
Comparing the US to Canadian dietary recommendations with respect to the consumption of fat in general, as well as the consumption of saturated fat in particular, one finds the recommendations mirror each other.
We are told to limit saturated fat ostensibly because of its negative impact on blood cholesterol and heart disease. We are told to increase consumption of vegetable oils, and to substitute polyunsaturated fats for saturated fat in cooking and baking and to eat 45-65% of our daily calories as carbohydrate.
It is increasingly my conviction that the simultaneous (1) marketing of polyunsaturated vegetable oil – more accurately called industrially-created seed oils, such as soybean oil and canola oil, along with (2) changes in the Dietary Recommendations in both Canada and the US for people to (a) limit calories from fat and especially to (b) limit saturated fat, combined with the recommendations for people to (c) eat 45-65% of calories as carbohydrate created the “perfect storm” that when viewed together, explains the obesity epidemic we now have and the associated increase in metabolic health problems that we now see 50 years later.
I will be writing more in the days ahead on what is thought to be the role of these industrially-created seed oils in the process of obesity and inflammation that underlies many metabolic conditions, including Type 2 Diabetes.
Why isn’t the public alarmed by this massive increase in obesity?
I believe it’s becauseit took place over such a long period of time that those old enough to remember what things were like before have either died or are approaching retirement age and have left its solution to the next generation, and those young enough to do something about it have never known it any other way.
I think that looking at the magnitude of the epidemic without the time frame is helpful.
What if only 10 years ago, only 1 in 10 people were obese and now 1 in 3 people were obese? Would there not be a public outcry for scientists to determine what caused this and to research to find a cure quickly?
Obesity underlies debilitating metabolic effects such as very high blood pressure that can lead to heart attacks and strokes and people of all ages are getting this disease – including children and teenagers. Obesity underlies the huge increase in Type 2 Diabetes and when poorly managed can result in blindness, limb amputation and organ failure. People of all ages are dying from these metabolic effects of these disease, which at present are mainly being managed through medication and advising people to “eat less and move more”.
Is that the best we can do to curb this epidemic?
As covered in previous articles, there are peer-reviewed published studies – some a year or two long, that demonstrate that these metabolic effects can be put into remission by eating a diet with less carbohydrates – yet government-funded research into use of this is not a priority.
Why?
What role does the sugar industry and the corn-producers (that manufacturer high fructose corn syrup found in much of our packaged food) play?
What role do the grain boards (that market wheat and other grains for baked goods) play?
What about the soybean and canola growers – multi-billion dollar a year industries in both countries that grows the soybeans and canola seed that are processed into fats sold to consumers for cooking and baking?
These industries and their respective lobby groups play an influential role in the economies of both Canada and the United States and in that way (and others) influence what types of research should be funded.
There is an epidemic going on and people are living with terrible metabolic consequences of them or dying from them.
Before the Dietary Guidelines are updated in both countries, the governments of Canada and the US must approve external, independent scientific review of the evidence-base for the existing dietary recommendation as well as examine the evidence-base for use of a well- designed low carbohydrate diet in reducing obesity and managing the debilitating metabolic effects.
The length of time since the obesity epidemic began does not make this any less urgent.
Do you have questions about how I can help you in tackling obesity and lowering or putting metabolic side effects into remission?
Please send me a note using the “Contact Me” form located on the tab above.
OECD Health Statistics 2017, June 2017, http://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf
Kearns C, Schmidt LA, Glantz SA, et al. Sugar Industry and Coronary Heart Disease Research: A Historical Analysis of Internal Industry Documents. JAMA Intern Med. 2016 Nov 01; 176(11):1680-1685.
Husten, L, How Sweet: Sugar Industry Made Fat the Villain, Cardio|Brief, 2016 Sept 13.
McGandy, RB, Hegsted DM, Stare,FJ. Dietary fats, carbohydrates and atherosclerotic vascular disease. New England Journal of Medicine. 1967 Aug 03; 277(5):242—47
The National Diet-Heart Study Final Report.” Circulation, 1968; 37(3 suppl): I1-I26. Report of the Diet-Heart Review Panel of the National Heart Institute. Mass Field Trials and the Diet-Heart Question: Their Significance, Timeliness, Feasibility and Applicability. Dallas, Tex: American Heart Association; 1969, AHA Monograph no. 28.
Introduction to the Dietary Goals for the United States — by Dr D.M. Hegsted. Professor of Nutrition, Harvard School of Public Health, Boston, MASS., page 17 of 130, https://naldc.nal.usda.gov/naldc/download.xhtml?id=1759572&content=PDF
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This is Part 1 in a new series titled Bad Fat Enduring Beliefs and this article looks at how and when saturated fat was vilified and why sugar was vindicated as the cause of heart disease.
The Diet-Heart Hypothesis
The diet-heart hypothesis is the belief that eating foods high in saturated fat contributed to heart disease was first proposed in the 1950s by a scientist named Ancel Keys who believed that by replacing saturated fat from meat, butter and eggs with newly-created industrial polyunsaturated vegetable oil (such as soybean oil) that heart disease and the deaths allegedly associated with it would be reduced by lowering blood cholesterol levels.
In 1952, Keys suggested that Americans should reduce their fat consumption by 1/3 and in 1953, Keys published a study where he said that he had demonstrated that there was an association between dietary fat as a percentage of daily calories and death from degenerative heart disease [1].
Four years later, in 1957, Yerushalamy et al published a paper with data from 22 countries[2] which showed a weak relationship between dietary fat and death by coronary heart disease — a much weaker relationship than was suggested by Keys’s in 1953. Nevertheless, in 1989 Keys and colleagues published their Seven Countries Study[3] which maintained there was an associative relationship between increased dietary saturated fat and Coronary Heart Disease — basically ignoring the data presented in Yerushalamy’s 1957 study, and which failed to study countries where Yerushalamy found no relationship between dietary fat and heart disease, such as in France. The paper maintained that the average consumption of animal foods (with the exception of fish) was positively associated with 25-year Coronary Heart Disease death rates and the average intake of saturated fat was strongly related to 10 and 25-year Coronary Heart Disease death rates. Keys and colleagues knew of the Yerushalamy’s data from 1957 and seemingly dismissed it.
Keys et al – Epidemiological studies related to coronary heart disease: characteristics of men aged 40—59 in seven countries [1]
Yerushalmy J, Hilleboe HE. Fat in the diet and mortality from heart disease. A methodologic note [2]The paper has been widely criticized for selecting data only from the 7 countries that best fit their Diet Heart Hypothesis.
The Sugar Industry Funding of Research Vilifying Fat
In August of 1967, Stare, Hegsted and McGandy – the 3 Harvard researchers paid by the sugar industry published their review inthe New England Journal of Medicine,titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which vindicated sugar as a contributor of heart disease and laid the blame on dietary fat and in particular, saturated fat and dietary cholesterol (previous article on that topic here).
Stare, Hegsted and McGandy concluded that there was “only one avenue” by which diet contributed to the development and progression of “hardening of the arteries” (atherosclerosis) and resulting heart disease and that was due to how much dietary cholesterol people ate and its effect on blood lipids;
”Since diets low in fat and high in sugar are rarely taken, we conclude that the practical significance of differences in dietary carbohydrate is minimal in comparison to those related to dietary fat and cholesterol…the major evidence today suggests only one avenue by which diet may affect the development and progression of atherosclerosis. This is by influencing the levels of serum lipids [fats], especially serum cholesterol.” [4]
These researchers concluded that there was major evidence available at the time which suggested that there was only ONE avenue for diet to contribute to hardening of the arteries and the development of heart disease – yeta year later in 1968 the report of the Diet-Heart Review Panel of the National Heart Institute made the recommendation that a major study be conducted to determine whether changes in dietary fat intake prevented heart disease because such a study had not yet been done [5];
”the committee strongly recommended to the National Heart Institute that a major definitive study of the effect of diet on the primary prevention of myocardial infarction be planned and put into operation as soon as possible. “
This is an important point; prior to a major study having ever been conducted to determine whether changes in dietary cholesterol impacts heart disease, 3 Harvard researchers paid by the sugar industry concluded that there was “only one avenue” by which diet contributed to the development and progression of atherosclerosis (i.e. “hardening of the arteries”) and heart disease and that was due to how much dietary cholesterol people ate and its effect on blood lipids.
Researcher Paid by the Sugar Industry Helps Develop the 1977 US Dietary Guidelines
Only ten years after the sugar industry paid Stare, Hegsted and McGandy to write their reviews, the same Dr. Hegsted was directly involved with developing and editing the 1977 US Dietary Guidelines [6] which recommended an increase in dietary carbohydrate and a decrease in saturated fat and cholesterol in the diet.
Historic changes in the Dietary Recommendation in Canada have largely been based on changes to the Dietary Recommendations in the US, and as a result both stemmed from a belief that eating saturated fat increases total cholesterol and therefore increases the risk of heart disease.
The problem is this belief is just that, a belief.
There have been many studies that have disproved this including a randomized, controlled dietary intervention trial from 2008 which compared a low calorie, low in fat with a low carbohydrate, high fat diet of the same number of calories. This study found that overall heart health is significantly improved when carbohydrate is restricted, rather than fat [7,8].
Not all LDL cholesterol is “bad” cholesterol.
Small, dense LDL (“Pattern B”) causes more “hardening of the arteries” than the large, fluffy LDL particles (“Pattern A”)[9].
It has been reported that when dietary fat is replaced by carbohydrate, the percentage of the small, dense LDL particles (the ones that cause hardening of the arteries) is increased, increasing risk for heart disease. Furthermore, the low carb diet increased HDL (so-called “good” cholesterol), which are protective against heart disease and HDL and small, dense LDL were made worse on the low fat diet. Quite opposite to the “Diet-Heart Hypothesis, this study demonstrated improvements in the risk of heart disease for those eating a low carbohydrate, high fat diet compared to those eating a low fat, low calorie diet – which is not all that surprising given that it had been reported previously that a diet high in saturated fat actually lowers small, dense LDL (the type of LDL that causes hardening of the arteries) and raises the large fluffy LDL; actually improving risk factors for heart disease [15].
There are also other randomized controlled trials from 2004-2008 which demonstrate that a low carb diet improves blood cholesterol test results more than a low fat diet [10,11,12,13,14] – yet despite this, the belief that eating saturated fat increases blood cholesterol, persists.
Both the American and Canadian governments are in the process of revising their Dietary Guidelines and what is clear is that what is needed is an external, independent scientific review of the current evidence-base for the enduring false belief that dietary fat, especially saturated fat contributes to heart disease.
Have questions about how I can help you follow a low carb lifestyle?
Please send me a note using the “Contact Me” tab above and I will reply shortly.
KEYS, A., Prediction and possible prevention of coronary disease. Am J Public Health Nations Health, 1953. 43(11): p. 1399-1407.
Yerushalmy J, Hilleboe HE. Fat in the diet and mortality from heart disease. A methodologic note. NY State J Med 1957;57:2343—54
Kromhout D, Keys A, Aravanis C, Buzina R et al, Food consumption patterns in the 1960s in seven countries. Am J Clin Nutr. 1989 May; 49(5):889-94.
McGandy, RB, Hegsted DM, Stare,FJ. Dietary fats, carbohydrates and atherosclerotic vascular disease. New England Journal of Medicine. 1967 Aug 03; 277(5):242—47
The National Diet-Heart Study Final Report.” Circulation, 1968; 37(3 suppl): I1-I26. Report of the Diet-Heart Review Panel of the National Heart Institute. Mass Field Trials and the Diet-Heart Question: Their Significance, Timeliness, Feasibility and Applicability. Dallas, Tex: American Heart Association; 1969, AHA Monograph no. 28.
Introduction to the Dietary Goals for the United States — by Dr D.M. Hegsted. Professor of Nutrition, Harvard School of Public Health, Boston, MASS., page 17 of 130, https://naldc.nal.usda.gov/naldc/download.xhtml?id=1759572&content=PDF
Volek JS, Fernandez ML, Feinman RD, et al. Dietary carbohydrate restriction induces a unique metabolic state positively affecting atherogenic dyslipidemia, fatty acid partitioning, and metabolic syndrome. Prog Lipid Res 2008;47:307—18
Forsythe CE, Phinney SD, Fernandez ML, et al. Comparison of low fat and low carbohydrate diets on circulating fatty acid composition and markers of inflammation. Lipids 2008;43:65—77
Tribble DL, Holl LG, Wood PD, et al. Variations in oxidative susceptibility among six low density lipoprotein subfractions of differing density and particle size. Atherosclerosis 1992;93:189—99
Foster GD, Wyatt HR, Hill JO, et al. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med 2003;348:2082—90.
Stern L, Iqbal N, Seshadri P, et al. The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: one-year follow-up of a randomized trial. Ann Intern Med 2004;140:778—85
Gardner C, Kiazand A, Alhassan S, et al. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women. JAMA 2007;297:969—77
Yancy WS Jr., Olsen MK, Guyton JR, et al. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: a randomized, controlled trial. Ann Intern Med 2004;140:769—77
Shai I, Schwarzfuchs D, Henkin Y, et al. Dietary Intervention Randomized Controlled Trial (DIRECT) Group. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med 2008;359:229—41
Dreon DM, Fernstrom HA, Campos H, et al. Change in dietary saturated fat intake is correlated with change in mass of large low-density-lipoprotein particles in men. Am J Clin Nutr 1998;67:828—36
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Yesterday, in preparing to begin a new series of articles on the relationship between polyunsaturated vegetable fats to obesity, I came across an old, yellowed sheet titled “Comparison of Dietary Fats” that I was given as an undergrad Dietetic student at McGill, in 1989.
(reverse side) Comparison of Dietary Fats — ”Provided as a Professional Service by Proctor & Gamble”, 1989 – full size photo, below
It was designed to help us teach consumers how to choose the “healthiest” dietary fats.
As indicated at the bottom of both sides of the handout (see full size photos, below), it was “provided as a Professional Service by Proctor and Gamble“.
Why would Proctor and Gamble, a soap company provide future Dietitians with a teaching handout on choosing healthy oils for cooking? A bit of understanding about how soap is made, will help.
At the time, the making of soap required a mixture of animal fats and lye, however William Procter and James Gamble (brothers-in-law living in Cincinnati in the late 1800s and who formed Proctor and Gamble) needed to find an inexpensive replacement for animal fat for the creation of individually wrapped bars of soap.
The source of soap fat they turned to was a waste-product of the cotton industry – cottonseed oil. It was literally the garbage leftover when cotton was produced and is cloudy, red and bitter to the taste,and toxic to most animals.
They needed to make cottonseed oil solid in order to make bar soap and utilized a newly patented technology to produce a creamy, pearly white substance out of cottonseed oil. This fat resembled lard (the most popular natural animal fat baking and frying fat at the time), so with a little more tweaking, this hydrogenated cottonseed oil was then sold in 1911 by Procter & Gamble to home cooks as Crisco® shortening.
All that was needed now was for Proctor and Gamble to market this industrially-produced seed oil fat, and market it they did. They hired America’s first full-service advertising agency, the J. Walter Thompson Agency that employed graphic artists and professional writers.
“Samples of Crisco were mailed to grocers, restaurants, nutritionists, and home economists. Eight alternative marketing strategies were tested in different cities and their impacts calculated and compared.
Doughnuts were fried in Crisco and handed out in the streets.
Women who purchased the new industrial fat got a free cookbook of Crisco recipes. It opened with the line, “The culinary world is revising its entire cookbook on account of the advent of Crisco, a new and altogether different cooking fat.” [1]
From the very beginning, Proctor and Gamble marketed their industrially-created solid fat (Crisco®) to “nutritionists” and “home economists” – the forerunners to Dietitians.
When Procter & Gamble introduced Puritan Oil® in 1976, a liquid cooking oil made of sunflower oil which became 100% canola oil by 1988, it was natural for them to market their newly created oil to Dietitians.
Proctor & Gamble now had a lucrative business manufacturing industrial seed oils as dietary fats and they wanted to make sure that we, as Dietitians encouraged people to use their “healthy” fats.
I’ve scanned in both sides of the handout (it’s old and yellowed, having been kept in the back of my “new” 1988 Canada’s Food Guide book for almost 30 years). As can be seen, in first place on the front side of the handout is canola oil identified by the trade name “Puritan Oil®”, a registered trademark of Proctor and Gamble.
(front side) Comparison of Dietary Fats – “Provided as a Professional Service by Proctor & Gamble”, 1989
On the reverse side, is what consumers should know about these oils, including that canola oil is “better than all other types of vegetable oil“.
(reverse side) Comparison of Dietary Fats – “Provided as a Professional Service by Proctor & Gamble”, 1989
I’ve highlighted some of the wording that makes Proctor & Gamble’s bias apparent;
(reverse side) Comparison of Dietary Fats – “Provided as a Professional Service by Proctor & Gamble”, 1989 – red text mine
Some Final Thoughts…
From the very beginning, industrially-produced seed fats and oils have been marketed to nutritionists, home economists and Dietitians by the companies that created them, in some cases as a “Professional Service”.
As will become clear in the next article we, as Dietitians were tasked by the Dietary Guidelines in both Canada and the US with promoting “polyunsaturated vegetable oils” to the public as ‘healthful alternatives’ to presumably unhealthy saturated animal fats. The manufacturers were there to ‘assist’ as a ‘Professional Service’.
Looking back on the role of fat manufacturers and the sugar industry (outlined in the preceding article) on which foods were recommended and promoted, it makes me question what I was taught and who affected what I was taught. Given that it was known at the time the sugar industry funded the researchers that implicated saturated fat as the alleged cause of heart disease, I wonder what we don’t know about which industry funded which research. After all, the knowledge about the sugar industry having funded the researchers that implicated saturated fat only ‘came out’ in November 2016 when it had occurred decades earlier.
NOTE: It is increasingly my conviction that the simultaneous (1) marketing of polyunsaturated vegetable oil (soybean oil, canola oil) along with (2) changes in the Dietary Recommendations for people to (a) eat no more than 20- 30% of calories from fat and to (b) limit saturated fat to no more than 10% of calories, combined with the recommendations for people to (c) eat 45-65% of calories as carbohydrate was the “perfect storm” that may well explain the current obesity crisis and associated increase in metabolic health problems that we now see 40 years later.
In subsequent articles I’ll elaborate on why I believe this is the case.
Ramsey, D*., Graham T., The Atlantic. How Vegetable Oils Replaced Animal Fats in the American Diet, April 26 2012 (www.theatlantic.com/health/archive/2012/04/how-vegetable-oils-replaced-animal-fats-in-the-american-diet/256155/)
*Dr. Drew Ramsey, MD is an assistant clinical professor of psychiatry at Columbia University.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Most criticism of a low carb lifestyle or ketogenic diet centers around a few common misconceptions including that such a lifestyle is “restrictive”, “imbalanced”, or that it’s “not sustainable”. This article addresses all three.
Firstly, as explained in an earlier post there isn’t a single “low carb” diet but basically 3 styles;
(1) low carb high protein
(2) low carb high fat approach
(3) higher protein lower fat intake during weight loss, then a moderate protein high fat intake during weight maintenance
What makes a low carb diet“keto” is the amount of carbohydrate that is eaten.
There are different types of therapeutic ketogenic diets which have different clinical applications, including use in epilepsy and seizure disorder, specific types of cancer, Polycystic Ovarian Syndrome (PCOS), weight loss and improving insulin sensitivity and in each case, the ratio of protein to fat is specific to the condition (and in cases of weight loss and improving insulin sensitivity, to the individual).
While our bodies have an absolute requirement for essential amino acids, and essential fatty acids, as covered in detail in an earlier article, according to the Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids (2005) there is no essential need for dietary carbohydrate provided that ”adequate amounts of protein and fat are consumed“.
That is, a low carb or ketogenic diet can be ‘complete’ as long as it supplies adequate amounts of protein (with all essential amino acids) and fat (with the essential fatty acids) and also provides the other nutrients the body requires (such as vitamins and minerals).
This is where I can help. I’ll design a nutritionally adequate Meal Plan specifically for you, in light of any clinical conditions you may have and factoring in your goals in choosing to eat this way.
Let me address the common (but unfounded) misconceptions that a low carb or ketogenic diet is “restrictive”, “imbalanced” or “not sustainable”.
A Low Carb or Keto Diet is “restrictive”, “imbalanced” or “not sustainable”
Usually, when people make comments like these, they have absolutely no idea that there are different types of low carb and keto diets. Ketogenic diets used in epilepsy and seizure disorder are very specific, as are ketogenic diets used for those with specific types of cancer. Ketogenic diets used to target insulin resistance associated with Type 2 Diabetes or pre-Diabetes are different again.
Foods and ratios of foods eaten when following a low carb diet targeting insulin resistance based on Dr. Jason Fung’s approach will differ somewhat from a low carb diet based on Dr. Eric Westman’s approach. A low carb diet based on Dr. Stephen Phinney and Dr. Jeff Volek’s approach will be different during the weight loss phase than during weight maintenance. As well, some low carb diets target protein and others target fat. Some promote unrestricted saturated fat in all forms, including bacon and cream, while others don’t. For example Dr. Fung’s approach does not limit eggs, cream and bacon and for weight loss, Dr. Westman’s approach does.
Low Carb Food Categories (based on a diagram from Dr. Ted Naiman)
In my practice, I focus on whole, unprocessed foods that are naturally low in carbohydrates and that come from a wide range of food categories, including non-starchy vegetables, plant fats, low sugar fruit, meat fish poultry and seafood, and animal fat.
I encourage people to eat the fat naturally found in the flesh of animal protein, but to trim meat of extraneous visible fat.
If people enjoy eating bacon from time to time, I’d encourage them to obtain one that is naturally cured and smoked and to eat it on occasion rather than daily.
From my perspective, it makes no sense for someone seeking weight loss to ‘add fat’ to foods for the sake of adding fat (e.g. ‘bulletproof’ coffee or ‘fat bombs’). If people want to have a bit of cream in their coffee or a touch of butter on their asparagus there’s no reason why not, as there is nothing intrinsically ‘dangerous’ about fat, even saturated fat (more on this in upcoming blogs!). However from my perspective, adding coconut oil and butter to coffee for the sake of “adding fat” makes no sense, even for those following a “ketogenic” diet. I encourage folks to pursue health, not ketones.
Note: There are very few physiological conditions that require very high fat intake such as specialized diets for epilepsy or seizure disorder or for specific types of cancer as an adjunct to treatment.
To address the misconceptions that a low carb or ketogenic diet is restrictive, imbalanced or in any way unsustainable, below are some photos of types of foods that I prepare and eat. Everybody has different types of foods that they enjoy, these are simply some of mine.
Keep in mind that in some photos, only the main course is shown not the large salad or side of cooked vegetables which almost always accompanies it. As well, many of the servings shown are of one of my young adult son’s plates, rather than mine (my serving sizes are different because my nutritional needs are different).
I am showing these photos to dispel the myth that eating a low carb diet is in any way “restrictive”, “imbalanced” or “not sustainable” and I hope they give you some ideas of the wide range of whole, delicious food that is available to be enjoyed when pursuing a low carb or keto lifestyle.
Shakshuka is weekend breakfast or brunch food, that I usually serve with a huge mixed green salad or cucumber and tomato salad.
Shakshuka for threeindividual serving of shakshuka
Another favourite on the weekend is Vanilla Bean Pancakes – which one of my young adult sons loves to smother in butter (too much butter for me!). That day, he had poached eggs on the side and a mixed green salad with pumpkin seeds and pomegranate arils on top, drizzled with cold-pressed olive oil.
One of my young adult son’s helping of Vanilla Bean pancakes and buttera close up of a Vanilla Bean pancake
This is one of my favourite breakfast or brunch salads:
Greek salad with mini marzano tomatoes, mini cukes, goat feta and kalamata olives with a drizzle of cold pressed olive oil, rubbed oregano and fresh lemon
Below is a totally decadent plate that I made this past Sunday from the other half of my rib steak that I cooked the night previously (way too much meat for me!!), that I sliced thinly and warmed with stir fried asparagus, roasted peppers (also from the previous night’s supper) and a few thin slices of melted brie on top. This was shared between two for brunch, and served along with a mixed green salad.
Brunch plate made with leftover steak, roasted peppers and asparagus, with melted brieBBQ’d burgers on a lettuce bun with grilled asparagus and a small side salad
Here’s how we eat “burgers” for dinner.
…and a close up of one of my son’s plates:
BBQ’d cheese burgers served on a lettuce bun
The burgers look bigger than they are, because they are served on a smaller diameter “lunch” plate, rather than a “dinner” plate. The burgers in this case were served with a large mixed green salad, with a few raspberries on top, a light sprinkling of roasted pumpkin seeds along with a drizzle of cold- pressed olive oil.
Below is one of my son’s plates of lamb souvlaki that I also made this past weekend, and served with homemade tzatiki, grilled asparagus and a small Greek salad on the side (my plate had less lamb and a smaller piece of feta and more asparagus – again, because my nutritional needs are different).
a son’s plate of lamb souvlaki with homemade tzatiki, grilled asparagus and small Greek salad
…and finally, this is a popular weekend Middle Eastern style brunch in warmer weather:
Homemade Maza for weekend brunch
Want “noodles”? Sure! See the “Recipe” tab for details.
low carb broad noodles
These can be cut (or bought pre-cut) in thinner slices like linguine and are wonderful topped with spaghetti sauce or pesto.
Eating low carb or keto need not involve this much cooking, either! One can make a simple piece of grilled, broiled or pan-fried fish or chicken, some cooked veggies in the microwave and/or a salad. I happen to enjoy cooking (and my sons enjoy eating!) so this is something I do to relax.
Whether the meals are simple with little cooking required or elaborate, there is nothing “restrictive” about eating low carb.
As for eating this way being “imbalanced”, someone would be hard-pressed to demonstrate that eating this way doesn’t provide adequate nutrients. There is cheese and other dairy, nuts, seeds, fruit, vegetables and a wide variety of meat, fish and poultry. The diet provides all essential amino acids, essential fatty acids and ample vitamin and minerals – certainly no less than the average Canadian diet provides!
As for eating this way being “not sustainable”, what is not sustainable about eating fresh, healthy, whole foods that can be eaten with a minimum of preparation or as elaborate as one’s imagination allows?
I know of people that have been eating this way for 15 or 20 years and I personally have been eating this way for just over a year now (see “A Dietitian’s Journey” tab) and there is nothing that I miss!
If I want something, I make it!
When it was blustery out, I wanted to make “Shepherd’s Pie”, so I made it, substituting cut up green and waxed beans with cubed carrot for the usual vegetable medley and topping with mashed cauliflower, instead of mashed potato.
low carb Shepherd’s Pie
Another time, I felt like lasagna so I made it with thinly sliced Chinese eggplant in place of pasta and it was delicious!
low carb lasagna
Oh and bread? No worries!
One of my son’s wanted a “grilled cheese” and so I made him this.
low carb grilled cheese
What if you want a kaiser bun for a sandwich, or a hamburger bun? No problem (see “Recipes” tab).
Low carb kaiser bun sandwichfreshly baked low carb hamburger buns
Crispy, yeasty pizza? Sure! Yes, the full recipe is available on the “Recipe” tab.
crispy, yeast pizza
While “keto pizza” is higher fat than I personally would ordinarily eat as an ‘everyday food’ (because I follow the third type of low carb style of eating and am still in the weight loss phase), if I really wanted a pizza, I’d make it! I can plan for it ahead of time or adjust my eating for a little while afterwards to compensate, but eating this way does NOT involve food restriction. It does require making some adaptation to prepare it differently, but there are plenty of websites geared to supporting those following a low carb lifestyle that have wonderful recipes.
I hope this post encouraged you that following a low carb or keto lifestyle is entirely doable, provides adequate essential nutrients from a wide variety of food categories. It is certainly not restrictive or nutritionally imbalanced and can be sustained for as long as someone desires to eat this way.
Want to get started, but need some help designing a Meal Plan just for you? I’d be glad to help.
Whether you live here in the Lower Mainland or live far away, the identical services and prices are available in-person or via Distance Consultation.
Have questions?
Please send me a note using the “Contact Me” form and I’ll reply as soon as possible.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
A year ago, I found out from a fellow Dietitian that a recently published article in the Journal of the American Medical Association revealed that the sugar industry had secretly funded a group of renowned Harvard researchers to write an influential series of articles which downplayed, discredited or outright ignored research known at the time, and which demonstrated that sugar was a contributor to heart disease.
I read the article and was stunned at its significance.
As I am in the midst of a new series of articles on the role of saturated fat and polyunsaturated fat in health and disease, I felt it’s important that people understand the sugar’s industry involvement in potentially skewing of the scientific evidence at the very time that the original 1977 low-fat high carb Dietary Guidelines were being formulated and so I researched further and wrote this article.
Two of the prominent Harvard researchers that were paid by the sugar industry and who wrote articles dismissing that sugar was a significant contributor to heart disease and implicating saturated fat as the cause were the late Dr. Fredrick Stare, chair of Harvard’s School of Public Health Nutrition Department and the late Dr. D. Mark Hegsted, a professor in the same department [2].
POST PUBLICATION NOTE (March 12 2018): Dr. Hegsted, one of the 3 Harvard researchers paid by the sugar industry to write these review articles was directly involved in developing the 1977 US Dietary Guidelines [6].
[Note: April 1, 2021: see this article for documentation.]
A commentary in the Journal of Accountability in Research [4] summarized the significance of those articles as follows;
“Researchers were paid handsomely to critique studies that found sucrose [sugar] makes an inordinate contribution to fat metabolism and heart disease leaving only the theory that dietary fat and cholesterol was the primary contributor.”
In the mid-1960’s, the Sugar Research Foundation (which is the predecessor to the Sugar Association) wanted to counter research that had been published at the time which suggested that sugar was a more important cause of atherosclerosis than dietary fat. The Sugar Research Foundation invited Dr. Stare of Harvard’s School of Public Health Nutrition Department to join its scientific advisory board and then approved $6,500 in funds ($50,000 in 2016 dollars) to support a review article that would respond to the research showing the danger of sucrose[2]. Letters exchanged between the parties were brought to light in the November 2016 article published by Kearns et al [1] maintained that the Sugar Research Foundation tasked the researchers with preparing ”a review article of the several papers which find some special metabolic peril in sucrose [sugar] and, in particular, fructose [3].”
This would seem akin to the tobacco industry having secretly funded articles demonstrating that something other than smoking was responsible for lung cancer.
In August 1967 the New England Journal of Medicine published the first review article written by Drs. Stare, Hegsted and McGandy titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which stated;
”Since diets low in fat and high in sugar are rarely taken, we conclude that the practical significance of differences in dietary carbohydrate is minimal in comparison to those related to dietary fat and cholesterol”
The report concluded;
”the major evidence today suggests only one avenue by which diet may affect the development and progression of atherosclerosis. This is by influencing the levels of serum lipids [fats], especially serum cholesterol.”
The Harvard researchers went on to say;
”there can be no doubt that levels of serum cholesterol can be substantially modified by manipulation of the fat and cholesterol of the diet.”
The Harvard researchers concluded;
“on the basis of epidemiological, experimental and clinical evidence, that a lowering of the proportion of dietary saturated fatty acids, increasing the proportion of polyunsaturated acids and reducing the level of dietary cholesterol are the dietary changes most likely to be of benefit.”
Stare, Hegsted and McGandy did not disclose that they were paid by the Sugar Research Foundation for the two-part review [4].
In response to Kearns et al article in the Journal of the American Medical Association in November 2016 [1], the Sugar Association responded [5] by stating that it;
”should have exercised greater transparency in all of its research activities, however, when the studies in question were published funding disclosures and transparency standards were not the norm they are today.” [5]
Some final thoughts…
The reviews written by these influential Harvard School of Public Health Nutrition Department researchers and paid for by the sugar industry have the appearance of being a deliberate manipulation of the perception of the scientific evidence known at the time.
Whether deliberate or inadvertent, the fact that such sponsorship occurred at the very period in time when the Dietary Guidelines were under revision to emphasize that saturated fat intake must be reduced and carbohydrate consumption must be increased cannot be understated — a move which certainly benefited the sugar industry.
POST PUBLICATION NOTE (March 12 2018): Discovered after publication of this article, one of the three Harvard researchers funded by the sugar industry, Dr. D.M Hegsted was one of the scientists that worked on the 1977 US Dietary Guidelines[6].
[Note: April 2, 2021: See this article for documentation.]
How has this turned out for us?
For the last 40 years, Americans and Canadians have diligently eaten more carbohydrate (including foods containing sucrose and fructose) and more polyunsaturated fats (especially soybean and canola oil) just as the Harvard researchers paid for by the sugar industry recommended — and to what end?
Obesity rates have gone from ~10% in the 1950’s and 60’s in both countries to 26.7% in Canada (2015) and ~34% in the US (2017) and Diabetes and high blood pressure (hypertension) rates have risen exponentially.
What’s going on?
Could it be that the shift to a diet abundant in omega-6 polyunsaturated fat (such as soyabean oil) and which supplies 45-65% of daily calories as carbohydrate created the ‘perfect storm‘ which inadvertently fueled the obesity and health epidemic we now see?
This will be the subject of future articles.
Have questions?
I provide both in-person and Distance Consultation services (via telephone or Skype) can help you learn a better and easier way to eat, while you achieve and maintain a healthy body weight long term.
Please send me a note using the “Contact Me” tab above and I will reply shortly.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Kearns C, Schmidt LA, Glantz SA, et al. Sugar Industry and Coronary Heart Disease Research: A Historical Analysis of Internal Industry Documents. JAMA Intern Med. 2016 Nov 01; 176(11):1680-1685.
Husten, L, How Sweet: Sugar Industry Made Fat the Villain, Cardio|Brief, 2016 Sept 13.
McGandy, RB, Hegsted DM, Stare,FJ. Dietary fats, carbohydrates and atherosclerotic vascular disease. New England Journal of Medicine. 1967 Aug 03; 277(5):242—47
Krimsky, S. Sugar Industry Science and Heart Disease, Accountability in Research. 2017 Oct 07; 24:2, 124-125.
This content of this post is based largely on a presentation titled “A New Hypothesis for Obesity” given by Dr. Michael Eades at the Low Carb Breckenridge Conference, Breckenridge Colorado, Sunday, March 4, 2018 with some details filled in from his website. Dr. Eades has been in full time practice of bariatric, nutritional and metabolic medicine since 1986 and is the Director of Medi-Stat Medical Clinics, a chain of ambulatory out-patient family care clinics in central Arkansas. I have added the Canadian data for the benefit of my readers. This article is Part 2 in the two-part series The Evolving Hypothesis of Obesity. Part 1, which lays the groundwork for this article can be read here.
In the 1970’s the Dietary Guidelines in both the US and Canada advised us to eat more grains, vegetables and fruit and to eat vegetable fat, instead of saturated fat in butter, eggs, whole milk and red meat.
The US has dutifully complied, as indicated by the following graph;
US per capita consumption of grains, vegetables and fruit and vegetable oils compared to red meat, whole milk, eggs, animal fats and butter – Nina Teicholtz via – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
Similar types of increases and decreases have been observed in Canada. According to Statistics Canada;
“In the past two decades, Canadians have shifted towards a diet which includes more fruits and vegetables, cereal products, and nuts and beans. During this time, poultry consumption has increased, while beef and pork consumption has continued to decline.”
In 2016, per capita consumption of beef, pork, lamb and veal in Canada was 47.7 kg (105 lbs) per person per year down from the 73.2 (161 lbs) per person per year it was in 1980. Egg consumption also dropped from 21.96 dozen per person per year in 1980 to 19.93 dozen in 2016. The last time it was measured nationally in 2009, total fresh vegetable intake (excluding potatoes) rose to a record 40.7 kg (89.7 lbs) per person and the amount of potatoes including as french fries was 27.9 kg (61.6) per person, making total vegetable consumption 68.6 kg (151 lbs) per person per year. Total fresh fruit consumption also rose to a record 39.3 kg per person.
The Canadian Canola Growers Association reported that in 2012, 600,000 tonnes of canola oil and soybean oil was consumed by Canadians either as grocery store items or food-service products, including margarine, cooking oil, mayonnaise and salad dressing. In the twelve months ending July 2012, 2.8 million tonnes of Canadian vegetable oil was exported to the US and China, accounting for another 2.4 million tonnes.
In 2012, Sean McPhee, President of the Vegetable Oil Industry of Canada said;
”The vegetable oil industry is an important part of Canada’s growing agri-food sector. The industry’s processing capacity in 2012 is nearly double the capacity of 2007, and it is anticipated that further expansion will increase capacity 50 per cent by 2015.”
As saturated fat intake has declined, carbohydrate intake has continued to increase from the mid-1960s onward.
Decrease in saturated fat consumption, increase in carbohydrate consumption (US data) – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
The Evolving Hypothesis of Obesity
The most significant change since 1976-1980 is that we are eating a great deal more linoleic acid found in soybean, canola and corn oil while simultaneouslyeating significantly less saturated fat and overall eating more calories.
Three factors together are thought to have produced the “perfect storm” which has resulted in the massive increase in obesity from 1980 until the present;
(1) the vilification of saturated fat
(2) the encouragement to eat industrially produced vegetable oils
(3) the increased consumption of refined carbohydrates.
Simply put, the evolving hypothesis of obesity states that in addition to the (a) increasing amount of carbohydrate in the diet since ~1980, things are made significantly worse by (b) large amounts of industrially-produced polyunsaturated fats which promote obesity simultaneous to the (c) decrease in naturally occurring saturated fats which protect against obesity.
Dr. Eades credits much of the mechanism for the linoleic hypothesis to Dr. Petro Dobromylskyj, whose is a doctor of veterinary medicine and who writes a technical blog called Hyperlipid which I referred to in order to fill out my understanding in writing this article.
The difference between how the body processes saturated fats versus polyunsaturated fats
To understand the mechanism, the only chemistry you need to understand is the difference between a saturated fat and an unsaturated fat.
Saturated fats are ones where all the carbons in the chain are saturated with hydrogen atoms and there are no double bonds in the middle of the fatty acid chain. Palmitic acid (a 16 carbon fat) is an example of a saturated fat – and is one that our body synthesizes.
Saturated fat – palmitic acid
When a saturated fat is broken down (called “beta oxidation”), 2 carbons are cleaved off at a time, until the fat is completely broken down.
Beta Oxidation of a Saturated Fat – e.g. palmitic acid
Glucose is processed anaerobically in the cytosol of cell, but fatty acids are metabolized inside organelles called mitochondria (the ‘powerhouse of the cell’). All our food (regardless what it is) is metabolized to a combination of FADH2 and NADH.
The NADH and FADH2 enter the Electron Transport Chain at different complexes. NADH enters at Complex I (CI), while FADH2 enters at Complex II (CII).
Saturated fat has a feedback mechanism called the Reverse Electron Transport which keeps the cell from taking in too much energy – – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
The lower the FADH2:NADH ratio is, the lower the local insulin resistance is and the higher the FADH2:NADH ratio, the higher the local insulin resistance.
A saturated fat generates a higher FADH2:NADH ratio, so saturated fat increases local insulin resistance which serves to keeps more carbs in the blood. A process called Reverse Electron Transport is initiated which results in the making of a signalling molecule known as a superoxide (SO) molecule. This signalling molecule tells the body to stop insulin signalling by inducing local insulin resistance. This way, the cell doesn’t take up too much energy.
An unsaturated fat, on the other hand (such as palmitoleic acid or linoleic acid) has double bonds in the middle of the chain which changes the way the body processes it.
Beta oxidation of Palmitoleic acid (unsaturated fatty acid)Polyunsaturated fat provide NO feedback mechanism (no Reverse Electron Transport) so there is nothing to keep the cell from taking in too much energy – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
When fat cells (and other cells) are metabolizing an unsaturated polyunsaturated fat (PUFA) such linleoic acid from soybean oil, corn oil or canola oil, they generates a lower FADH2:NADH ratio, so an unsaturated fat reduces local insulin resistance, which means they allow plenty of glucose into the cells along with the PUFA.
These n-6 PUFAs generate energy all the way through the Electron Transport Chain and the Reverse Electron Transport is not triggered, so NO (superoxide) signalling molecule to tell the body to stop insulin signalling (i.e. there is no localized insulin resistance caused). The cell just keeps taking in more and more energy even though it doesn’t need any more! This means the fat gets driven into the fat cells and is stored there, making it unavailable for use for energy.
Once fat gets stored in the fat cells, the body can only break it down when no more energy is coming in (such as when fasting), so the only way the body can get more energy is to eat more. The glucose is driven into the cells because of the decreased insulin resistance caused by the n-6 PUFAs oils, which results in glucose level falling. This causes the body to produce a strong signal to eat; in other words, it makes you hungry.
Along with carbohydrates, n-6 PUFA vegetable oils have increased dramatically in the typical American and Canadian diet since the 1970s and this mechanism explains why we’ve been getting fatter and fatter since then.
So much of our eating now takes place away from home, or with food made away from home, that much of the fat intake in the diet is n-6 PUFA vegetable oils that signal glucose to come right in along with them.
French Fries then and now
In the 1960’s French fries were fried in beef tallow (which is a saturated fat), and the stearic acid from the beef fat and the glucose (from the broken down potato) would be processed by the fat cell (adipocyte).
When the cell had enough energy, Reverse Electron Transport would kick in and create the signalling molecule (superoxide molecule), which would tell the body that it didn’t need any more energy. This would result in a decrease in hunger and an increase in energy expenditure.
Think of the superoxide molecule as a “bouncer” at a night club. When there are enough people inside, the “bouncer” simply won’t admit any more people until some leave.
When French fries are fried in polyunsaturated vegetables oil, the linoleoic acid (from the soybean oil or canola oil) and glucose (from the broken down potato) are processed by the fat cell. The problem is, that even when the cell has more than enough energy, Reverse Electron Transport does NOT kick in and there is NO signalling molecule (superoxide) produced. The body doesn’t get any message that it doesn’t need any more energy, and the person doesn’t get any signal that they’re full, so they just keep eating.
In the case of eating foods made with polyunsaturated fat, it would be like a night club that has no “bouncer”. Even when the club is jam-packed with people, everybody is admitted until there is no room to move!
The absence of a feedback mechanism in processing unsaturated polyunsaturated fats results in fat cells getting bigger and bigger – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
The mechanism simply explained
Fat cells (adipocytes) bind more insulin at a given level of exposure when eating polyunsaturated fats such as soybean oil, canola oil and corn oil, than fat cells bind when eating saturated fat such as butter, lard or beef tallow.
Since insulin has to bind to its receptor to work and more insulin is bound when eating a diet rich in polyunsaturated fats, significantly more glucose is taken up into a fat cell in a diet high in polyunsaturated fats than in a diet rich in saturated fat. That is, the cells are more sensitive to insulin when eating a diet rich in polyunsaturated fats than a diet rich in saturated fat, so polyunsaturated fats allow too much glucose in to cells.
When fat cells and other cells are metabolizing saturated fat they make a superoxide (SO) molecule as a result of Reverse Electron Transport which is used to stop insulin signalling. When fat cells and other cells are metabolizing polyunsaturated fats, there is NO Reverse Electron Transport, so they are unable to generate the superoxide molecule that is needed to stop insulin signalling. This is because there is too little FADH2 being delivered to ETF.
Saturated fats, such as Palmitic acid have a higher FADH2: NADH ratio and it is believed that this is what drives Reverse Electron Transport (RET).
The FADH2 to NADH Ratio (also called the F:N ration – different with saturated fats and unsaturated fats – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
Oleic acid, the monounsaturated fat found in olive oil drives Reverse Electron Transport (RET) somewhat, but to a lesser degree than a saturated fat.
Unsaturated polyunsaturated fats such as Linoleic acid (found in soybean oil, corn oil and canola oil) have too small a FADH2: NADH ratio which prevents it from initiating Reverse Electron Transport (RET). It is thought that because polyunsaturated fats have such a low FADH2: NADH ratio, they are treated by the body similarly to glucose.
There are two consequences to eating fats with this low FADH2: NADH ratio.
the fat cells (adipocytes) get over-stuffed with fat (because there is no “off switch”)
When these fat cells get over-full they are unable to keep the fat contained as they should, and as a result free fatty acids are released and eventually find their way into other places where fat is not supposed to be found, such as in the liver, pancreas, even muscle and bone cells. This is known as ectopic fat and the condition that results is called metabolic syndrome.
Summary
What happened after the 1950s and 1960s that caused overweight and obesity to suddenly explode in the 1970’s – and just keep rising?
The answer is the types of fat we started eating.
Even though we were eating the same total amount of fat as before, these new industrially-produced polyunsaturated fats (such as soybean oil, canola oil and corn oil) do NOT provide the feedback mechanism that natural fats (such as butter, lard and beef tallow) do, so there is nothing in these manufactured fats to signal us that we are “full”.
This is why we began eating 240 more calories per day in carbohydrates –because the polyunsaturated fat that accompanied the carbs don’t tell us we’ve had enough!
The (1) the vilification of saturated fat, the (2) encouragement to eat and our acceptance and adoption of industrially produced vegetable oils and the (3) increased consumption of refined carbohydrates created the “perfect storm” and which taken together, certainly provide a reasonable mechanism with explains the massive increase in obesity from 1980 until the present.
Final Thoughts…
The different way the body processes natural saturated fats (such as butter, lard and beef tallow) versus the way it processes industrially-produced polyunsaturated fats (such as soybean oil, canola oil and corn oil) explains the mechanism by which the prevalence of obesity graph so closely mirrors the consumption of vegetable oil graph.
Trends in obesity among US Adults Aged 20-74 – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018Added fats and oils compared with trends in obesity among US Adults Aged 20-74 – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
Given that (1) total fat consumption has not changed since the 1960’s, only the type of fat we are eating has and (2) given that the body manufactures saturated fat in the form of palmitate, these naturally occurring saturated fats should not be thought of as “dangerous” or to underlie obesity.
As occurred late in the game with trans fats, it is time that these industrially-produced polyunsaturated fats be examined much more closely.
We ought to ask ourselves if we should even be eating oil from crops not thought of as fat-containing. If we squeeze an olive and fat comes out or we crush a nut and oil comes out, these are natural fats. Fats such as cold pressed olive oil, macadamia nut oil and walnut oil (to name a few) are natural sources of largely monounsaturated fats that are foods our ancestors (or other people’s ancestors) knew.
If “oil” needs to be produced under high pressure, high heat and with the use of solvents and deodorizers, is this even “food”? I think not.
Have questions?
Want to understand how to best nourish your body explained by someone who can make the science simple? Please feel free to send me a note using the “Contact Me” form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Reference
Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4, 2018 (NOTE: here is a similar talk given a Low Carb Down Under on August 11, 2018 and published on YouTube, called A New Hypothesis of Obesity.)
This content of much this post is based on a presentation titled “A New Hypothesis for Obesity” given by Dr. Michael Eades at the Low Carb Breckenridge Conference, Breckenridge Colorado, Sunday, March 4, 2018. Dr. Eades has been in full time practice of bariatric, nutritional and metabolic medicine since 1986 and is the Director of Medi-Stat Medical Clinics, a chain of ambulatory out-patient family care clinics in central Arkansas. I have added Canadian data and photos for Canadian readers. This article is Part 1 of two on The Evolving Hypothesis of Obesity.
The current ‘obesity epidemic’ is often understood in terms of the change in the percentage of obese people in the US or Canada from the early 1950’s, through the early 1970s until today. In Canada in the early 1960s the obesity rates were 10.2% (~8% of men and ~12% of women) and in the US, obesity rates at that time were 10.7%. From 2007 to 2009, obesity in Canada rose to 24.1% and in the US, rose even more to 34.4%.
In addition to statistics, another way to understand the obesity epidemic is through historical photos. Below is a sorority photo from Louisiana from the 1950s (one of the US States that currently has one of the highest rates of obesity).
Louisiana sorority, 1950s
What about Canada?
Here’s a photo of what people looked like in 1967, riding the subway in Toronto.
As can be seen in another photo (below) from a Toronto rush hour, young adults, middle aged adults and older people were very slim compared to today’s standards.
In the 1950’s, people in US as in Canada ate carbohydrates at each meal. They ate cereal or toast for breakfast and just about every household had a toaster. Lunch was often sandwiches, as there were no microwaves to heat food up in. Potatoes were a mainstay at dinner, sometimes pasta – yet the majority of young adults and adults were slim. Of course there were always some people that were overweight. Most elementary school classes had one ‘chubby’ kid, but when one looks around the classes of today or on public transit or in stores and supermarkets, most people are considerably heavier than people in the 1950’s and 1960’s.
What happened? What changed?
What caused overweight and obesity to all of a sudden explode in the 1970’s – and just keep rising?
A clue is in the macronutrient intake between 1971 and 2010.
Macronutrient Intake 1971-2010 – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
The graph on the left above shows macronutrients (protein, fat and carbohydrate) as a percentage of calories. After 1980, carbohydrate intake went up, fat intake went down and protein remained about the same.
As carbs intake went up and fat went down (protein intake stayed about the same), people began to gain weight. But what caused people to start eating more carbs?
The graph on the right above is much more telling as it shows the macronutrient intake in grams eaten per person per day. There are only two lines on the graph because the amount of fat and the amount of protein are superimposed over each other and appear as one line. The amount of fat (in grams) and the amount of protein (in grams) is approximately 75 g each however keep in mind that fat has 9 calories per gram and protein only has 4 calories per gram. The top line on the graph shows carbohydrate intake in grams and as can be seen around ~1976-1980 carbohydrate intake suddenly skyrocketed by ~ 240 calories per day.
What made people start eating 240 calories more per day in carbohydrate?
More on this in Part 2, but the clue is in the type of fat that people began to eat.
The graph below shows the change in the type of fat that people ate from 1970 to 2010. While the total amount of fat remained relatively constant from 1970 – 2010, there was a significant change in the type of fat that people ate. From 1970 onward, there is a huge increase in the consumption of polyunsaturated vegetable oils.
Added fats and oils – 1970-2010 – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
Breaking these vegetable oils down into specific types of oils, one can see that there is a huge increase in the consumption of soybean oil over this period.
Increase in soybean oil consumption 1949 – 1999 – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
Where does good old Canadian “canola oil” place?
Clinical and Metabolic Effects of Altering Omega-3 and Omega-6 Fatty Acids – Dr. Doug Mann MD, Professor of Neurology, University of North Carolina, February 21 2014
The graph at the top of the illustration below is the same graph as the one above and shows that soybean oil consumption reaches 12 kg per person per year. Looking at the graph below that one, canola oil is less than 1 kg per person per year.
It’s important to remember that the per person consumption of these oils is not only the fats that people buy and use at home, but include the oils used in the food that people eat at restaurants and in pre-made foods, including baked goods. Most oils sold as “vegetable oil” are soybean oil and it finds its way into things we’d never expect to find it in. Read labels more closely and you’ll find it everywhere. It’s in peanut butter and infant formula, most commercial salad dressings, crackers and baked goods, such as muffins. Its what your mayonnaise is made of (even if it says that its “olive oil mayonnaise”) because soybean oil can turn two ounces of olive oil into 500 ml bottle of ‘olive oil’ mayo or salad dressing. These vegetable oils are what potato chips and tortilla chips are fried in and it’s the fat in almost all commercial bread you eat – from burger buns to wraps. It’s everywhere!
While the total amount of fat in the diet hasn’t change over time (1970-2010), the type of fat being eaten is very different!We’re eating MUCH more vegetable oils just as the Dietary Guidelines in Canada and the US have encouraged us to do since the 1970s and at the same time, we’re eating less saturated fat from beef, pork, eggs, butter etc. As will be developed in the second part of this article, this increase in the consumption of vegetable oils and decrease in eating saturated fat has served as two sides of a dual-edged sword that has contributed to the obesity epidemic.
One of the reasons for the huge increase in the consumption of vegetable oils is the number of meals that are eaten away from home, as opposed to cooked at home. In the 1950’s and 1960’s people rarely ate out at restaurants unless there was a special occasion, or they were travelling away from home. Meals at home were cooked from scratch (there were very few ‘convenience foods’) and before the creation of vegetable shortening (Crisco®) people used lard (a saturated fat) in their pies and butter in their cakes. Butter (also a saturated fat) was the used on potatoes and as a spread on bread but with the rationing during World War II, margarine came into use – as did vegetable shortening, which was inadvertently created when extracting fats for the industrial production of soap.
Restaurants in the 1950s and 1960s used either beef tallow or lard in their deep fat fryers, but with the change in the Dietary Guidelines in the 1970s which told us ‘saturated fat was bad for our health’, these natural fats were replaced with industrially produced soybean oil and canola oil which are extracted under high heat and pressure, with the use of solvents, bleaches and deodorizers.
Note: you can squeeze a soybean all day long and you’re not going to get any ‘oil’ out of it – same with a corn kernel or canola (rapeseed). Gently pressing olives or nuts between one’s fingers will extract some oil so one can easily see that these are rich sources of fat. Soybeans, corn and canola require hours of industrial processing (heat, pressure and solvents) to extract ‘oil’. It has long been known that polyunsaturated omega-6 fats compete for binding sites with anti-inflammatory omega-3 fats (from fatty fish and flax seed) and as a result PUFA oils such as soybean oil, corn oil and canola oil promote inflammation in the body.
Approximately 1/2 of meals now are eaten away from home. These could be grabbing a coffee and a pastry at Starbucks® or Tim Hortons®, eating lunch at the work or school cafeteria or picking up ready-made sandwiches at a grocery store. Of course, this amount includes order in pizza and Chinese food, a quick bowl of Pho and any number of snacks bought away from home. The issue with these is the fat used in cooking these foods is now out of our control. Most often, soybean oil is used and behind that, canola.
Let’s take a closer look at these vegetable oils.
Linoleic content of canola oil, soybean oil compared to beef fat – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
As can be seen from this chart, canola oil is 32% polyunsaturated fatty acids (PUFAs), soybean oil is 61% polyunsaturated fatty acids and beef tallow is only 4% polyunsaturated fatty acids. The issue with oils (which will be presented in part 2 of this article) is that canola oil and soybean oil are very high in linoleic acid.
Reflective of the linoleic content of our diet is that the linoleic acid content of human body fat has also increased in a dramatic linear fashion over the last 50 years. The following graph was created by researcher Dr. Stephan Guyenet, PhD (neurobiology) based on various US studies, each of which is represented by an orange dot.
Linoleic Acid in US Body Fat 1961-2008 – Dr. Stephan Guyenet
This graph indicates that as we’ve been eating a lot more linoleic acid in our diet, this is showing up as an increasing amount of linoleic acid in our bodies. Why these polyunsaturated fatty acids (PUFAs) are being taken up so readily will become clear in Part 2 of this post, which will show the proposed mechanism.
Let’s look at the prevalence of obesity among US adults aged 20-74 from 1960-2010. In 1960-1962, obesity rates in the US were 10.7% which is very comparable to the Canadian obesity rates referred to above. From 2007 to 2009 the prevalence of obesity in the US was 34.4%, which is 10% higher than the obesity rate in Canada which was 24.1%.
Trends in obesity among US Adults Aged 20-74 – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
Now let’s compare the above graph on obesity rates to the increased use of vegetable oils over the same period.
Added fats and oils compared with trends in obesity among US Adults Aged 20-74 – Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4 2018
The parallel rise in the intake of polyunsaturated fats over the same period is striking, and while we know that “correlation is not causation” (i.e. two things being related does not mean that one causes the other) one must wonder if these two factors are related, and if so, how.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Reference
Dr. Michael Eades – A New Theory of Obesity, Low Carb Breckenridge, March 4, 2018 (NOTE: here is a similar talk given a Low Carb Down Under on August 11, 2018 and published on YouTube, called A New Hypothesis of Obesity.)
This article is Part 3 in a three-part series on Protein and is based largely on a lecture given by Dr. Donald Layman, PhD – Professor Emeritus from the University of Illinois (Nutrition Forum, June 23, 2013, Vancouver, British Columbia, Canada).
People understand it’s important for children to eat enough protein because they’re growing but adults and older adults need to eat enough protein each day, as well.
After youth have finished growing, they are at their maximum physical capacity between age 20 and 30 years old and after the age of 30 years old, adults begin to lose muscle mass at the rate of 1% per year [1].
We’ve come to expect that as people age, they will gain more fat, loose bone mass and that they’ll have decreased muscle strength and that in time, these will lead to difficulty getting around, a greater risk of falls and eventually to physical disability. We commonly see older people with spindly legs and bony arms and we think of this as ‘normal’, but as discussed in a recent “A Dietitian’s Journey” article, we’ve mixed up what is “common” with what is “normal”. When we look at seniors in Okinawa, Japan for example, we don’t see this. They continue to do manual jobs and practice martial arts well into their 80’s and 90’s. Aborigine elders in Australia also remain lean, fit and active as seniors. This is normal.
The physical deterioration that we associate with aging including weak bones (osteoporosis) and the loss of skeleton muscle mass (sarcopenia) don’t develop suddenly, but take place over an extended period of time – brought on by less than optimal practices in early middle age.
The Recommended Dietary Allowance (RDA) for protein is set at 0.8 g protein/kg per day and describes the minimum quantity of protein that needs to be eaten each day to prevent deficiency. Protein researchers propose that while sufficient to prevent deficiency, this amount is insufficient to promote optimal health as people age[2].
There have been several recent “position statements” issued by those that work with an aging population indicating that protein intake between 1.0 and 1.5 g protein / kg per day may provide optimal health benefits during aging [3, 4]. This seems at odds with the 2010 Dietary Guidelines Advisory Committee report [5] which states that ‘protein intake in the US is more than adequate’ and that ‘inadequate protein intake is rare’ [5]. These seemingly contradictory positions are largely due to a difference in terms of how protein adequacy is determined.
The RDA – more specifically the Estimated Average Requirement (EAR) is the minimum amount of protein intake required to prevent deficiency and is based on nitrogen balance studies (since nitrogen is the main component of the amino acids which make up proteins). The EAR is set at the amount of protein that allows the body to achieve nitrogen balance (protein making and protein breakdown is equal) and evaluates overall protein intake. Evaluation of optimal protein intake not only considers total amount of protein eaten, but alsoevaluates the metabolic roles of individual amino acids. While the EAR may be enough protein for healthy younger adults, higher intakes of specific Essential Amino Acids (ones the body can’t make, e.g. Leucine and Isoleucine and Valine) have been reported to improve body composition (muscle mass and increased strength) in older adults.
Another factor is that nitrogen balance studies look at the total amount of protein eaten in a day but don’t look at the amount of protein eaten at each meal [6,7] nor the role of the Essential Amino Acid Leucine which is required to be present for protein synthesis to begin(including synthesis of new protein for muscle and bone)[6]. Leucine is an indispensable amino acid in the making of all types of protein, but has a unique role in signaling the beginning of muscle protein synthesis. Much research has been done with large doses of free leucine, however a 2012 animal study[6] found that in small meals with limited protein intake (often the case for older adults), that there was a specific minimum amount of Leucine required to be be present, before protein synthesis took place. This “Leucine threshold” had to be met or exceeded before the body would even begin the energy-expensive process of making new proteins!
Typically, the average American eats only 10 g protein for breakfast, 15 g protein for lunch and has most of their daily protein at supper (65 g protein at supper) and since the minimum amount of Leucine that needs to be present in a meal (i.e. “Leucine Threshold”) is not enough at breakfast and lunch with this pattern of protein intake, protein synthesis is only triggered after the evening meal. As elaborated on below, it is recommended that this change.
A 2013 study of muscle protein synthesis in adults in their late 30’s found that when the amount of protein is distributed evenly throughout the day (30 g protein at breakfast, lunch and supper) that significantly more muscle protein was made. Of importance, the (a) making of new protein and (b) the threshold at which protein will be triggered to be made differ with age – with older people needing a higher intake of protein and specifically the amino acid Leucine, than younger adults [8]. This reduced muscle protein synthesis has been called “anabolic resistance” (anabolic means to ‘build’) and studies have shown that this “anabolic resistance” can be overcome with meals containing higher amounts of Essential Amino Acids and appears to be related to the Leucine content of the meal [8]. These findings led to Dietary Recommendations for older adults that emphasize a minimum of 20 g of protein per meal containing more than 2.3 g Leucine to optimize the building of new muscle protein [4].
Final Thoughts…
It is not only growing children and youth that need to eat adequate protein daily, but older adults as well. In many Indigenous cultures, the Elders eat first and eat the best of the animal proteins – which may factor in to the preservation of bone and muscle mass we see in many of these cultures.
The average protein intake for men >20 years old in the US is ~98 g per day and for women it is 68 g per day which may be adequate in total for healthy young adults, but is considered imbalanced in terms of distribution, as a minimum amount of Leucine is required for protein synthesis (specific amount in humans has not yet be determined). Dr. Layton recommends that until further research is conducted and the optimal amount of Leucine is determined that young adults and middle aged adults distribute their protein evening throughout the day with ~25 g (women) -30 g (men) of animal-based protein at each meal. The reason high biological value proteins from animal sources (meal, poultry, fish, egg, dairy) are recommended is because these are high in Leucine (rather than having only 10 g protein for breakfast, 15 g protein for lunch and 65 g protein at supper).
The recommendations above for older adults to eat 1.0 – 1.5 g protein / kg per day distributed evening over three meals which would be on average ~30-40g of animal-based protein at each meal to provide for optimal muscle protein synthesis, preventing sarcopenia – the muscle loss we’ve come to see as ‘normal’ in aging.
How much is too much protein?
According to Dr. Layman, the Upper Limit of Protein according to the Recommended Daily Allowance for Protein is set at ~ 2.5 g protein / kg per day which would put the maximum amount for most adult men at ~200 g protein per day.
Recommended Daily Allowance (RDA) for Protein [slide from Dr. Donald Layman, PhD – The Evolving Role of Dietary Protein in Adult Health]Have questions?
Need help determining how much protein you should optimally be eating at each meal and from what sources? Please send me a note using the “Contact Me” form and I will reply as soon as possible.
Keller K, Engelhardt M. Strength and muscle mass loss with aging process. Age and strength loss. Muscles, Ligaments and Tendons Journal. 2013;3(4):346-350.
Volpi E, Campbell WW, Dwyer JT, et al. Is the optimal level of protein intake for older adults greater than the recommended dietary allowance? J Gerontol A Biol Sci Med Sci. 2013 Jun;68(6):677-81
Fielding RA, Vellas B, Evans WJ, Bhasin S, et al, Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011 May;12(4):249-56
Bauer J1, Biolo G, Cederholm T, Cesari M, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013 Aug;14(8):542-59
U.S. Department of Agriculture and U.S. Department of Health and Human Services, Dietary Guidelines for Americans, 2010. 7th Edition, Washington, DC.
Norton LE, Wilson GJ, Layman DK, et al. Leucine content of dietary proteins is a determinant of postprandial skeletal muscle protein synthesis in adult rats. Nutr Metab (Lond). 2012 Jul 20;9(1):67
Mamerow MM, Mettler JA, English KL, et al. Dietary Protein Distribution Positively Influences 24-h Muscle Protein Synthesis in Healthy Adults. The Journal of Nutrition. 2014;144(6):876-880.
Layman DK, Anthony TG, Rasmussen BB, et al. Defining meal requirements for protein to optimize metabolic roles of amino acids, The American Journal of Clinical Nutrition, Volume 101, Issue 6, 1 June 2015, Pages 1330S—1338S
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.





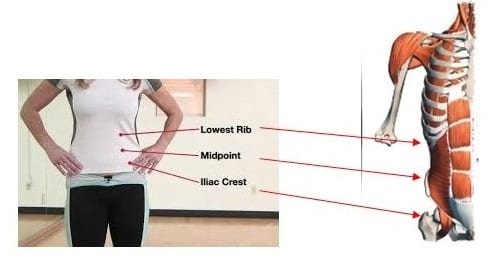
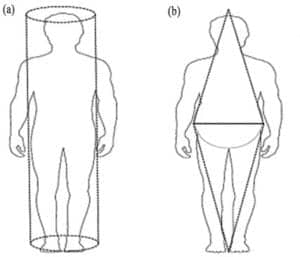

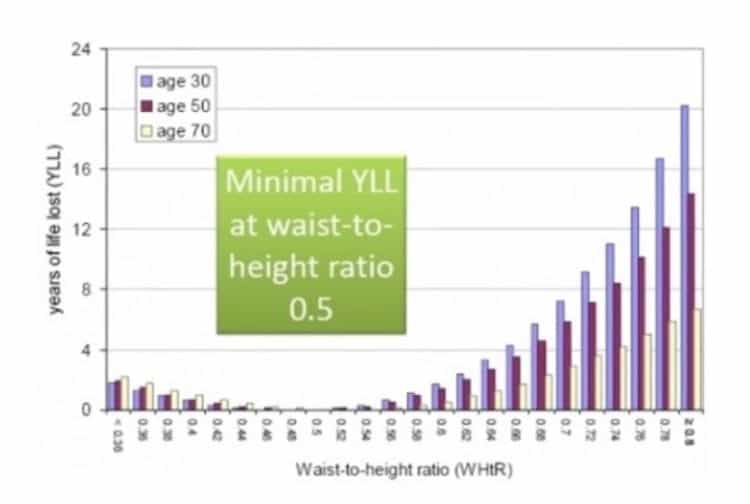

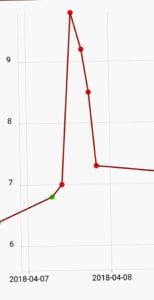 As mentioned in the
As mentioned in the 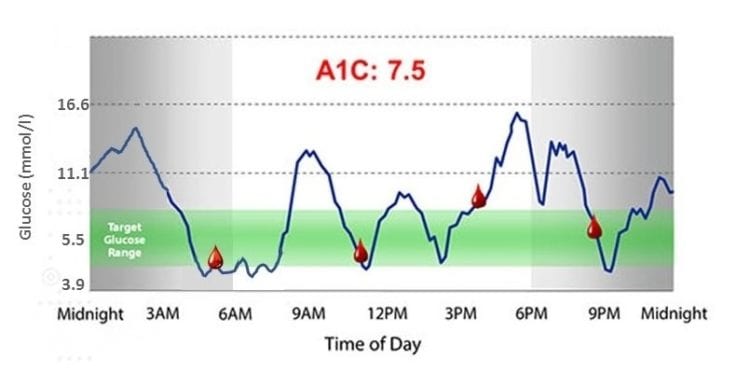


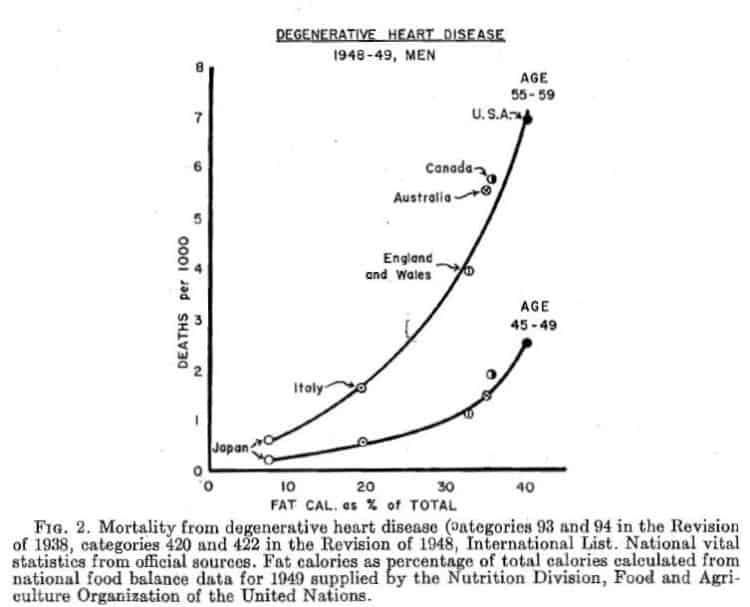
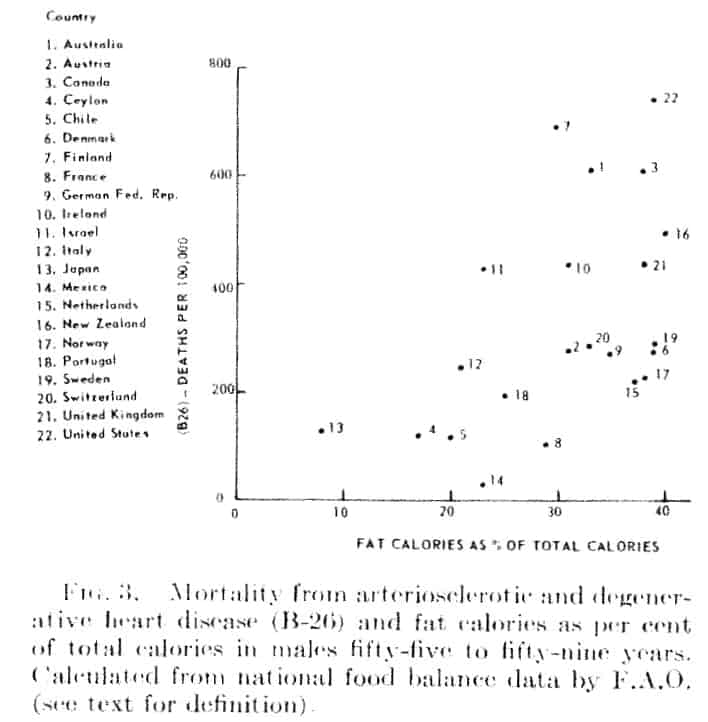
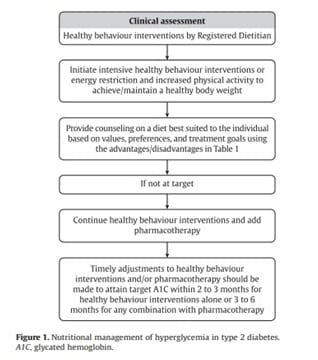
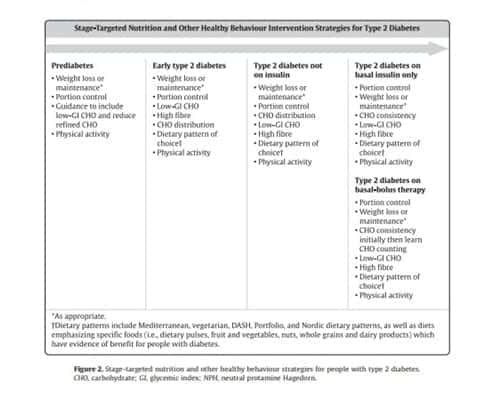

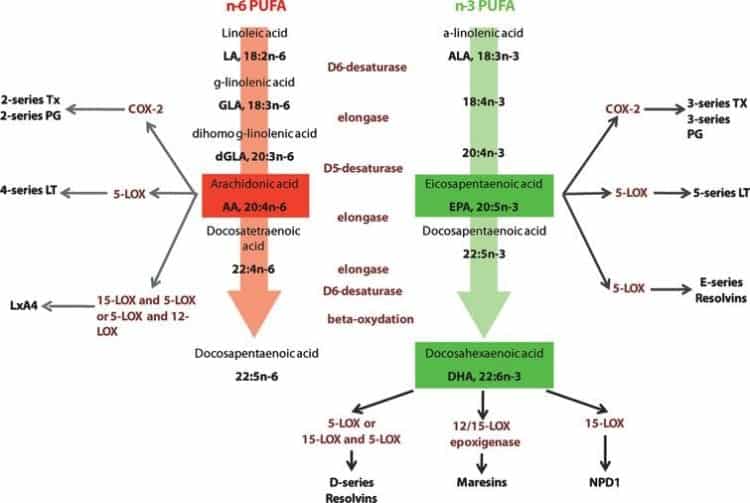



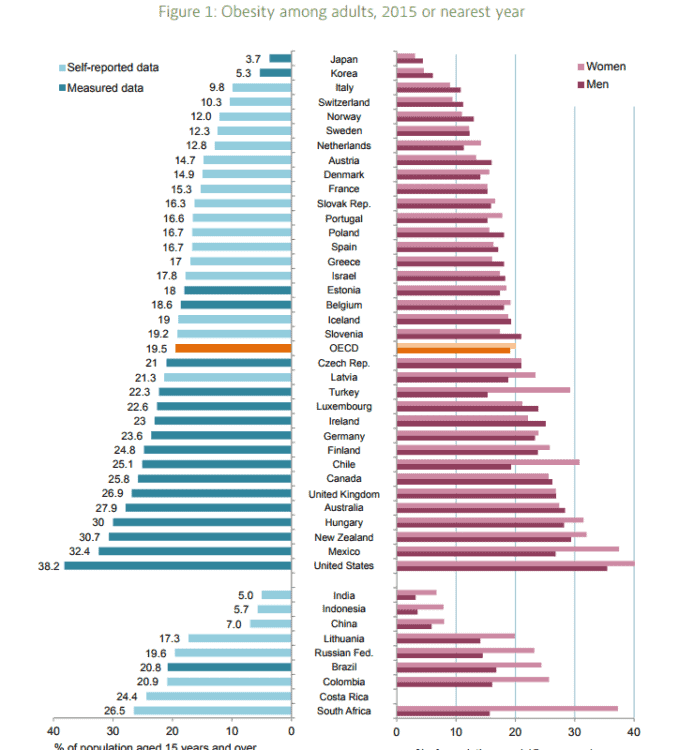


















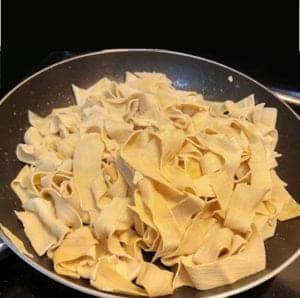






 In August 1967 the New England Journal of Medicine published the first review article written by Drs. Stare, Hegsted and McGandy titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which stated;
In August 1967 the New England Journal of Medicine published the first review article written by Drs. Stare, Hegsted and McGandy titled ”Dietary fats, carbohydrates and atherosclerotic vascular disease”[3] which stated;