This post contains a one page downloadable printout that you can bring to your doctor or other healthcare professional which summarizes the American Diabetes Association’s new Consensus Report of April 18, 2019 regarding the use of a low carbohydrate eating pattern of 26-45% of total daily calories as carbohydrate and the use of a very low carbohydrate (ketogenic) eating pattern of 20-50 g carbohydrate per day for the management of pre-diabetes, Type 1 or Type 2 Diabetes in adults [1].
This new downloadable printout is available by clicking here.
DISCLAIMER: This printout is intended for information purposes only and is not affiliated with the American Diabetes Association in any way.
The previous printout from January 2019 (available by clicking here ) was based on two earlier reports;
(1) the ADA’s October 2018 joint Position Statement with the European Association for the Study of Diabetes (EASD) which approved use of a low carbohydrate diet of <130 g of carbohydrate/day (<26% of daily calories as carbohydrate) as Medical Nutrition Therapy (MNT) for adults with Type 2 Diabetes [2]
and
(2) the ADA’s recently released 2019 Standards of Medical Care in Diabetes – Lifestyle Management [3] which includes the use of low carbohydrate diets as Nutrition Therapy and which reflects the organization’s emphasizes on a patient-centered, individualized approach
If you have been diagnosed as pre-diabetic or as having Type 2 Diabetes (T2D) and would like some professional support to put the symptoms into remission by following a low carbohydrate or very low carbohydrate eating pattern, I can help.
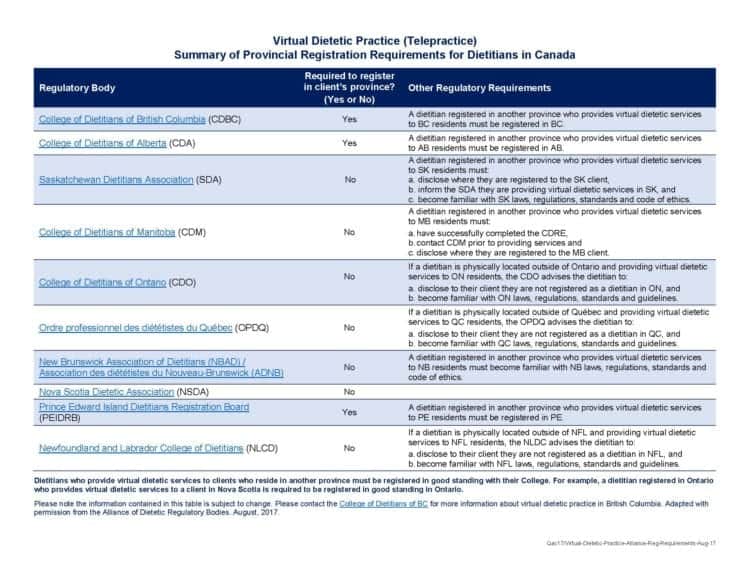
I can provide Registered Dietitian services to those in any province in Canada (except PEI), and for those in the US, I can provide you with nutrition education to help you know how to eat according to a low carb eating pattern.
You can learn more about my services under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
To your good health!
Joy
Here are the links to 4 articles that I wrote about the new ADA Consensus Report:
Evert, AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014
Davies M.J., D’Alessio D.A., Fradkin J., et al, Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), Diabetes Care, October 2018, https://doi.org/10.2337/dci18-0033
American Diabetes Association, Lifestyle Management Standards of Medical Care in Diabetes — 2019. Available at: http://care.diabetesjournals.org/content/42/Supplement_1. Accessed: Dec. 17, 2018.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This 4 minute introduction to the topic of circadian rhythms (which is the 24 hour clock on which our body runs) and about when research indicates it’s best to eat and not to eat, including intermittent fasting.
This is the 11th entry in the series titled “Making Health a Habit”, which can be found here.
Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information about lowering insulin resistance, keeping blood sugar at a healthy level, or maintaining (or building) muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet. Making Health a Habit are short videos (< 5 minutes in length) or short blogs on health-related topics and are quite different than Science Made Simple articles which are longer, research-focused articles.
Feel free to leave your thoughts on social media after watching the video.
If you’d like to know how I can help you set up the best time for you to eat and not eat in order to achieve your health and nutrition goals, please let me know.
You can learn more about my services and their costs above under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This is the 10th entry in the series titled “Making Health a Habit”, which can be found here.
Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information that can be applied to almost anyone for lowering insulin resistance, keeping blood sugar at a healthy level, or maintaining (or building) muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet.Making Health a Habit are short videos (< 5 minutes in length) or short blogs on health-related topics and are quite different than Science Made Simple articles which are longer, research-focused articles.
This very short video (2 1/2 minutes long) has a few thoughts on the fact that none of us are promised “tomorrow” and how living in that light can impact our lives for the better.
Feel free to leave your thoughts on social media after watching the video.
If you’d like to know how I can help you achieve your health and nutrition goals, please let me know.
You can learn more about my services and their costs above under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This short video are some reflections about a challenge I received on social media as to whether I was “an obese Dietitian” or “A Dietitian with obesity or a Dietitian that developed obesity”. What is the difference?
What does it mean to have “obesity in remission”?
In this short video I talk about the second topic first; why it is appropriate to talk about obesity as being “in remission”. In my next video, I’ll talk about whether I “was obese” or “did I have/develop obesity”, and what the difference is.
This is the 8th entry in the series titled “Making Health a Habit” , which can be found here.
Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information that can be applied to almost anyone for lowering insulin resistance, keeping blood sugar at a healthy level, or maintaining (or building) muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet. Making Health a Habit are short videos (< 5 minutes in length) or short blogs on health-related topics and are quite different than Science Made Simple articles which are longer, research-focused articles.
Feel free to leave your thoughts on social media after watching the video.
If you’d like to know how I can help you to get started eating healthier or beginning to address symptoms of obesity, or some of the disorders that often accompany it, please let me know.
You can learn more about my services and their costs above under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
In its recently published Consensus Report (April 18, 2019), the American Diabetes Association confirmed something that I have written about in several previous articles, including How Much Carbohydrate is Essential in the Diet and that is that the body has no essential need for dietary carbohydrate.
From the top of page 4 of the Consensus Report:
“The amount of carbohydrate intake required for optimal health in humans is unknown. Although the recommended dietary allowance for carbohydrate for adults without diabetes (19 years and older) is 130 g/day and is determined in part by the brain’s requirement for glucose, this energy requirement can be fulfilled by the body’s metabolic processes, which include glycogenolysis, gluconeogenesis (via metabolism of the glycerol component of fat or gluconeogenic amino acids in protein), and/or ketogenesis in the setting of very low dietary carbohydrate intake.”
Body can make all the glucose it needs for the brain
That is, the body can make all the glucose the brain needs from the glycogenolysis (which is the breakdown of glycogen to glucose), via gluconeogenesis (which is thegeneration of glucose from glycerol or glucogenic amino acids) and via ketogenesis (which is from ketones generated in a very low dietary carbohydrate [ketogenic] diet).
In short, dietary intake of carbohydrate is not essential. While there is no biological need to eat carbohydrate-based food, one certainly can and there are many good reasons to include some types of carbohydrate-containing food in the diet.
Because there is no essential need to eat carbohydrate because the body can make all the glucose it needs itself, the American Diabetes Association includes among its eating patterns both a low carbohydrate pattern (26-45% daily calories as carbohydrate) and a very low carbohydrate (ketogenic) eating pattern (20-50 g carbohydrate / day).
How much carbohydrate is a major consideration for those who are pre-diabetic or Diabetic because as the ADA stated in this new consensus report;
“Carbohydrate is a readily used source of energy and the primary dietary influence on postprandial blood glucose.
That is, it is the carbohydrate in a meal that is the biggest predictor of how high blood sugar will rise after a meal, and how quickly.
For those who want to improve their blood sugar levels (glycemia) the same report also makes it clear that;
“Reducing overall carbohydrate intake for individuals with diabetes has demonstrated the most evidence for improving glycemia* and may be applied in a variety of eating patterns that meet individual needs and preferences.”
For those adults with Type 2 Diabetes who are not meeting their blood sugar targets or who need to, or want to have their physician reduce their need for Diabetes medications, a low carbohydrate or very low carbohydrate (keto) eating pattern is a viable option;
“For select adults with type 2 diabetes not meeting glycemic targets or where reducing anti- glycemic medications is a priority, reducing overall carbohydrate intake with low or very low- carbohydrate eating plans is a viable approach.”
Remember, carbohydrate-based foods are not necessary for your brain because your body can make all the glucose it needs from the metabolic processes listed above. That’s not to say one has to avoid carbohydrate-based foods, but how much and how often can and is best determined based on people’s individual needs and glycemic response to carb-based foods.
Remember too as outlined in the article posted yesterday , that in the US a well-designed low carb or ketogenic diet prescribed to lower blood sugar need not have all the same foods or food groups as a diet based on The Dietary Guidelines for Americans because it is used as Medical Nutrition Therapy (i.e. is a therapeutic diet). While these are the guidelines for those with pre-Diabetes or Type 1 or Type 2 Diabetes in the US, in Canada individuals have the ability to choose a low carbohydrate lifestyle if that is their personal preference.
If you would like some professional support to begin eating this way or to continue eating this way, I can help. I provide Registered Dietitian services to those in any province in Canada (except PEI), and for those in the US, I can provide nutrition education to help you know how to eat according to a low carb eating pattern.
You can learn more about my services including individual hourly appointments and sessions as well as packages above under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
To your good health!
Joy
Here are the links to other articles that I wrote about the new ADA Consensus Report:
Evert, AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Introduction: Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information that can be applied to almost anyone for lowering insulin resistance, keeping blood sugar at a healthy level, maintaining a healthy body weight, or building muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet.Making Health a Habit are short videos (< 5 minutes) or short blogs on health-related topics and are quite different than Science Made Simple articles, which are longer, research-focused articles.
This is the 7th entry in the new series titled “Making Health a Habit”, which can be found here.
Part of successfully ‘making health a habit’ has to do with transitioning over to a maintenance diet once you’ve accomplished your goals, but how?
In this short (~3 minute) video, I talk about some of the factors that need to be considered in doing that.
If you are getting to that stage in your health journey and would like some help making the transition, I can help — and if you are just setting out, I’d be glad to help you get started with a meal plan designed for you, based on your needs and goals.
If you’d like to know more about my services, you can find out under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
To our good health!
Joy
P.S. Here is a picture of where I walk.
Como Lake, Coquitlam, British Columbia
Isn’t it beautiful and it’s minutes from my house, in the middle of an urban area! I encourage you to find a place near you to enjoy being active at. It makes it so pleasant and something to look forward to.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
In its recently published Consensus Report (April 18, 2019)[1] the American Diabetes Association emphasized that Medical Nutrition Therapy (MNT) is “fundamental in the overall Diabetes management plan” [2], but what exactly is Medical Nutrition Therapy?
According to the report, the National Academy of Medicine defines Medical Nutrition Therapy (MNT) as ‘the treatment of a disease or condition through the modification of nutrient or whole-food intake’ [1].
In contrast, The Dietary Guidelines for Americans (DGA) “provides advice for healthy Americans ages 2 years and over about food choices that promote health and prevent disease [3]. The Consensus Report says (pg. 2) that The Dietary Guidelines for Americans (DGA) 2015-2020 “provide a basis for healthy eating for all Americans and recommend that people consume a healthy eating pattern that accounts for all foods and beverages within an appropriate calorie level”, but for people with Diabetes;
“recommendations that differ from the DGA are highlighted in this report”.
That means that the eating patterns listed in the American Diabetes Association’s new Consensus Report knowingly differ from the Dietary Guidelines for Americans because they are Medical Nutrition Therapy used in the treatment of a disease (i.e. Diabetes).
The Consensus Report outlines several eating patterns that are effective to varying degrees for achieving different Diabetes-related management goals, including HbA1C reduction, weight loss, lowered blood pressure, improved lipids (higher HDL-c, lower LDL-c), lower triglycerides (TG), but says that low carb eating patterns show the most evidence for blood glucose control [1].
As outlined in the previous article, the Consensus Report includes among the choices of Medical Nutrition Therapy various eating patterns, including a low carbohydrate eating patternand very low carb (keto) eating pattern and the various eating patterns with their different potential benefits are summarized below [1];
Table 3 – Eating Patterns reviewed for this report [1]
Role of a Registered Dietitian and Healthcare Team in Providing Medical Nutrition Therapy
The Consensus Report highlights (pg. 2) that it is the role of a Registered Dietitian/ Nutritionist (RDN) to provide Medical Nutrition Therapy (MNT), but that other members of the healthcare team (physicians, nurses and pharmacists) can and should complement this with evidence-based guidance (pg. 2);
“To complement diabetes nutrition therapy, members of the health care team can and should provide evidence-based guidance that allows people with diabetes to make healthy food choices that meet their individual needs and optimize their overall health.”
The Consensus Report specifies that the essential components of Medical Nutrition Therapy are;
“assessment, nutrition diagnosis, interventions (e.g., education and counseling), and monitoring with ongoing follow-up to support long-term lifestyle changes, evaluate outcomes, and modify interventions as needed.”
…and that the goals of Medical Nutrition Therapy (from Table 1 [1]) are;
“To promote and support healthful eating patterns, emphasizing a variety of nutrient-dense foods in appropriate portion sizes, in order to improve overall health and specifically to:
â—‹ Improve A1C, blood pressure, and cholesterol levels (goals differ for individuals based on age, duration of diabetes, health history, and other present health conditions. â—‹ Achieve and maintain body weight goals â—‹ Delay or prevent complications of diabetes
To address individual nutrition needs based on personal and cultural preferences, health literacy and numeracy, access to healthful food choices, willingness and ability to make behavioral changes, as well as barriers to change
To maintain the pleasure of eating by providing positive messages about food choices, while limiting food choices only when indicated by scientific evidence
To provide the individual with diabetes with practical tools for day-to-day meal planning
The Consensus Report also states that the Registered Dietitian/Nutritionists (RDN) is the preferred member of the health care team to provide diabetes MNT and to lead an inter-professional team;
“The unique academic preparation, training, skills, and expertise make the RDN the preferred member of the health care team to provide diabetes MNT and leadership in inter-professional team-based nutrition and diabetes care.”
…but implied in this is that the whole healthcare team needs to work in concert together to choose and customize an eating pattern to the individual’s metabolic needs and personal preferences.
Remember, if you have pre-diabetes or Diabetes (Type 1 or Type 2) and are following any of the eating patterns outlined as Medical Nutrition Therapy (including a low carb or very low carb (ketogenic) eating pattern, then it is understood that these will not be like the food groups and portions of the “food pyramid” of The Dietary Guidelines of Americans because they are therapeutic diets for the treatment of a disease.
If you have been diagnosed as pre-diabetic or as having Type 2 Diabetes (T2D) and would like some professional support to work on reversing the symptoms through a low carbohydrate or very low carbohydrate eating pattern, I can help. I don’t believe there is a “one-sized-fits-all” approach to either of these and will work within you needs to design an individual plan just for you.
You can learn more about my services including individual hourly appointments and sessions as well as packages above under the Services tab or in the Shop.
If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
To your good health!
Joy
Here are the links to other articles that I wrote about the new ADA Consensus Report:
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Evert, AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014
Introduction: Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information that can be applied to almost anyone for lowering insulin resistance, keeping blood sugar at a healthy level, maintaining a healthy body weight, or building muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet, or may simply be my opinion on different matters related to a low carb or ketogenic diet. Making Health a Habit are short videos (< 5 minutes) or short blogs on health-related topics and are quite different than Science Made Simple articles, which are longer, research-focused articles.
This is the 6th entry in the new series titled “Making Health a Habit”, which can be found here.
The idea for this short video (~4 minutes) came from a lively discussion that occurred on social media yesterday about which is more important to change first in achieving one’s health and weight loss goals; how we eat or exercise.
The person who initiated the discussion said they believed without a doubt that exercise was the more important of the two and many people contributed to what they felt was the most important from their experience and why.
In this short video I summarize what was said in that interchange, as well as my own thoughts on the subject.
If you’d like to know how I can help you to get started eating healthier or incorporating activity into your day, please let me know.
If you’d like to know more about my services, you can find out under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
On April 18, 2019, the American Diabetes Association published a new Consensus Report which not only includes the use of a low carbohydrate eating pattern of 26-45% of total daily calories as carbohydrate, but in this report also includes the use of a very low carbohydrate (ketogenic) eating pattern of 20-50 g carbs per day.
The report is clear that there is no “one-size-fits-all” eating pattern for the prevention or management of diabetes, and that it unrealistic to expect that there should be just one eating pattern for everyone; especially given the wide variety of people affected by diabetes and pre-diabetes, including their varied cultural backgrounds, personal preferences, co-occurring conditions and the variety of socio-economic backgrounds from which they come.
The new report underlines several eating patterns that are effective to varying degrees for achieving different goals, with potential benefits including HbA1C reduction, weight loss, lowered blood pressure, improved lipids (higher HDL-c, lower LDL-c), lower triglycerides (TG), but says clearly that low carb eating patterns show the most evidence for blood glucose control;
“Reducing overall carbohydrate intake for individuals with diabetes has demonstrated the most evidence for improving glycemia (blood sugar) and may be applied in a variety of eating patterns that meet individual needs and preferences.”
The new Consensus Report includes low carb eating patterns and very low carb (keto) eating patterns among the choices of eating patterns for those with pre-diabetes as well as adults with Type 1 or Type 2 Diabetes.
The various eating patterns with their different potential benefits are summarized in Table 3, below;
Table 3 – Eating Patterns reviewed for this report [1]
The report also indicates that for adults with Type 2 Diabetes not meeting their blood sugar targets, or where there is a need to lower anti-glycemic medications that lower blood sugar, that
“reducing overall carbohydrate intake with low- or very low- carbohydrate eating plans is a viable approach.”
If you have been recently diagnosed as pre-diabetic or as having Type 2 Diabetes (T2D) and would like support to reverse the symptoms through a low carbohydrate or very low carbohydrate eating pattern, then I can help. I also don’t believe there is a “one-sized-fits-all” approach to either of these and will work within you needs to design an individual plan just for you.
You can learn more about my services including individual hourly appointments and sessions as well as packages above under the Services tab or in the Shop.
If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
To your good health!
Joy
Here are the links to other articles that I wrote about the new ADA Consensus Report:
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Reference
Evert, AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014
Introduction: Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information that can be applied to almost anyone for lowering insulin resistance, keeping blood sugar at a healthy level, maintaining a healthy body weight, or building muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet. Making Health a Habit are short videos (< 5 minutes) or short blogs on health-related topics and are quite different than Science Made Simple articles, which are longer, research-focused articles.
This is the 5th entry in the new series titled “Making Health a Habit”, which can be found here.
In making health a habit, how we ‘talk’ to ourselves makes all the difference —especially during the first 9 – 12 weeks that it is becoming a habit. How do we make excuses?
In this short video (<4 minutes) I share my own struggles with making excuses for being active, simply because I have years of practice at making excuses.
For health to be a habit, I need to “talk” to myself differently.
If you’d like to know how I can help you to get started eating healthier or being more active, please let me know.
You can learn more about my services and their costs above under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Introduction: Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information that can be applied to almost anyone for lowering insulin resistance, keeping blood sugar at a healthy level, maintaining a healthy body weight, or building muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet.Making Health a Habit are short videos (< 5 minutes) or short blogs on health-related topics and are quite different than Science Made Simple articles, which are longer, research-focused articles.
This is the 4th entry in the new series titled “Making Health a Habit”, which can be found here.
This photo was liked 370 times on Twitter and 120 times on Facebook in less than 24 hours, which astounded me. I think it’s because people can identify with what I looked like on the left.
I am a Dietitian but I clearly had a “weight problem”. Despite having 2 degrees on the wall that indicate that I should have “known better” I was still obese. While the BSc from McGill in Nutritional Sciences and the MSc from UBC in Human Nutrition gave me tools that I could apply to myself to lose weight, I found it very difficult to eat a low fat, calorie restricted diet, especially given that all I do all day is talk about food.
Not only was I obese, but I also had Type 2 Diabetes for 8 years and my HbA1C kept gradually rising, year after year. Like many who are in the same boat, I then developed high blood pressure.
I was a mess.
I was a fat Dietitian.
Then I heard about the therapeutic use of a low carbohydrate diet from a retired physician friend and my life, and my clinical practice changed. Not right away, of course — but the more I read in the literature about it, the more I became convinced that this was not something I could simply write off as another “fad diet”.
I began using a low carbohydrate approach with some of my clients and then when I was sick enough and tired enough of feeling ‘sick and tired’, I did for myself what I do for others. I designed a Meal Plan for myself. And the rest, as they say, is ‘history’.
The photo below was the result of a whim to wear the same camisole and crocheted top on Friday night that I wore two years ago — just to see the difference when I’d later compare the two pictures.
When I compared them, it was almost unreal.
I used to look like that and what was far worse, was that I was really metabolically sick.
I’m not any more and I think THAT I am not struck a chord with people.
That is why I think it was liked and shared so much in such a short period of time — because people could identify with the process (either because they’ve been through it themselves or because they want to).
Twitter post, April 20, 2019
The whole story of reclaiming my healthy (March 5-2017 – March 4, 2019) is under “A Dietitian’s Journey”.
In short, I lost 55 pounds, put the symptoms of Type 2 Diabetes into remission and lowered my blood pressure. I did it without being hungry all the time and without taking medication to accomplish it. I did what I teach my clients to do and no surprise, it worked.
I made reclaiming my health a priority.
As I’ve often explained, I did it “as if my life depended on it” because it did.
Yes, I understand the process from both sides of the clinical desk — as a Dietitian and as a formerly obese person with major health issues.
I hope that by having my “fat pictures” out there from the beginning, I’ve encouraged you that I believed in advance that I was going to be successful. I did.
And here I am.
I haven’t “arrived”. I am simply making health a habit.
If I can help you do the same, please let me know.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
A newly published American Diabetes Association (ADA) consensus report on Diabetes and pre-diabetes that was just publishedonline ahead of print yesterday (April 18, 2019) indicates that;
“Reducing overall carbohydrate intake for individuals with diabetes has demonstrated the most evidence for improving glycemia* and may be applied in a variety of eating patterns that meet individual needs and preferences.”
* glycemia is blood glucose, also called “blood sugar”
NOTE: This is the first article in a series I will be writing on this new Consensus Report.
The report emphasizes that there is no “one-size-fits-all” eating pattern for the prevention or management of diabetes, and that it is an unrealistic expectation that there should be a singular eating pattern given the broad spectrum of people affected by diabetes and pre-diabetes, their cultural backgrounds, personal preferences, co-occurring conditions (i.e. co-morbidities), and the variety of socio-economic backgrounds from which they come.
The new report underlines several eating patterns that are effective to varying degrees for achieving different goals, with potential benefits including HbA1C reduction, weight loss, lowered blood pressure, improved lipids (higher HDL-c, lower LDL-c), lower triglycerides (TG).
“The most robust research available related to eating patterns for pre-diabetes or type 2 diabetes prevention are Mediterranean-style, low-fat, or low-carbohydrate eating plans.”
According to this new report, low-carbohydrate eating patterns (26-45% of total calories from carbs ) and very low carbohydrate eating patterns, also called “ketogenic” or “keto” diets (20-50 g of non-fiber carbohydrate per day) show the most evidence for blood glucose control.
The various eating patterns with their different potential benefits are summarized in Table 3, below;
Table 3 – Eating Patterns reviewed for this report [1]
The report indicates that for adults not meeting their blood sugar targets, or where there is a need to lower anti-glycemic medications that lower blood sugar, that “reducing overall carbohydrate intake with low- or very low- carbohydrate eating plans is a viable approach.”
“For select adults with type 2 diabetes not meeting glycemic targets or where reducing anti- glycemic medications is a priority, reducing overall carbohydrate intake with low or very low- carbohydrate eating plans is a viable approach.”
American Diabetes Association Consensus Recommendations Summary
A variety of eating patterns (combinations of different foods or food groups) are acceptable for the management of diabetes.
Until the evidence surrounding comparative benefits of different eating patterns in specific individuals strengthens, health care providers should focus on the key factors that are common among the patterns:
—‹ Emphasize non-starchy vegetables. —‹ Minimize added sugars and refined grains. —‹ Choose whole foods over highly processed foods to the extent possible.
Reducing overall carbohydrate intake for individuals with diabetes has demonstrated the most evidence for improving glycemia and may be applied in a variety of eating patterns that meet individual needs and preferences.
For select adults with type 2 diabetes not meeting glycemic targets or where reducing anti-glycemic medications is a priority, reducing overall carbohydrate intake with low- or very low carbohydrate eating plans is a viable approach.
If you have been recently diagnosed as pre-diabetic or as having Type 2 Diabetes (T2D) and would like to work on reversing the symptoms through a low carbohydrate or very low carbohydrate eating pattern, then I can help. I don’t believe there is a “one-sized-fits-all” approach to either of these and will work within you needs to design an individual plan just for you.
You can learn more about my services including individual hourly appointments and sessions as well as packages above under the Services tab or in the Shop.
If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
To your good health!
Joy
Here are the links to other articles that I wrote about the new ADA Consensus Report:
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Reference
Evert, AB, Dennison M, Gardner CD, et al, Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report, Diabetes Care, Ahead of Print, published online April 18, 2019, https://doi.org/10.2337/dci19-0014
Yesterday, the headlines screamed out from around the world that a new study from Oxford University found that there is a 20% higher chance of developing colorectal cancer from eating as little as one strip of bacon per day.
This sounds terrible, but is it true?
To understand what this study is reporting, it is important to understand the difference between relative risk and absolute risk.
Absolute Risk
It was known before this study, that regardless what people eat, there is approximately a 5% chance of developing colorectal cancer in a person’s lifetime (whether they eat bacon every day or not). This is known as the absolute risk. A 5% likelihood means that for every 100 people, 5 will get colorectal cancer regardless what they eat. Illustrated, this looks as follows;
Absolute Risk: 5% = 5 per every 100 people
Relative Risk
The study reported that there is a20% higher chanceof developing colorectal cancer by eating as little as one strip of bacon per day. This means that compared to not eating bacon daily, eating it daily results in one more person per 100 people developing colorectal cancer in their lifetime. This is known as relative risk and illustrated that looks as follows:
Each individual person’s increased risk of getting colorectal cancer by eating as little as 1 strip of bacon per day is NOT 20%!Their increased absolute risk of getting colorectal cancer (*based on this study) is0.08%.
*this study was an epidemiological study, not a clinical study and can only show if there is an association between two factors and cannot make any conclusions about cause. The difference is explained below.
The study found that for every 10,000 people who ate 21g a day of red and processed meat, 40 were diagnosed with colorectal (bowel) cancer, and a single slice (or rasher) of bacon is ~23g.
i.e. 40 / 10,000 = 0.4%
The study also found that for every 10,000 people who ate 76g a day of red and processed meat, 48 were diagnosed with colorectal (bowel) cancer.
i.e. 48/10,000 = 0.48%
The actual chance of a person getting colorectal cancer (i.e. absolute risk)from eating bacon daily is the difference between these two numbers;
i.e. 0.4% – 0.48% = 0.08%
Association is not Causation
This was an epidemiological study based on population data, and was not a clinical study.
Epidemiological studies are the study of diseases in populations and are helpful for researchers to know which areas warrant clinical studies. It is important to know that epidemiological studies cannot attribute “cause” of disease or death.
When an epidemiological study finds an “association” between two factors such as bacon and higher colon cancer rates — this does NOT mean that eating bacon ’causes’ heart disease.
Based on this study, all that can be said is that there was an increase in the association between eating bacon and absolute rates of colon cancer of 0.08%.
Not so impressive now, is it?
If you are having trouble sifting through all the information you read and in knowing if it is accurate, or even says what it seems to be saying, I can help. Sometimes people start by booking an appointment just to ask me those types of questions, because they want credible answers.
You can learn more about my services including individual hourly appointments and sessions as well as packages above under the Services tab or in the Shop.
If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Reference
Kathryn E Bradbury, Neil Murphy, Timothy J Key, Diet and colorectal cancer in UK Biobank: a prospective study, International Journal of Epidemiology, , dyz064, https://doi.org/10.1093/ije/dyz064
Introduction:Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information about lowering insulin resistance, keeping blood sugar at a healthy level, or maintaining (or building) muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet. Making Health a Habit are short videos (< 5 minutes in length) or short blogs on health-related topics and are quite different than Science Made Simple articles which are longer, research-focused articles.
I often get asked if walking is “real” exercise, so this morning I decided to respond to that question in the 3rd entry in my new series titled “Making Health a Habit”, which can be found here.
In this short video I share some of the reasons I choose to walk and when, along with other options that may work better for you. I also talk about some of walking’s health benefits when it comes to those who are Type 2 Diabetic or in remission from it, and tie it into the first video in the series that was on sarcopenia.
If you’d like to know how I can help you to get started eating healthier or being more active, please let me know.
You can learn more about my services and their costs above under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Day 1 getting started eating healthy or being active again is important, but what is so significant about “Day 2”?
This is the 2nd entry in the new series titled “Making Health a Habit”, which can be found here.
Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information about lowering insulin resistance, keeping blood sugar at a healthy level, or maintaining (or building) muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet. Making Health a Habit are short videos (< 5 minutes in length) or short blogs on health-related topics and are quite different than Science Made Simple articles which are longer, research-focused articles.
In this short video I explain:
Research demonstrates that it takes 2-3 months (~66 days) to do something enough that it becomes a habit [1]. For some, making something a habit is simply a matter of setting SMART Goals (as I talk about in this article) and working on them consistently until they achieve them. For others, having the support of a professional such as myself during this formative time is what makes it possible for them to make their health a habit. As I say in the video; whatever works!
If you’d like to know how I can help you get started eating healthy or working towards putting symptoms of Type 2 Diabetes or high blood pressure into remission, please let me know.
If you’d like to learn more about my own health recovery and weight-loss journey, you can find more than 2 year’s worth of articles and videos under “A Dietitian’s Journey”. Even just have a look at the very first video I made March 16, 2017 which is posted here , as it is quite remarkable to compare how I look and sound in that one, with today’s.
The photo on the left is from the first video I made on March 16, 2017 when I first began my journey, and the photo on the right is from today’s video (May 16, 2019).
You can learn more about my services and their costs above under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
To our good health!
Joy
Reference
Lally, P. , van Jaarsveld, C. H., Potts, H. W. and Wardle, J. (2010), How are habits formed: Modelling habit formation in the real world. Eur. J. Soc. Psychol., 40: 998-1009. doi:10.1002/ejsp.674
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Introduction: Making Health a Habit picks up where A Dietitian’s Journey left off and provides general health information about lowering insulin resistance, keeping blood sugar at a healthy level, or maintaining (or building) muscle mass, or may simply be my opinion on different matters related to a low carb or ketogenic diet. Making Health a Habit are short videos (< 5 minutes in length) or short blogs on health-related topics and are quite different than Science Made Simple articles which are longer, research-focused articles.
This is the 1st entry in the new series titled “Making Health a Habit”, which can be found here.
It’s been a little over a month since my last video, so here is a bit of an update as well as some thoughts that I had about sarcopenia being a “thing”. I hope this provides some helpful Monday morning encouragement.
If you’d like to know how I can help you get started on your own health “journey”, please let me know.
You can learn more about my services and their costs above under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Note: This article is mainly a Science Made Simple article with some personal comments and rhetorical questions added in, so it is categorized as both an editorial and a Science Made Simple article.
In writing the recent article about low carbohydrate diets eliminate the grains food group, I came across a statement that troubled me. It was in a Health Canada document titled What are Canada’s Dietary Guidelines? [1] and stated;
“Guidelines 1 and 2 were developed based on convincing findings from scientific reports that included extensive reviews of the literature on the relationship between food and health [1,2]. The reports are listed in Table 1. These convincing findings are supported by a well-established evidence-base and are unlikely to change in the foreseeable future as new evidence emerges.”
Note: Guideline 1 is the recommendation to eat more plant-based foods and limit foods with saturated fat and Guideline 2 is the recommendation to avoid beverages high in sugar and to eat less processed/prepared food]
To me, a natural reading of the statement seemed to indicate that the Guidelines are unlikely to change in the foreseeable future as new evidence emerges. That is, the subject of the statement is Guidelines 1 and 2 —which are said to be based on convincing findings supported by well-established evidence base and unlikely to change in the foreseeable future as new evidence emerges.
I thought that it couldn’t say what I understood it to say and asked myself what else it could have meant.
Perhaps Health Canada meant to say that they considered the evidence-base so strong that it was unlikely to change in the foreseeable future, even as new scientific evidence emerges.
I looked up the two references on which Guidelines 1 and 2 were based, namely;
Health Canada. Evidence review for dietary guidance: technical report, 2015. Ottawa: Health Canada; 2016.
Health Canada. Food, Nutrients and Health: Interim Evidence Update 2018. Ottawa: Health Canada; 2019.
Evidence Review for Dietary Guidance (2015) and Interim Evidence Update (2018) [2,3]
In looking at these documents, I found a very similar statement to the one above and which read;
“When developing dietary guidance, Health Canada uses convincing findings that are supported by a well-established evidence base and are unlikely to change in the foreseeable future as new scientific evidence emerges.” [2]
In this context, it is clear that it is the “convincing findings” that are supported by a “well established evidence-base” on which dietary guidance is based that Health Canada believes are unlikely to change in the foreseeable future as new scientific evidence emerges [1].
In support of this understanding, Health Canada says in the earlier report [3], that;
“Health Canada will update Canada’s dietary guidelines, as needed, to ensure the guidance remains consistent with the latest convincing evidence” [3].
Conclusion:
According to Health Canada, the findings are supported by such a well-established evidence-base that they are “unlikely to change in the foreseeable future, even as new evidence emerges”.
[Rhetorical question: is the evidence-base for recommending that Canadians limit saturated fat intake really so strong that it is “unlikely to change in the foreseeable future as new evidence emerges”?
As I elaborate on below, in 2015 the Heart and Stroke Foundation of Canada already questioned the link between saturated fat and cardiovascular disease in their updated position paper (a paper, that I elaborate on below was not included as a reference in the new Canada Food Guide).
In addition, the 2017 PURE epidemiological study that Health Canada references in their 2018 paper but does not cite (see below) did not find that dietary saturated fat intake was associated with cardiovascular disease.
Furthermore, a meta-analysis published just last week (months after the release of the new Canada’s Food Guide) of 43 cohort or nested case-control studies that were conducted up until July 1, 2018 did not find that higher saturated fat intake was associated with higher risk of cardiovascular disease (CVD) events.
In my opinion, the presupposition that new evidence is unlikely to change an old, “well established evidence base” assumes that the relationship between blood lipid values (such as LDL) and cardiovascular disease is almost indisputable. Current evidence does not seem to support this.
This brings me to two questions that I have about Canada’s Food Guide’s evidence-base for Guideline 1 (the recommendation to consume plant-based protein more often because it results in lower intake of foods that contain saturated fat).
My questions relate to two references that seem to me to be conspicuous by their absence.
Guideline 1; consume plant-based protein more often because it results in lower intake of foods that contain saturated fat
Question 1
BACKGROUND: Health Canada’s Interim Evidence Update 2018 [2] lists the 2016 World Health Organization (WHO) reports by Mensink (# 56, below) and Brouer (#57, below) and both of these reports are used as a basis for developing Canada’s Food Guide.
Reference list from Health Canada. Food, Nutrients and Health: Interim Evidence Update 2018. Ottawa: Health Canada; 2019
Reference 58 which is the 2017 Prospective Urban Rural Epidemiology (PURE) study by Souza, RJ, Mente A Maroleanu A et al, is listed in Health Canada’s Interim Evidence Update but is noticeably absent from the table (Annex 3) in the document and is not referenced in Canada’s Food Guide.
The PURE study was largest-ever epidemiological study which recorded dietary intake in 135,000 people in 18 countries over ~ 7.5 years, in low- medium and high income countries and which found that increased saturated fat intake was not associated with increased rates of cardiovascular disease.
Annex 3: Summary of Convincing (strong) Food and Health Relationships and Changes Since 2015, pg 5 (Reference 58 omitted)
QUESTION: Why is the PURE study omitted from the table, but is listed in the References?
Question 2
BACKGROUND: Table 2 of What are Canada’s Dietary Guidelines? [1] titled “convincing findings supporting Guideline 1” lists 5 additional reports in addition to the 2010 FAO/WHO report and the two WHO reports from 2016 and 2017 on which this Guideline was based. One of these five is the American College of Cardiology/American Heart Association report of 2013.
QUESTION: Why was the Canadian Heart and Stroke Foundation position statement titled ”Saturated Fat, Heart Disease and Stroke” released in September 2015 omitted from Table 2 of What are Canada’s Dietary Guidelines? [1] when it it is both; (a) Canadian and (b) several years more recent than the American Heart Association position statement of 2013 which was used in place?
Here is an excerpt from the Canadian Heart and Stroke Foundation position statement titled ”Saturated Fat, Heart Disease and Stroke” released in September 2015. I have highlighted sections of interest in red and put their references directly below, so they can be looked up.
HEALTH EFFECTS OF SATURATED FATS Research over several decades clearly indicates that saturated fats raise low density lipoprotein cholesterol (LDL-cholesterol) in the blood[4,10,11,15]. Research also indicates that elevated LDL-cholesterol is a risk factor for heart disease and stroke, and that lowering LDL-cholesterol decreases cardiovascular morbidity and mortality. However, epidemiological studies provide a mixed picture of the association between saturated fatty acids and cardiovascular disease (heart disease and stroke) [15-22]. Early studies found an association between cardiovascular disease and saturated fat [23,24] while more recent studies have found no such association [18,21]. These mixed findings have been the focus of recent scientific debate, and underscore that the health effects of saturated fats are complex.
Studies investigating the effects of replacing saturated (animal) fats with plant oils and unsaturated spreads (mono- and poly-unsaturated fats) have found that this dietary change results in improved cholesterol levels and reduced risk of cardiovascular disease [5,25,26]. Research further indicates that modifying the type of fat we eat seems to protect us better if we adhere to the changes for at least two years[25].
Dietary recommendations to reduce overall fat intake have also included recommendations to replace saturated fats with carbohydrates. In retrospect, this advice may have played a role in increased calorie consumption and contributed to increased rates of obesity and metabolic syndrome [19].
Studies that have looked at the individual fatty acids (i.e. lauric, stearic, myristic and palmitic acids) have found that individual saturated fatty acids may have different effects on blood cholesterol levels[4,15]. The food source from which the saturated fat is derived may have different effects on cardiovascular risk [20,22]. Additional studies are required to determine whether cardiovascular risks are influenced by the nutrients used to replace saturated fats (i.e. carbohydrates, monounsaturated fatty acids or polyunsaturated fatty acids),[21] the types of saturated fat [26] and/or the foods in which they are consumed.
References
4. Food and Agriculture Organization of the United Nations (FAO). Fats and fatty acids in human nutrition: Report of an expert consultation 2008. Rome, Italy: 2010.
5. Mozaffarian D et al. Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials. PloS Med 2010;23:7(3):e1000252.
6. Ramsden CE et al. Use of dietary linoleic acid for secondary prevention of coronary heart disease and death, evaluation of recovered data from the Sydney Diet Heart Study and updated meta-analysis. BMJ 2013;346:e8707.
7. de Oliveira Otto MC, Mozaffarian D, Kromhout D, et al. Dietary intake of saturated fat by food source and incident cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis. Am J Clin Nutr 2012;96:397-404.
8. Health Canada. Do Canadian adult meet their nutrient requirements through food intake alone? Health Canada, Ottawa 2012. Retrieved from http://www.hc-sc.gc.ca/fn-an/surveill/ nutrition/commun/art-nutr-adult-eng.php
9. Moubarac JC, Batal M, Bortoletto Marins AP, Claro R, Bertazzi Levy R, et al. Processed and ultra-processed food products: Consumption trends in Canada from 1938 to 2011. Can J Diet Pract Res 2014;75(1):15-21.
10. Department of Health and Human Services, US Department of Agriculture. Dietary Guidelines for Americans 2010. http://www. health.gov/dietaryguidelines/2010.asp. Updated 2012.
11. American Heart Association Nutrition Committee. Lichenstein AH, Appel LJ, et al. Diet and lifestyle recommendations revision 2006. A scientific statement from the American Heart Association nutrition committee. Circulation 2006;114:82-96.
12. The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). European guidelines on cardiovascular disease prevention in clinical practice (version 2012). European Heart Journal 2012;33:1635-1701.
13. Vannice G, Rasmussen H. Position of the academy of nutrition and dietetics: dietary fatty acids for healthy adults. J Acad Nutr Diet 2014;114(1):136-153.
14. National Cancer Institute. Risk factor monitoring and methods: Table 1. Top food sources of saturated fats among the US population, 2005-2006. NHANES.
15. Micha R, Khatibzadeh S, Shi P, Fahimi S, Lim S, Andrews KG, et al. Global, regional and national consumption levels of dietary fats and oils in 1990 and 2010: a systematic analysis including 266 country-specific nutrition surveys. BMJ 2014;348:e2272.
16. Mensink RP, Zock PL, Kester AD, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a metaanalysis of 60 controlled trials. Am J Clin Nutr 2003;77:1146-1155.
17. Mente A, et al. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Intern Med 2009;169(7):659-669.
18. Chowdhury R, Warnakula S, Kunutsor S, Crowe F, Ward HA, Johnson L, et al. Association of dietary, circulating and supplement fatty acids with coronary risk: A systematic review and meta-analysis. Ann Internal Medicine 2014;160:398-406.
19. Ravnskov U, DiNicolantonio JJ, Harcombe Z, Kummerow FA, Okuyama H, Worm N. The questionable benefits of exchanging saturated fat with polyunsaturated fat. Mayo Clinic Proceedings 2014;89(4):451-53.
20. O’Sullivan TA, et al. Food sources of saturated fat and the association with mortality: a meta-analysis. Am J Public Health 2013;103:e31-42.
21. Sri-Tarino PW, Sun Q, Hu FB, Krauss RM. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am J Clin Nut 2010;91(3):535-546.
22. de Oliveira Otto MC, Nettleton JA, Lemaitre RN, et al. Biomarkers of dairy fatty acids and risk of cardiovascular disease in the Multi-Ethnic Study of Atherosclerosis. J Am Heart Assoc 2013;2:e000092.
23. Hu FB, Stampfer MJ, Manson JE, et al. Dietary fats and the risk of coronary heart disease in women. New England Journal of Medicine 1997;337:1491-1499.
24. McGee DL, Reed DM, Yano K, Kagan A, Tillotson J. Ten-year incidence coronary heart disease in the Honolulu Heart Program. Relationship to nutrient intake. Am J Intern Med 2014;160:398- 406.
25. Hooper L, Summerbell CD, Thompson R, Sillis D, Roberts FG, Moore HJ, et al. Reduced or modified dietary fat for preventing cardiovascular disease. Cochrane database of systematic reviews. 2012 issue 5.
26. Jakobsen MU, O’Reilly EJ, Heitmann BL, et al. Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies. Am J Clin Nutr 2009;89:1425-1432
Final thoughts…
Health Canada has based the new Canada Food Guide on what they consider ‘convincing findings’ that are supported by a ‘well-established evidence-base’; findings that they believe are unlikely to change in the foreseeable future as new evidence emerges. As stated several times in previous articles, for those that are metabolically healthy, the new guide is a huge improvement over the previous one as it focuses on eating real, whole food and avoiding sugar-laden drinks including fruit juice, and processed foods that are high in both fat and carbs.
My main concern, as elaborated on in several previous posts is the effect of a high carbohydrate diet (even if those carbohydrates are unrefined) on the large percentage of Canadians who are metabolically unwell. My other concern is the further limiting of healthy, whole foods such as meat, seafood, cheese and milk because they contain saturated fat, when mixed research findings indicate that the relationship between saturated fat intake and cardiovascular disease is complex.
Guideline 2 to limit processed foods is fantastic and benefits all Canadians, however in my opinion, recommending that Canadians across the board limit animal based protein foods because the saturated fat they contain may predispose them to cardiovascular disease is not based on robust data. Furthermore, it unnecessarily limits foods that are the best sources of the most bioavailable sources heme-iron (outlined in this article in relation to the plant-based Eat-Lancet Diet) as well limits some of the richest sources of B-vitamins (as outlined in this article).
How does one sort through all this information and make sense of these recommendations in relationship to themselves? As part of my complete assessment, I not only ask about how you usually eat and your food preferences, and weigh and measure you, I also review your most recent lab work to determine whether you fall in the large percentage of Canadians that are no longer metabolically healthy, or don’t. From there, we’ll discuss the various options you have for improving your weight and metabolic markers so that you can decide what is the best approach for you.
You can learn more about my services and their costs above under the Services tab or in the Shop and if you have questions about these, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.To your good health!
Health Canada, What are Canada’s Dietary Guidelines? https://food-guide.canada.ca/en/guidelines/what-are-canadas-dietary-guidelines/
Health Canada. Food, Nutrients and Health: Interim Evidence Update 2018. Ottawa: Health Canada; 2019.
Health Canada. Evidence review for dietary guidance: technical report, 2015. Ottawa: Health Canada; 2016.
Heart and Stroke Foundation of Canada, Position Statement ”Saturated Fat, Heart Disease and Stroke, September 24, 2015, https://www.heartandstroke.ca/-/media/pdf-files/canada/position-statement/saturatedfat-eng-final.ashx
Note: This article is classified as an editorial as it reflects some of my own thoughts on these issues and is also classified as a Science Made Simple article, as it is rooted in the science. By way of references, I have linked to previous articles I have written (that are referenced) or to the original sources, rather than using footnotes and a reference list.
One of the common concerns is that a low carbohydrate or ketogenic diet avoids “an entire food group” (i.e. grains) and implies that people will be setting themselves up for decreased nutrient status, or even deficiency if they eat this way, but is that true? Does eliminating this entire food group pose a nutritional risk? That is the subject of this article.
I will begin by discussing food groups, however I will make a small but necessary diversion into the evidence used for recent dietary guidelines that recommend a diet low in saturated fat, as there is a link between the two. As will become clear, it is advisable to include grains in a diet that is low in meat and other animal products.
Food Groups Come and Go
With the recent re-design of Canada Food Guide, we’ve seen that food groups are not carved in stone.
The once-familiar Meat and Alternatives and Milk and Alternatives food groups were completely eliminated in the newest food guide and replaced by the somewhat all-inclusive “Protein” food group. I qualify this by saying ‘somewhat all-inclusive’ because while the illustrated sample plate of the new guide includes approximately equal amounts of animal-based and plant-based proteins, both milk and cheese are not illustrated on the front, although low fat yogurt is.
Milk and cheese both figured prominently in the past food guides, as did meat, fish and poultry of all kinds, but now inclusion of cheese and higher fat meats are relegated to the inner pages of the new guide where it is explained how to ”limit the amount of foods containing saturated fat” by limiting foods such as “higher fat meat”, “cheeses” and “foods containing lots of cheese” (see this article for details).
Of course, milk, cheese and meat can all still be included in the diet, however the new food guide recommends that these be limited due to their high saturated fat content, which is said to be linked to an increased risk of cardiovascular disease.
Health Canada writes about how the guidelines were prepared in their report “What are Canada’s Dietary Guidelines?”. They state that they considered the “best available evidence” published between 2006 and 2018 to make their recommendations, but as I will outline below, the 2017 PURE study (Prospective Urban Rural Epidemiology) — which was the largest-ever epidemiological study to date and which recorded dietary intake in 135,000 people in 18 countries over ~ 7.5 years, including high-, medium- and low income nations did not seem to be included. This study found that increased saturated fat intake was NOT associated with increased rates of cardiovascular disease.
Health Canada explains in its report that the Guidelines, including Guideline 1 to eat more plant-based food in order to lower the intake of saturated fat was based on “convincing findings” from scientific reports that included extensive systematic reviews of the literature on the relationship between food and health, and that these reports are listed in Table 1 of the report.
from Health Canada’s “What are Canada’s Dietary Guidelines?”
Best Available Evidence for Saturated Fat Recommendations
Table 1 of Health Canada’s report says that the “best available evidence” for the saturated fat recommendations in the new food guide were based on the following three systematic reviews;
Food and Agriculture Organization (FAO) of the United Nations 2010 – Fats and fatty acids in human nutrition — report of an expert consultation
World Health Organization (WHO) 2016 – Effects of saturated fatty acids on serum lipids and lipoproteins: a systematic review and regression analysis
World Health Organization (WHO) 2017 – Health effects of saturated and trans-fatty acid intake in children and adolescents: Systematic review and meta-analysis
Based on Table 2 of the report titled “Convincing findings supporting Guideline 1” (the guideline which recommends more plant-based food in order to lower intake of saturated fat) lists the same three systematic reviews as above, plus adds;
Dietary Guidelines Advisory Committee 2010: Report of the DGAC on the Dietary Guidelines for Americans
Health Canada 2012: Summary of Health Canada’s assessment of a health claim about the replacement of saturated fat with mono- and polyunsaturated fat and blood cholesterol lowering
American College of Cardiology/American Heart Association 2013: Guideline on lifestyle management to reduce cardiovascular risk: a report of the ACC/AHA task force on practice guidelines
Dietary Guidelines Advisory Committee 2015: Scientific report of the DGAC: advisory report to the Secretary of Health and Human Services and the Secretary of Agriculture
That is, the new saturated fat guidelines were based on systematic reviews from 2010, 2012, 2013, 2015 as well as the FAO/WHO recommendations from 2010, 2016 and 2017.
It appears that the largest-ever epidemiological study (PURE) that was published in 2017 and which found that saturated fat intake was not associated with cardiovascular disease, or increased rates of death was not included or was deemed for some reason to not be “best available evidence”. What is puzzling is that a key the 2018 Health Canada report titled Interim Evidence Update lists it as a reference, but doesn’t seem to refer to the study anywhere. More on that in the next article.
Systematic Reviews of Epidemiological Studies
As pointed out at the end of the previous article, epidemiological studies are the study of diseases in populations. These are helpful for researchers to know which areas warrant clinical trials, because epidemiological studies can’t attribute “cause” of disease or death.
When an epidemiological study finds an “association” between two factors such as saturated fat and higher blood lipid levels — this does NOT mean that saturated fat ’causes’ heart disease. It only means that higher saturated fat intake is associated with higher blood lipid values. Other studies associate high blood lipid values such as total LDL cholesterol to cardiovascular disease, but this is only helpful when we know which LDL is raised; the atherosclerotic small, dense sub-fraction or the neutral (or possibly protective) large fluffy sub-fraction. To know whether higher saturated fat intake causes cardiovascular disease events requires clinical trials.
There had already been eight meta-analysis and systematic reviews of evidence from randomized control trials (RCT) that had been conducted between 2009-2017 that did not find an association between saturated fat intake and the risk of heart disease that I reviewed in this article — data that was available prior to the redesign of the new food guide. As of this week we also have a new meta-analysis of clinical data from 43 study cohort group studies that was just published on April 6, 2019 which found NO relationship between higher saturated fat intake and higher risk of cardiovascular disease (CVD) events.
Not Carved in Stone
The recommendations made in the new food guide were based largely on epidemiological evidence and clinical data related to the association between saturated fat and blood lipid levels — sometimes lumping saturated fat and trans fats together. One one would hope that as clinical data from well-designed studies continues to emerge showing no association between saturated fat intake and cardiovascular disease (CVD) — the actual area of concern, that these recommendations will change.
If food groups are not carved in stone, dietary recommendations ought not to be either.
Eliminating an Entire Food Group
Now back to the topic of this article…
Is there a valid concern that those eating a low carbohydrate or ketogenic diet who are eliminating a entire food group (i.e. grains) are setting themselves up for decreased nutrient status or deficiency?
To answer that question we need to ask ourselves;
(1) which nutrients are found in grains in significant quantities
and
(2) can those nutrients be found in sufficient quantities in other foods in the diet?
If so, then eliminating grains does not predispose people to risk of decreased or deficient nutrient status.
Main Nutrients in “Healthy Whole Grains”
Yesterday evening, while writing this post, I stumbled across a recent article title ‘Healthy whole grains’ – really?! that was written by Dr. Zoe Harcombe, a Ph.D. in public health nutrition. In her article, Dr. Harcombe compiled data from the USDA’s National Nutrient Database for Standard Reference to evaluate the nutrient content in whole grain whole wheat flour, long grain brown rice, whole wheat spaghetti / pasta, oats and whole wheat bread. These foods are representative of what I think most Dietitians would categorize as ‘healthy whole grains’ which are known for being high in B vitamins such as B1 (thiamine), B2 (riboflavin), B3 (niacin) and folate (also called folic acid), as well as minerals such as iron, magnesium and selenium.
Dr. Harcombe demonstrated that foods such as chicken liver, sardines, eggs and sunflower seeds are much better sources of the B-vitamins than these “healthy whole grains”. As well, I know from having researched the topic that meat and seafood are excellent sources of the most bioavailable form of iron (heme iron which is superior to the non-heme iron found in grains). As discussed in the previous article, nuts and seeds, dark chocolate and avocados are all rich in magnesium and animal foods such as pork, beef, turkey, chicken, fish, shellfish and eggs are all rich in selenium.
Whole grains are also good sources of fiber, but so are the wide range of non-starchy vegetables that are eaten on a well-designed ketogenic diet, as well as the starchy vegetables and berries that are eaten on a well designed low- carbohydrate diet. In fact I wrote an article about this a year and a half ago.
In short, there are no nutrients found in grains that are not found in adequate, or even higher quantities in foods eaten as part of a well-designed low carbohydrate or ketogenic diet.
Some Final Thoughts…
As far as I can see, it is only the conviction that there is an established relationship between saturated fat and cardiovascular disease (based on a proxy relationship between saturated fat and blood lipids) and the resulting dietary guidelines based on that relationship that makes the eating of whole grains ‘necessary’.
The reason?
Current dietary guidelines recommend limiting animal foods so eating more plant-based foods and grains containing B-vitamins, iron, magnesium and selenium is necessary. If, however guidelines could change in the future based on emerging evidence (provided that they continue to be validated by future studies), then eating whole grains would be “optional”, since animal-based foods are equal or superior sources of those nutrients.
If ‘eating foods with saturated fat causes heart disease’, then limiting them is necessary, and eating whole grains is the next best source of these nutrients.
Personality I am not convinced that the evidence is unequivocal and that it is warranted to limit foods rich in saturated fat. At the same time, I am not persuaded that there is evidence that eating lots of saturated fat to the exclusion of other healthy fats is necessary or preferred.
Assuming the emerging evidence on the safety of saturated fat continues to hold, I believe including animal foods in the diet precludes the necessity to eat whole grains.
For those that choose to follow a vegetarian diet, the inclusion of some whole grains as good sources of B vitamins, iron, magnesium and selenium is advisable.
If you would like nutritional support to ensure you are obtaining a wide range of nutrients while following a low carbohydrate diet, I would be glad to help.
You can learn more about my services and their costs above under the Services tab or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
A newly published large-scale epidemiological study has reported that taking vitamin and mineral supplements does not reduce the risk of cardiovascular disease such as heart attack and stroke, cancer rates or other causes of health-related death. The study published Tuesday, April 9, 2019 in the Annals of Internal Medicine analyzed US nutritional data from 30, 899 adults over the age of twenty from the NHANES survey between 1999 to 2010 and linked it to mortality data from the National Death Index [1]. During the six year follow-up period there were 3613 deaths; of which 945 were cardiovascular-related and 805 were from cancer.
Vitamin and Mineral Supplement versus Nutrient Intake from Food
The study found that use of vitamin and mineral supplements was not related to improved outcomes in rates of death from cardiovascular disease, cancer or all-cause health related death. Adequate intake of vitamin A, vitamin K, magnesium, zinc and copper was associated with reduced rates of cardiovascular disease and death from all health-related causes, but these improved associations only applied to those who obtained these nutrients from food.
Calcium Supplements – too much of a ‘good’ thing
So many adults take calcium supplements, however calcium intake from supplements of ≥ 1000 mg/day (which many adults take!) was associated with increased risk of death from cancer.
Want to Live Longer? Eat Whole, Real Food
Based on this large-scale epidemiological study, eating foods rich in vitamin A, vitamin K, magnesium, zinc and copper was associated with reduced rates of cardiovascular (CVD) disease and death from all health-related causes. Good news! All of these nutrients are widely available in whole, real foods that also happen to be low in carbohydrate.
Zinc and Copper
Meat and seafood are some of the richest sources of zinc and copper.
Vitamin K
Dark, leafy greens are excellent sources of vitamin K. Vitamin K is needed to help the body absorb vitamin D and to help with proper calcium utilization.
Magnesium
Nuts and seeds, including cocoa beans (think ‘dark chocolate’!) are very good sources of magnesium, as are avocados.
Vitamin A
…and yellow and orange vegetables are excellent sources of vitamin A.
Final thoughts…
Epidemiological studies (which are the study of diseases in populations) are helpful to know what areas warrant good quality clinical trials, but aren’t useful for attributing “cause” of disease or death.
When an epidemiological study finds an “association” between two factors, this does NOT mean that one causes the other. For that, clinical trials are necessary.
That said, eating whole, real foods that also happen to be low in carbohydrate are an excellent way to get all of the nutrients that this study found are associated with lower rates of cardiovascular disease and death from all health related causes and it is pretty difficult to eat too much of any nutrient when eating whole, real food.
Since taking vitamin and mineral supplements is not associated with lower rates of disease or death, and in the cases of calcium supplements may even be associated with negative health outcomes, eating a whole-food diet rich in the above foods is the safest way to ensure adequate intake of these nutrients.
If you would like more information about how much of these foods you should be eating, I’d be glad to help. Please have a look at the Services tab or the Shop for more information.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Reference
Chen F, Du M, Blumberg JB, Ho Chui KK, Ruan M, Rogers G, et al. Association Among Dietary Supplement Use, Nutrient Intake, and Mortality Among U.S. Adults: A Cohort Study. Ann Intern Med. [Epub ahead of print ] doi: 10.7326/M18-2478
An analogy is a comparison between similar ideas to help illustrate one of them. The featured photo for this post are sugar crystals on a string and the reason for this will become clear.
The idea for this article came when someone I follow on social media (Dr. RD Dikeman*) posted the graphic below, which shows complex carbohydrates as long strings of glucose, which starches are. But there are also other types of complex carbohydrates that are long strings of different sugar molecules that can impact blood glucose differently. I thought a simple explanation of what “complex carbohydrates” are, how they are digested and how these can affect blood sugar differently might be helpful, so that is what this article is about.
graphic from RD Dikeman, Typeonegrit
*Dr. RD Dikeman holds a PhD in Theoretic and Mathematical Physics and has become very knowledgeable in carbohydrate metabolism as a result of his son having been diagnosed in 2013 with Type 1 Diabetes. His son was eating 40-60 g of carbohydrate per meal and was experiencing a “roller-coaster ride” of high and low blood sugars, including an incidence of “ketoacidosis”; which is a life-threatening condition when the body produces high levels of ketones due to an insufficiency of insulin. This should not be confused with “ketosis” where the body switches to using fat stores for energy, such as after an overnight fast. Five years ago, Dr. Dikeman’s son began to follow the low carbohydrate protocol of Dr. Richard Bernstein MD (outlined in his book “Diabetes Solution”) and since that time has been able to maintain normal normal blood sugar levels with the minimum required doses of insulin.
I liked the analogy of Dr. Dikeman’s graphic and wanted to use it as a ‘jumping off point’ for this article.
Glucose Explain Simply
Glucose (also called dextrose) is the type of sugar found in the blood which is why the common term “blood sugar” and the more clinical term “blood glucose” refer to the same thing.
Glucose is one of the two sources of energy (along with ketones) that are used to fuel the body’s cells. Even people that don’t eat “low carb” will make ketones after a night’s sleep, so the body of healthy people runs on both glucose and ketones.
The carb-containing foods that we eat are broken down into glucose for energy or the body makes the glucose it needs for the brain and red blood cells from other substances in a process called gluconeogenesis.
The Glucose-Complex Carb Analogy
In the graphic above, Dr. Dikeman questions whether people such as Diabetics that have trouble metabolizing glucose should be eating complex carbohydrates that are essentially just long strings of glucose molecules strung together like beads on a chain.
As in Dr. Dikeman’s illustration, some complex carbohydrates such as starch are just long chains of glucose molecules, however other complex carbohydrates are made up of other sugars such as galactose and fructose, along with glucose. Because of that I wanted to expand on Dr. Dikeman’s illustration.
Simple and Complex Carbs
One way that carbs are sometimes classified is as “simple” or “complex”; with starch and fiber being categorized as complex carbs and all sugars being categorized as simple carbs.
Simple Sugars
There are two types of simple sugars; monosaccharides and disaccharides.
Mono means “one” and saccharides means “sugar” so a monosaccharide is just a single sugar molecule. Di means “two”, so a disaccharide is two sugar molecules joined together.
Monosaccharides
As mentioned above, monosaccharides are made up of only a single sugar molecule and examples of these are glucose, fructose and galactose. All three monosaccharides have 6 carbons and the same chemical formula but look entirely different from each other. For example, glucose and galactose are 6-ring sugars and fructose is a 5-ring sugar.
Glucose is usually found in food bound either to other glucose molecules, as in Dr. Dikeman’s illustration above, or may be bound to other types of sugar molecules in a disaccharide (2 sugar molecules) or a starch or fiber (long chain of sugar molecules).
Fructose is the sugar found in fruit and since it is a 5-ring sugar, it can’t simply be broken down into glucose, which is a 6 ring sugar.
Galactose is a six ring sugar that rarely exists on its own in food but that can be broken down in the body through digestion. It is usually found bound to glucose to form lactose, the sugar found in milk and dairy products.
Disaccharides
Disaccharides are two monosaccharide sugar molecules bound together.
Sucrose is ordinary table sugar and made up of glucose-fructose.
Lactose is the sugar in milk and milk products and is glucuse-galactose
Maltose which rarely occurs naturally in foods, is glucose-glucose. Maltose is used in food processing such as the shiny glaze on Chinese roast duck.
complex carbohydrates
Complex carbohydrates are made up of more than two monosaccharides (sugar molecules). Oligosaccharides (where oligo means “scant” or “few”) are made up of 3-10 sugar molecules, whereas polysaccharides are made up of hundred or even thousands of monosaccharides (sugar molecules).
Oligosaccharides
Oligosaccharides are made up of 3-10 sugar molecules and the two most common are some of the complex carbohydrates found in dried beans, peas and lentils[1].
Raffinose is an oligosaccharide made from 3 sugar molecules: galactose-glucose-fructose and stachyose is an oligosaccharide made from 4 sugar molecules: galactose-galactose-glucose-fructose.
The body can’t break down either raffinose or stachyose, but this is done by the bacteria in the intestine.
Polysaccharides
Polysaccharides are made up of hundreds or thousands of sugar molecules linked together. When those sugar molecules are only glucose, the polysaccharide is called “starch”.
Some polysaccharides form long straight chains while others are branched like a tree. These structural difference affect how these carbohydrates behave when they’re heated or put in water.
The way the monosaccharides are linked together makes the polysaccharides either digestible as in starch, or indigestible as in fiber.
Polysaccharides found in plant foods such as fiber, cellulose, hemicellulose, gums and mucilages (such as psyllium) are indigestible by the body so won’t be covered in this article, but it should be noted that they can slow down the absorption of digestible carbohydrate.
Starch
Starches are long chains of glucose molecules strung together like beads on a string and are the ones illustrated in Dr. Dikeman’s illustration, above.
Starches are found in grains such as wheat, corn, rice, oats, millet and barley as well as in legumes such as peas, beans and lentils* and tubers such as potatoes, yams and cassava.
*Recall as mentioned above that peas, beans and lentils also have the complex carbohydrates called oligosaccharides which are not broken down by the body, but by the bacteria of the gut.
There are two types of starches; the long unbranched chains called amylose and the long branched chain ones call amylopectin. What is important in this context is that the long branched chain starches called amylopectin are more easily digested.
The body digests most starches very easily, although those with a high percentage of amylopectin (such as cornstarch) are digested much more easily than those with a high amount of amylose, such as wheat starch [1].
Since starches are just glucose molecules linked together and they are easily broken down to individual glucose molecules, starches can quickly affect the blood sugar of those who are pre-diabetic or have Diabetes.
That is the “point” behind Dr. Dikeman’s illustration, above which I have modified slightly, below.
adapted from graphic by RD Dikeman by Joy Y. Kiddie, MSc, RD
Those who are Diabetic (or pre-diabetic) already have challenges with their blood glucose (“blood sugar”), so does eating foods that are nothing more than long strings of glucose such as starches really make sense?
Note: While the fiber content of whole grain pasta will slow down its digestion compared to refined pasta, it is still long strings of glucose molecules. Think of whole wheat pasta as a string of pearls with in addition to the pearls, in this case fiber.
Digestion of Carbohydrates
Carbohydrate digestion begins in the mouth where an enzyme in saliva called amylase breaks starch down into shorter polysaccharides and maltose.
The acidity of the stomach temporarily stops the effect of the salivary amylase, but the digestion of carbohydrate starts up again in the small intestine where most carbohydrate digestion takes place. Digestion of carbohydrates begins again when the pancreas secretes pancreatic amylase into the small intestine.
In the small intestine, starch is broken down in to many, many individual units of the disaccharide maltose, which are simply two glucose molecules linked together. Then, enzymes located to the brush border of the small intestine break the alpha bond which holds the two glucose molecules together.
It’s easy to understand how starch, which is simply long chains of glucose molecules strung together are so easily broken down when digestion already starts in the mouth and is completed in the small intestine where the disaccharide (maltose) is broken down into 2 glucose molecules.
In the small intestine, other enzymes split other disaccharides into monosaccharides; so for example, the enzyme sucrase splits the disaccharide sucrose into glucose and fructose and the enzyme lactase splits the disaccharide lactose into glucose and galactose. Note that these other disaccharides are only 1/2 glucose.
Absorption of Carbohydrates
Monosaccharides are absorbed into the mucosal cells of the small intestine and travel to the liver, where galactose and fructose are converted to glucose and the glucose is stored in the liver as glycogen.
Glycogen is long, highly branched chains of glucose molecules (similar to amylopectin, but much more highly branched). When needed, the liver can break down glycogen into glucose at a rate of 100 mg to 150 mg of glucose per minute for up to 12 hours [2].
When glycogen stores of the liver are already full, the glucose from the broken down carbohydrate with the help of the hormone insulin converts the excess glucose into fat and sends to other parts of the body to be stored in adipose tissue.
Carbohydrate-based Foods in the Diet
As covered in previous articles including this one , there is NO requirement for people to eat carbohydrate-based food” provided that adequate amounts of protein and fat are consumed“[3] which are used to provide essential glucose for the brain via gluconeogenesis. This does not mean that I recommend people don’t eat any carbohydrate-based food!
Which carbohydrate-based food people are able to eat and in what quantity without it affecting their blood sugar to any large degree varies considerably from person to person[4], whether or not they are Diabetic. For those who already have Type 2 Diabetes or are pre-diabetic, a personalized nutrition approach is needed. This is often called “eating to your meter“; testing a specific quantity of a food by itself, to see how your blood sugar responds.
Based on research, some people with Type 2 Diabetes can do well eating certain types of legumes (pulses) including black beans, white navy beans, pinto beans, red and white kidney beans, chickpeas and fava beans [5] which is helpful for those who follow a plant-based vegetarian diet. Once people have lowered their HbA1C and fasting blood glucose levels and achieved remission of Type 2 Diabetes symptoms, I work can work with them in determining which foods they can re-introduce into their diet and in what quantities and how often, so as not to adversely impact their blood sugar. Some do better than others.
Over the last 4 years of my clinical practice, I have found that many people with pre-diabetes or Type 2 Diabetes can often manage their blood glucose well while including small servings (1/2 cup / 125 ml) of whole-food starchy vegetables such as winter squash (butternut, acorn, kobacha, etc.), as well as small servings of other starchy whole-food vegetables such as orange or purple yam, or peas. For those eating a moderately-low level of carbs (non-ketogenic) or want to keep eating these foods, I encourage them to choose these more often over starch-based foods such as pasta, rice and bread.
That doesn’t mean that people with Type 2 Diabetes shouldn’t ever eat whole, unmilled brown rice or quinoa but that avoiding refined starches such as white bread, pasta and rice is best preferable.
I hope that you found this article helpful to understand what complex carbohydrates are, and why certain types of complex carbs are more of a challenge to those with Type 2 Diabetes or pre-diabetes.
If you have questions about how I can help you eat in a way to lower your blood sugar levels, please send me a note through the Contact Me form above and for information about the types of services I offer, please have a look under the Services tab or in the Shop.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Chapter 4, Carbohydrates: Simple sugars and Complex Chains, http://samples.jbpub.com/9781284064650/9781284086379_CH04_Disco.pdf
National Academies Press, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids (2005), Chapter 6 Dietary Carbohydrates: Sugars and Starches”, pages 265-275
Zeevi D, Korem T, Zmora N, et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell. 2015 Nov 19;163(5):1079-1094.
Sievenpiper, J.L., Kendall, C.W.C., Esfahani, A. et al. Effect of non-oil-seed pulses on glycaemic control: a systematic review and meta-analysis of randomised controlled experimental trials in people with and without diabetes. Diabetologia (2009) 52: 1479.
A recently published meta-analysis of 43 cohort or nested case-control studies up until July 1, 2018 [1] did not find that higher saturated fat intake is associated with higher risk of cardiovascular disease (CVD) events. This is the first study to examine the effect of total dietary fat intake and the intake of specific fatty acids on CVDs risk based on dose-response meta-analysis of prospective cohort studies.
It has been proposed that saturated fat (SFA) and trans fatty acids (TFA) contribute to CVD via inflammatory mechanisms and oxidative stress, mediated through the production of reactive oxygen species (ROS) [2,3]. With respect to trans fatty acids, this new study found that dietary TFA intake had a dose-response association with CVDs risk; specifically a 16% increased risk of CVD with an increased TFA intake of 2% of energy per day, however no association was observed between total fat or dietary saturated fatty acid (SFA) intake and the risk of CVDs [1]. In addition, this meta-analysis found no protective effect from the consumption of either monounsaturated fatty acids (MUFA), or polyunsaturated fatty acids (PUFA) and risk of CVDs, except PUFAs showed a protective effect in sub-group analysis followed up for more than 10 years [1].
These findings do not support 2010 recommendations of the WHO / FAO [4] which continue to influence national dietary guidelines around the world to recommend reducing intake of saturated fat in order to lower the rates of CVD.
As well, these new findings call into question the findings of the PREDIMED study [5] and the Lipid Research Clinics Prevalence Follow-up Study [6] that indicated that diets high in polyunsaturated fatty acid (PUFA) and monounsaturated fatty acid (MUFA) and low in saturated fatty acid (SFA) and trans fatty acids (TFA) are associated with reduced CVDs events.
The authors caution that;
“it is possible that the role of dietary fat played in the development of CVDs might be confounded by the fat sources. For instance, vegetables and fruits play protective roles in the development of CVDs. However, we could not investigate the different effects of fat from animal, vegetables and fruit separately in this current meta-analysis.” [1]
Some thoughts…
For almost 50 years it has been believed that dietary saturated fat intake was a risk factor for CVDs based on the assumption that dietary fat can increase low density lipoprotein (LDL) cholesterol and blood pressure and in turn, increase CVDs risk, however this meta-analysis of 43 cohort studies did not find a positive association between total dietary fat intake or saturated fat intake and CVDs risk.
The 2017 Prospective Urban Rural Epidemiological (PURE) study (covered in this earlier article) is the only prospective study to date which covered multiple world regions and which found that total dietary fat and types of dietary fat were not associated with cardiovascular disease or mortality and further, that dietary saturated fat had an inverse association with stroke and a risk of all-cause mortality with higher intake (up to ~14% of energy intake). That is, dietary saturated fat intake was protective.
The findings of the current meta-analysis study, combined with the findings of the 2017 PURE study call into question current dietary recommendations which continue to recommend that people limit dietary saturated fat in order to reduce cardiovascular risk. Such recommendations are included in the most recent Canada’s Food Guide which encourages Canadians to ”choose foods with healthy fats instead of saturated fat” and to ”prepare meals and snacks using ingredients that have little to no added sodium, sugars or saturated fat” (see this article for details) *.
Post publication note (April 7, 2019): As I’ve stated in previous articles, I am not opposed to Canada’s new Food Guide. It is a huge improvement over it’s predecessor for many reasons already discussed. My two concerns that I’ve expressed previously remain; (a) that the recommendations for the general population to continue to limit saturated fat because it contributes to CVD has not been conclusively demonstrated. The only thing that has been shown is that saturated fat can raise LDL, but which LDL; the large fluffy sub-fraction, or the small dense sub-fraction? Please see article linked to above for an elaboration. My second concern is that (b) the recommended amount of carbohydrate is too high for the large percentage of the population that are already metabolically unhealthy. Please see this article for an elaboration.
Author’s Conclusions
The study’s authors concluded that;
“This current meta-analysis of cohort studies suggested that total fat, SFA, MUFA, and PUFA intake were not associated with the risk of cardiovascular disease. However, we found that higher TFA intake is associated with greater risk of CVDs in a dose-response fashion. Furthermore, the subgroup analysis found a cardio-protective effect of PUFA in studies followed up for more than 10 years. Dietary guidelines taking these findings into consideration might be more credible.” [1]
If you would like to learn about the types of fats in your diet and how they may impact your health or those of your family, please send me a note through the Contact Me form on the tab above. You can learn more about the services I provide by clicking on the Services tab or having a look in the Shop.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Zhu Y, Bo Y, Liu Y, Dietary total fat, fatty acids intake, and risk of cardiovascular disease: a dose-response meta-analysis of cohort studies, Lipids in Health and Disease (2019) 18:91, https://doi.org/10.1186/s12944-019-1035-2
Sverdlov AL, Elezaby A, Qin F, Behring JB, Luptak I, Calamaras TD, Siwik DA, Miller EJ, Liesa M, Shirihai OS, et al. Mitochondrial reactive oxygen species mediate cardiac structural, functional, and mitochondrial consequences of diet-induced metabolic heart disease. J Am Heart Assoc. 2016;5:e002555.
Ruparelia N, Chai JT, Fisher EA, Choudhury RP. Inflammatory processes in cardiovascular disease: a route to targeted therapies. Nat Rev Cardiol. 2017;14:133—44.
Nations FaAOotU. Summary of conclusions and dietary recommendations on total fat and fatty acids in fats and fatty acids in human nutrition—report of an expert consultation. Geneva: FAO/WHO; 2010.
Estruch R, Ros E, Salas-Salvado J, Covas MI, Corella D, Aros F, Gomez- Gracia E, Ruiz-Gutierrez V, Fiol M, Lapetra J, et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med. 2013;368:1279—90.
Guasch-Ferre M, Babio N, Martinez-Gonzalez MA, Corella D, Ros E, Martin-Pelaez S, Estruch R, Aros F, Gomez-Gracia E, Fiol M, et al. Dietary fat intake and risk of cardiovascular disease and all-cause mortality in a population at high risk of cardiovascular disease. Am J Clin Nutr. 2015;102:1563—73.
Dehghan M, Mente A, Zhang X, Swaminathan S, Li W, Mohan V, Iqbal R, Kumar R, Wentzel-Viljoen E, Rosengren A, et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. Lancet. 2017;390:2050—62.
Recently, I came across a social media post about someone that wanted to drink green tea for it’s health benefits, but just couldn’t get over it’s “bad taste”. I followed the origin of the thread to Reddit, where people guessed whether green tea’s “off taste” for that person may be genetic, like the taste of cilantro. While that can be the case (i.e. genetic sensitivity to a compound called 6-n-propylthiouracil which is found in some flavonoids), others touched on whether it was because the person was making tea using supermarket green tea bags rather than loose tea, whereas a few people hit on the complexity of the issue. In this post I will discuss some of the factors that affects whether your green tea has a pleasant or “off taste”, because after all green tea should be something you actually enjoy and not only drink for it’s health benefits.
NOTE: The first part of this article are some personal details of my experience learning to prepare multi-ethnic food and beverages and the second part of the article is specifically about the preparation of green tea and its health benefits.
Once a Foodie, Always a Foodie
I have been adventurous in trying different kinds of food and beverages since I’m little and I remember my parents taking me to an authentic Japanese restaurant even as a kid. As a teen, I enjoyed cooking multi-ethnic food and learned authentic Cantonese cooking in the 1970s when my mom took a course in Chinatown. In the 1980’s, I learned authentic Thai cooking from the friend of a family business associate who was from Thailand and in those days one couldn’t buy pre-made Thai curry pastes that are available everywhere now, so I sourced the raw ingredients in Lao-Thai groceries and hand-pounded them myself in a mortar and pestle (that I still own and use!). I still have the recipe books sent to me from Thailand.
It didn’t matter whether it was Asian, Middle Eastern or Jamaican, I was a bit of a purist; wanting the ingredients and cooking method to be as authentic as possible. For me, the best way to find out how to make something was to ask someone from that culture that loved to cook.
What was true about food was also true for beverages.
I couldn’t just enjoy a cup of coffee or glass of wine without knowing more. Whether it was the origin of the coffee beans, the length of time the beans were roasted, or how long the water is in contact with the beans — I needed to know, and I was interested in such things when it was not popular either.
Before “West Coast coffee” was a thing and before there ever was Starbucks® or Peet’s, there was a place called La Vieille Europe on St. Laurent Blvd in Montreal which was where I got my single origin, whole bean coffee. As I found out years later, the son of the roaster that owned that store taught the original roaster from Peet’s in the US how to roast beans. Small world.
When I lived in wine country (Sonoma county) of California for a few years in the early 2000s, I was determined to educate my palate to distinguish between different types of wine, which I did. I knew what I liked — which turned out to be an expensive habit when I returned to Canada after 9/11. At the beginning I explored the wines of Australia and found some I really liked, but missed the delicious and inexpensive wines of Sonoma and Napa.
Once again, my palate returned to coffee, but finding a decently roasted coffee in Vancouver BC was harder than I thought. Given that this was the “West Coast”, I was discouraged how difficult it was to find good quality Arabica beans that weren’t over roasted. I stumbled across a few small roasters that did an excellent job, but in time they modified their roasts for “local tastes”, so once again, I was back looking for a new roaster. On a few occasions, I ordered from La Vieille Europe in Montreal because in the 40 or 50 years they have been in business, they never lost their passion for properly roasted, single origin coffee.
Over the 20 years I have lived in Vancouver, I discovered the world of quality tea that is largely unknown to most non-Asian born Chinese. There was one excellent tea importer in the Chinatown that I knew of and one that is still in the Richmond Public market that have single origin estate teas that rival the diversity of the best coffee roaster. Over the past 20 years, I’ve explored different types of tea from China and have come to like a few; my favourite of which is a fermented tea known as Pu-ehr.
A number of years ago, I stumbled across matcha tea in a specialty Japanese store before it was a “thing”. Knowing nothing about it, I have since found out that I had been using ‘culinary matcha‘ (designed for making Japanese sweets) for drinking. No wonder it tasted bitter and I needed to blend it with other ingredients to make it palatable. Thankfully, when fresh it had the same health benefits, which I wrote about in 2013 in this article about the Role of Green Tea Powder (Matcha) in Weight and Abdominal Fat Loss. As you’ll read below, I have since learned about making and enjoying real ceremonial-grade matcha, which is intended for drinking from large matcha bowls.
Learning about Japanese Green Tea
At the beginning of this year, I began to explore green teas from Japan when I discovered Hibiki-An, an online tea importer from Uji region of Kyoto. My culinary world expanded once again.
Unable to decide between the many different types and grades of tea that they carry, I order a sampler of 3 types of green teas (Sencha, Gyokuro Superior and Sencha Fukamushi). They came in 4 oz individual bags — the quantity that can be reasonably be used up within 3 months, when it is fresh. All 3 teas were all of “superior” grade, which is not the best quality (as my palate is not developed yet) but is a high grade tea.
When the tea arrived, it came with very specific brewing instructions (a summary of the much more detailed instructions on their web page). I’ve since learned that different types of green tea require different water temperatures and different lengths of brewing time.
Wow, who knew?
For the purpose of “cooling” the water to just the right temperature, there is a yuzamashi — which is a small ceramic cup with a spout that the boiled water gets poured into to cool momentarily before being poured into the kyuzu; a special tea pot with a single handle, built in mesh filter and large opening for the water (see photo, above).
You don’t need the get fancy, though. I had these things for years from my days exploring different regional teas, but one can use an ordinary bowl to cool the water and any plain ceramic tea pot to brew the tea in!
Tea to Water Ratio, Water Temperature and Steeping Time
Each type of green tea has a very specific ratio of green tea leaves to water, and very specific water temperatures and steeping time.
For example, of the three teas in my sample set, Sencha is brewed at 80° Celsius (176 ° Fahrenheit) for one minute, Gyokuro is brewed at 60-70 ° Celicus (140-158° Fahrenheit) for 1 -1/2 to 2 minutes and Sencha Fukamushi is brewed at the same temperature as regular Sencha, but for only 40-45 seconds.
I’ve discovered that following these guidelines using good quality, fresh tea leaves makes a cup of tea that is like nothing I’ve tasted anywhere before. It is not simply snobbery, but the science of what makes for a good cup of tea.
Note: I downloaded several studies that have researched the difference in brewing time, water to tea leaf ratio and water temperature but have decided against boring anyone with the details.
Recently, I became ready to move onto “real” matcha tea and ordered some from the same supplier in Japan.
It came in tiny cans (quantities that should be used up in a 3 week period).
The colour was a bright jade green and the taste had no hint of bitterness whatsoever!
It tastes amazing!
My teas ordered from Japan are my “weekend teas” and during the week I used run-of-the-mill Sencha purchased locally at a Japanese store.
I drink them because I like them and for the health benefits.
Health Benefits of Green Tea
The health benefits of green tea are many. Several large-scale population studies have linked increased green tea consumption with significant reductions in the symptoms of metabolic syndrome; a cluster of clinical symptoms which include insulin resistance and hyperinsulinemia (high levels of circulating insulin), Type 2 Diabetes, high blood pressure, and cardiovascular disease including coronary heart disease and atherosclerosis.
Catechins make up ~ 30% of green tea’s dry weight, of which 60—80% are catechins. Oolong and black tea which are produced from partially fermented or completely fermented tea leaves contains approximately half the catechin content of green tea.
It is believed that epigallocatechin gallate (EGCG) which is the most abundant catechin in green tea actually mimics the action of insulin, which has positive health effects for people with insulin resistance or Type 2 Diabetes [Kao et al].
EGCG also lowers blood pressure almost as effectively as the ACE-inhibitor drug, Enalapril, having significant implications for people with hypertension (high blood pressure) and cardiovascular disease [Kim et al].
Green tea catechins also have benefit for weight loss. A 2009 meta-analysis of 11 green tea catechin studies found that subjects consuming between 270 to 1200 mg green tea catechins / day (1 — 4 tsp of matcha powder per day) lost an average of 1.31 kg (~ 3 lbs) over 12 weeks with no other dietary or activity changes [Hursel].
Drinking 8-10 cups of green tea per day is enough to increase blood levels of EGCG into a measurably significant range [Kim et al], but matcha contains 137 times greater concentration of EGCG compared to green tip tea [Weiss et al].
WARNING TO PREGNANT WOMEN While EGCG has also been found to be similar in its effect to etoposide anddoxorubicin, a potent anti-cancer drug used in chemotherapy [Bandele et al], high intake of polyphenolic compounds during pregnancy is suspected to increase risk of neonatal leukemia. Bioflavonoid supplements (including green tea catechins) should not be used by pregnant women [Paolini et al].
Green Tea Shouldn’t Taste Bad!
The reason someone would find green tea has an “off flavor” was because the tea was either not fresh, not of a half-decent quality, was brewed at the wrong temperature or for the wrong length oftime. Think about it this way; it all a person ever drank was cheap pre-ground coffee, they might think coffee tasted bad, too.
The fact is, one doesn’t need to order tea from Japan to enjoy a decent cup of green tea! I found the green teas below at a local Japanese grocery store and when brewed properly they are great as everyday tea.
If you aren’t adventurous to explore ethnic markets or time is limited, I can highly recommend the online supplier I mentioned above as having excellent price for the quality of green tea, very good explanations on their web page and quick delivery.
For everyday use, I have a little water cooler (yuzamashi) bowl and small single handed tea pot (kyuzu) so brewing a decent quality sencha green tea (my daily tea of choice) has become second nature, but as I mentioned above, one doesn’t need special equipment to make a decent cup of green tea! All you need is the right amount of fresh, good quality tea leaves steeped for the right length of time in hot water that’s at the right temperature. The only thing to keep in mind is that once the package of tea is opened, it needs to be stored in a sealed, airtight, light-proof container and used up within 3 months or sooner.
Making a good cup of green tea is not really much different than brewing a good cup of coffee. To make a good cup of coffee, one needs to consider the country / countries of origin of the beans, the bean roasting time and temperature, the brewing method involved (drip, espresso, French press, etc), the required water temperatures needed for that method, and the different grind of beans and a specific water-to-ground-bean ratio required for that brewing method. It sound’s complicated, but if you a few types of coffee regularly, it’s not hard.
It’s the same with green tea.
In one sense, there is a lot to learn at first to make a good cup of green tea but on the other hand, once you know a few basics and find a green tea or two you really enjoy, the rest is easy!
Tea has amazing health benefits, but unlike the cough medicine Buckley’s®, there is no need to drink tea that “tastes terrible, but it works”!
If you would like to know more about what I do as a Dietitian and how I can help you with weight loss or to seek to reverse the symptoms of metabolic syndrome, including Type 2 Diabetes, high blood pressure and other related markers, please send me a note using the Contact Me form on this web page.
If you would like to learn more about the services I offer and their costs, please click on the Service tab or have a look in the Shop.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Gayathri Devi A, Henderson SA, Drewnowski A. Sensory acceptance of Japanese green tea and soy products is linked to genetic sensitivity to 6-n-propylthiouracil. Nutr Cancer. 1997;29(2):146-51
Hursel R, Viechtbauer W, Westerterp-Plantenga MS. The effects of green tea on weight loss and weight maintenance: a meta-analysis. Int J Obes (Lond) 2009;33:956—61.
Paolini, M, Sapone, A, Valgimigli, L, ”Avoidance of bioflavonoid supplements during pregnancy: a pathway to infant leukemia?”. Mutat Res 527 (1—2): 99—101. (Jun 2003)
Kao YH, Chang MJ, Chen CL, Tea, Obesity, and Diabetes, Molecular Nutrition & Food Research, 50 (2): 188—210, February 2006
Kim JA, Formoso G, Li Y, Potenza MA, Marasciulo FL, Montagnani M, Quon MJ., Epigallocatechin gallate, a green tea polyphenol, mediates NO-dependent vasodilation using signaling pathways in vascular endothelium requiring reactive oxygen species and Fyn, J Biol Chem. 2007 May 4;282(18):13736-45. Epub 2007 Mar 15.
Weiss, DJ, Anderton CR, Determination of catechins in matcha green tea by micellar electrokinetic chromatography, Journal of Chromatography A, Vol 1011(1—2):173-180, September 2003
I’ve heard that some types of cancer feed on glucose (the sugar in our blood) and I know of a few people that started a ketogenic diet as adjunct therapy to be used along side surgery and chemotherapy in the treatment of glioblastoma (a form of aggressive brain cancer), but just came across an article that explains why limiting sugar intake can lower one’s risk of cancer. In this article, I explain one biological link between cancer and sugar.
A “Master Switch for Cancer”
In the 1980’s, Dr. Lewis Cantley was a Professor at Tufts University School of Medicine in Boston when he identified a previously unknown enzyme known as phosphoinositide-3-kinase, or PI3K which turned out to a type of ‘master switch for cancer’.
PI3K’s normal function is to alert cells to the presence of the hormone insulin; resulting in the cells pumping in glucose to be used as metabolic fuel for the cell. Signals from PI3K are necessary for normal cell growth, survival and reproduction, however when this enzyme is hijacked by cancer cells, it provides tumors with an over-abundant supply of glucose, which results in their rapid proliferation.
The gene that codes for PI3K is now thought to be the most frequently mutated cancer-promoting gene in humans and is believed to be associated with 80% of cancers, including those of the breast, brain and bladder.
In 2012, Dr. Cantley became the Director of the Sandra and Edward Meyer Cancer Center at Weill Cornell Medicine, which is the biomedical research unit and medical school of Cornell University, where he is Professor of Cancer Biology. In his work at Weill Cornell, Dr. Cantley has continued to investigate the role of PI3K.
Challenges with some anti-cancer drugs that have been developed that block the PI3K enzyme is that these PI3K-inhibitor drugs are designed to starve the cancer cell of glucose, but also signal the person’s liver that their body is starving for glucose, too. As a result, the liver would break down glycogen (a storage form of glucose) and send large amounts of glucose into the person’s blood, resulting in their blood sugar spiking and triggering their pancreas to release lots of insulin, as a result. The presence of all of this glucose from the liver and insulin from the pancreas resulted in these patient’s tumors continuing to grow.
Dr. Cantley and his colleagues wondered whether the spike in insulin from the breakdown of glycogen might be countering the effect of the PI3K-inhibiting drugs by reactivating the PI3K pathway in the cancer cells. Studies first tried giving these patients Diabetes medications to lower their blood sugar and insulin levels, but this didn’t work nearly as well as what they tried next.
The researchers came up with a theory that a ketogenic diet (a diet that is very low in carbohydrate) could prevent the spikes caused in blood sugar by the PI3K-inhibiting drugs and might help the drug starve the tumor, while the patient’s blood sugar remained normal because the body would be fueled by breaking down fat and protein for ketones.
They tested the theory using genetically engineered mice that developed pancreatic, bladder, endometrial and breast cancers and treated the mice with a new PI3K inhibitor drug. The study demonstrated that spikes of insulin did indeed reactivate the pathway in tumors, countering the anti-cancer effect of the drug. However, when the researchers put the mice on a ketogenic diet, in addition to the medication, the tumors shrank. The results were published in the journal Nature in July 2018.
Dr. Cantley explains the biological connection between cancer and sugar this way;
“Our pre-clinical research suggests that if somewhere in your body you have one of these PI3K mutations and you eat a lot of rapid-release carbohydrates, every time your insulin goes up, it will drive the growth of a tumor. The evidence really suggests that if you have cancer, the sugar you’re eating may be making it grow faster.”
Some Final Thoughts…
A normal cell function requires the enzyme PI3K that results in the cell pumping in glucose to fuel growth and reproduction and a cancer cell that has a defect in the gene that codes for PI3K may do the same thing. Sugar, in and by itself does not cause cancer, but in those that have a few abnormal cells, sugar can drive the process of tumor development.
According to the World Health Organization, the average American consumes 126 grams of sugar a day, more than people in any other country and the average Canadian eats almost 90 grams (89.1) of sugar per day. Sugar is not required in the diet; in fact, there is no essential need to eat carbohydrate at all, if people eat adequate amounts of healthy fats and protein.
Given that as many as 88% of Americans are already metabolically unhealthy — with likely a smaller percentage of Canadians following suit (due to slightly lower obesity statistics), there is no valid reason for the average American or Canadian to be eating foods with added sugar.* As I’ve written about in many previous articles, high blood sugar and high insulin levels already predispose people to Type 2 Diabetes and obesity and as outlined in this article, are involved in the proliferation of some types of cancer cells.
*(update April 29, 2019): While I say above that there is ”no valid reason” for those who may already be metabolically unwell to eat foods with added sugar — in retrospect, this is not well worded. I think there are lots of valid reasons for people to eat foods with added sugar, but believe that it may be preferable for those who are already metabolically unwell to limited added sugars.
It would seem to me that a prudent approach for metabolically healthy people (12% of Americans, and perhaps an estimated 25% of Canadians) is to stay healthy by avoiding processed foods that are high in refined carbs and sugar, as well as foods high in “natural sugar” such as 100% fruit juice in order to reduce the risk of becoming metabolically unwell or inadvertently feeding malignant cells that feed on glucose.
For the large majority of those that are already metabolically unhealthy, a well-designed low carbohydrate diet can help you reverse the symptoms of Type 2 Diabetes, putting the disease into remission, as well as achieve and maintain a healthy body weight. Not inadvertently feeding tumor proliferation seems like a nice ‘side benefit’, too.
If you would like to know more about how I can help you achieve and maintain a healthy body weight or halt the progression of Type 2 Diabetes and other related metabolic disorders, please send me a note using the Contact Me form on this web page. If you would like to learn more about the services I offer and their costs, please click on the Service tab or have a look in the Shop.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Dr. Laura Saslow, PhD serves on the nutrition review committee for the American Diabetes Association (ADA) and spoke on March 15, 2019 at the 42nd annual National Food Policy Conference in Washington, DC . She was on a panel of experts discussing the tremendous cost of diet-related disease and the role of public policy in encouraging healthier eating.
The talk was titled, Let Food Be Thy Medicine and Dr. Saslow said this;
“…The American Diabetes Association (ADA) reviewed all of the clinical trial evidence for the new 2019 ADA clinical guidelines and has noted that a very low carbohydrate diet (VLCD) of 20-35g carbohydrate per day (not low in fat or salt) is the most powerful eating approach for treating type 2 diabetes, leading to a 40-50% remission rate.
Current standard of care leads to less than a 5% remission rate.
VLCD can also be helpful for patients with type 1 diabetes, pre-diabetes, hypertension, nonalcoholic fatty liver disease, polycystic ovarian syndrome and Alzheimer’s disease, and there is now more clinical trial evidence for VLCD than for any other eating pattern…”
In December, the American Diabetes Association (ADA) released its 2019 Standards of Medical Care in Diabetes, including its Lifestyle Management Standards of Care which included use of a low carbohydrate diet (you can read about that here), but that the ADA has now noted that a very low carbohydrate diet of 20-35 g carbohydrate per day is “the most powerful eating approach for treating Type 2 Diabetes, leading to a 40-50% remission rate” compared to the current standard of care which leads only to “less than a 5% remission rate” is very exciting.
A very low carbohydrate diet listed as Medical Nutrition Therapy in the upcoming 2019 American Diabetes Association Clinical Guidelines will certainly pave the way for organizations such as Diabetes Canada to re-evaluate the strength of the evidence for use of carbohydrate restriction for significantly improving remission rates for those with Type 2 Diabetes in this country.
What an exciting time to be a Dietitian!
NOTE: The video of her speaking had been posted on YouTube at https://www.youtube.com/LEKw1Ri7ryA but has since been deleted as the individual posting it did obtain permission to post it.
You can find out more about the hourly consultations and packages I offer by clicking on the Services tab above and if you have questions, feel free to send me a note using the Contact Me form, and I will reply as soon as I am able.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
If you live almost anywhere in Canada and are looking for a Registered Dietitian with experience providing low carbohydrate or ketogenic diet support, I can help.
Whether you live in British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Quebec, New Brunswick, Nova Scotia, Newfoundland or Labrador, I am now licensed to provide you with services.
I currently can’t provide Dietitian services to Prince Edward Island (PEI) but if I have enough demand, I will consider becoming licensed in that province, as well.
Registered in British Columbia since 2002
I have been registered with the College of Dietitians of British Columbia since 2002 as an RD(t) and since 2008 as a full registrant. This registration enables me to provide services to people across Canada, with the exception of Alberta and PEI but since I’ve had several physicians in Alberta who have asked to refer patients to me as well as individuals from Alberta requesting services, I recently applied to- and was accepted into the College of Dietitians of Alberta.
Provincial Registration Requirements for Virtual Dietetic Practice
As can be seen from the table below, Registered Dietitian such as myself that provide virtual Dietetic practice services (Distance Consultation) to other provinces are required to meet very specific registration requirements, as well as observe other regulatory regulations.
Virtual Dietetic Practice (Telepractice) – from the Alliance of Dietetic Regulatory Bodies. August, 2017
In the US or overseas?
I am a member of the College of Dietitians of British Columbia as well as the College of Dietitians of Alberta and am licensed to provide Registered Dietitian services in most provinces in Canada (except PEI), but if you live in the USA or elsewhere, I can provide you with low carb or ketogenic nutrition education services that would not be considered medical nutrition therapy (MNT) and that would be provided for information purposes only.
More Info
If you would like more information, you can find out more under the Services tab or by looking in the Shop. If you have specific questions, please send me a note using the Contact Us form on the tab above and I’d be glad to reply as I am able.


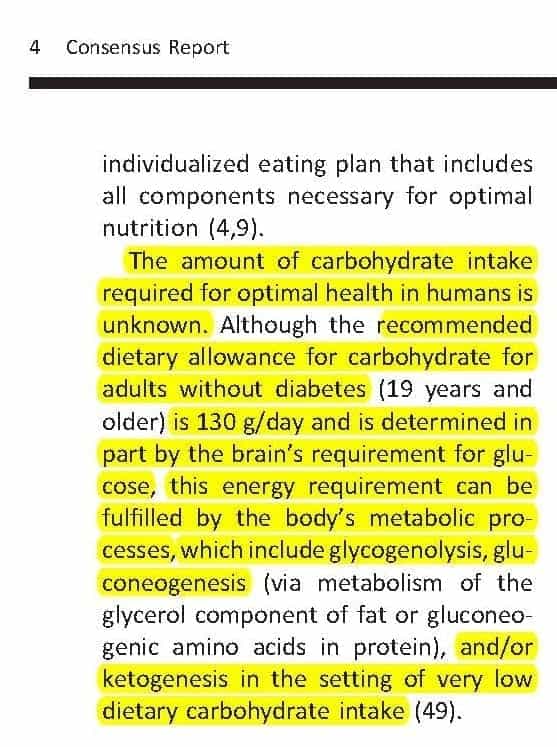

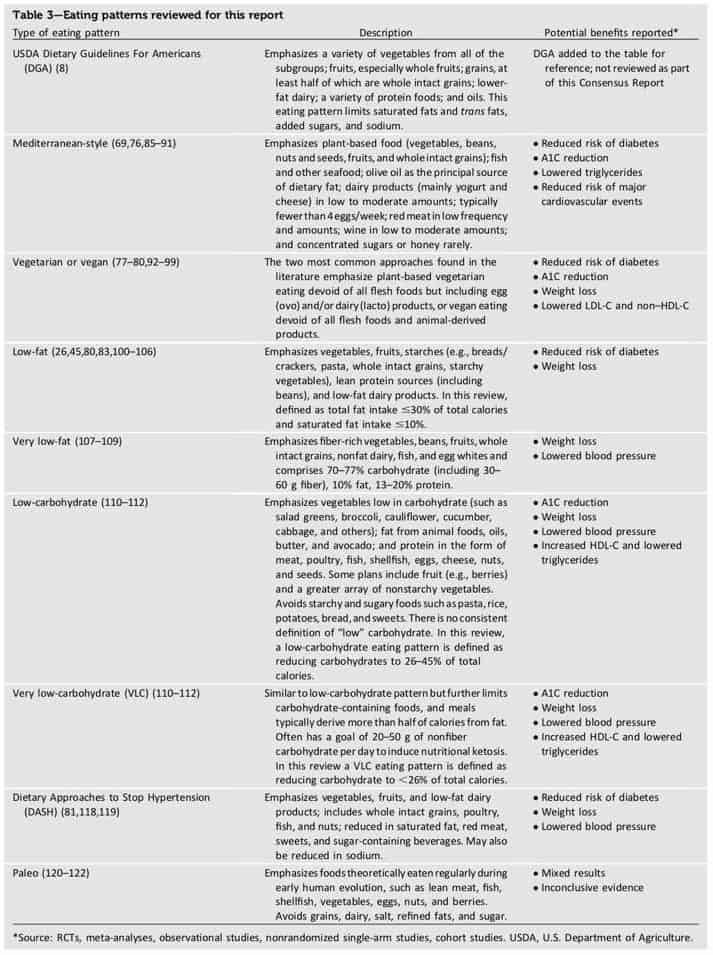
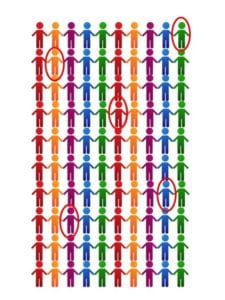
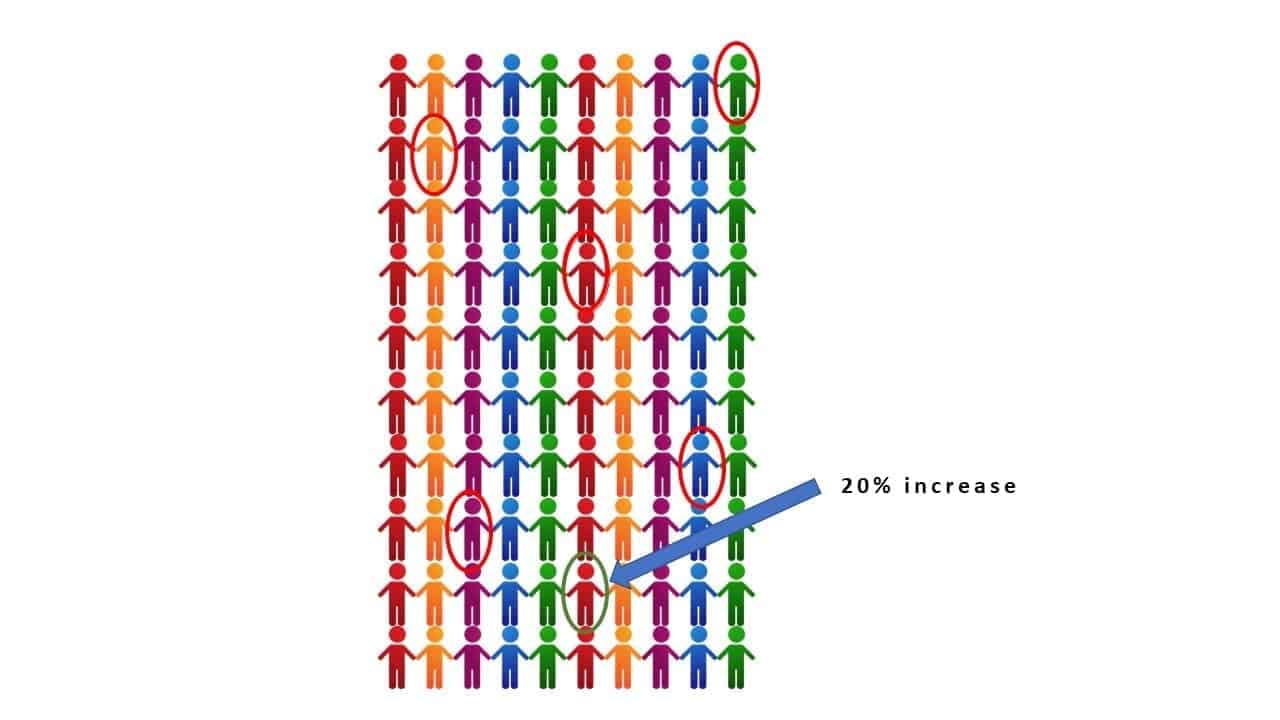



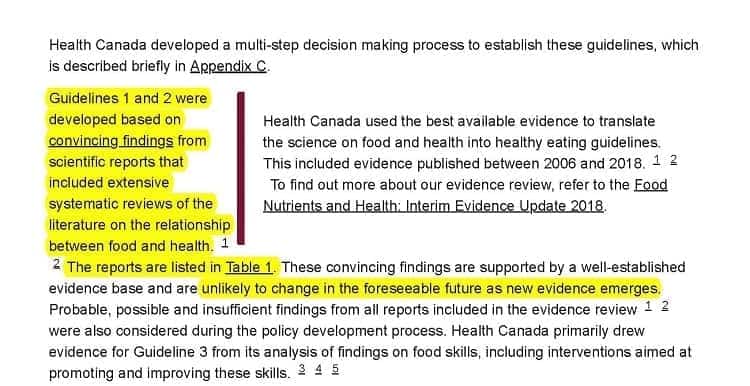



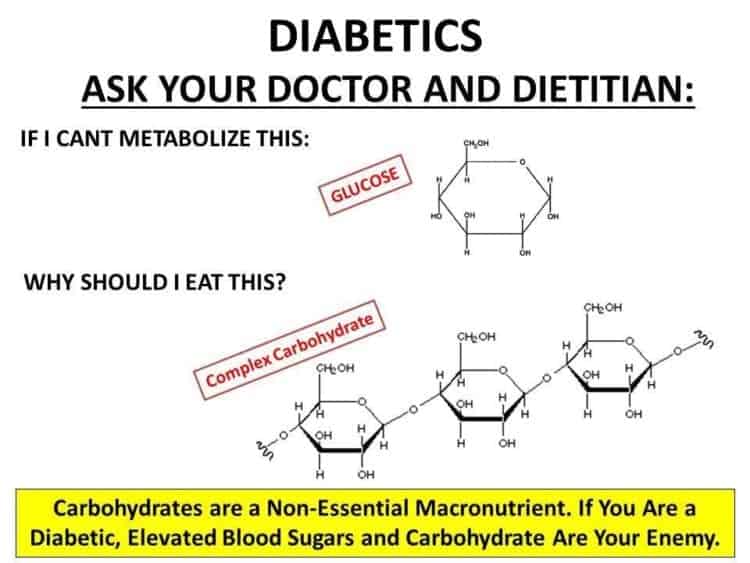
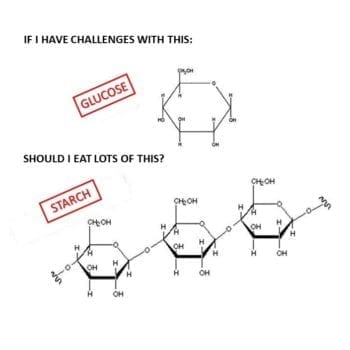
 What was true about food was also true for beverages.
What was true about food was also true for beverages. Once again, my palate returned to coffee, but finding a decently roasted coffee in Vancouver BC was harder than I thought. Given that this was the “West Coast”, I was discouraged how difficult it was to find good quality Arabica beans that weren’t over roasted. I stumbled across a few small roasters that did an excellent job, but in time they modified their roasts for “local tastes”, so once again, I was back looking for a new roaster. On a few occasions, I ordered from La Vieille Europe in Montreal because in the 40 or 50 years they have been in business, they never lost their passion for properly roasted, single origin coffee.
Once again, my palate returned to coffee, but finding a decently roasted coffee in Vancouver BC was harder than I thought. Given that this was the “West Coast”, I was discouraged how difficult it was to find good quality Arabica beans that weren’t over roasted. I stumbled across a few small roasters that did an excellent job, but in time they modified their roasts for “local tastes”, so once again, I was back looking for a new roaster. On a few occasions, I ordered from La Vieille Europe in Montreal because in the 40 or 50 years they have been in business, they never lost their passion for properly roasted, single origin coffee. Over the 20 years I have lived in Vancouver, I discovered the world of quality tea that is largely unknown to most non-Asian born Chinese. There was one excellent tea importer in the Chinatown that I knew of and one that is still in the Richmond Public market that have single origin estate teas that rival the diversity of the best coffee roaster. Over the past 20 years, I’ve explored different types of tea from China and have come to like a few; my favourite of which is a fermented tea known as Pu-ehr.
Over the 20 years I have lived in Vancouver, I discovered the world of quality tea that is largely unknown to most non-Asian born Chinese. There was one excellent tea importer in the Chinatown that I knew of and one that is still in the Richmond Public market that have single origin estate teas that rival the diversity of the best coffee roaster. Over the past 20 years, I’ve explored different types of tea from China and have come to like a few; my favourite of which is a fermented tea known as Pu-ehr. At the beginning of this year, I began to explore green teas from Japan when I discovered Hibiki-An, an online tea importer from Uji region of Kyoto. My culinary world expanded once again.
At the beginning of this year, I began to explore green teas from Japan when I discovered Hibiki-An, an online tea importer from Uji region of Kyoto. My culinary world expanded once again. For the purpose of “cooling” the water to just the right temperature, there is a yuzamashi — which is a small ceramic cup with a spout that the boiled water gets poured into to cool momentarily before being poured into the kyuzu; a special tea pot with a single handle, built in mesh filter and large opening for the water (see photo, above).
For the purpose of “cooling” the water to just the right temperature, there is a yuzamashi — which is a small ceramic cup with a spout that the boiled water gets poured into to cool momentarily before being poured into the kyuzu; a special tea pot with a single handle, built in mesh filter and large opening for the water (see photo, above).
 The colour was a bright jade green and the taste had no hint of bitterness whatsoever!
The colour was a bright jade green and the taste had no hint of bitterness whatsoever!