I was eating low carb for a year and following that, eating keto for 1.5 years, and for the past 6 months I’ve been in partial remission of my type 2 diabetes (with HbA1C significantly ≤ 6.5%). Two weeks ago my fasting blood sugar (FBG) was assessed at the lab as being 5.2 mmol/L (94 mg/dl), so for all intents and purposes, it is though I am not diabetic (normal HbA1C and normal FBG). My blood pressure too is totally normal (120/70) — which is a huge drop from the hypertensive emergency level that started me on my “journey” March 5, 2017. I feel well and I look well and provided I continue to eat a very low carbohydrate diet, I am well. But this past weekend, I had conclusive evidence that I am NOT cured of my type 2 diabetes!
Sunday I was invited over to a friend’s house for a holiday party and I decided for the first time in as many years to eat “off plan”; not that I haven’t had the odd taste of something , but I’ve not had an off-plan meal in two and a half years. This past Sunday, I did. I didn’t go crazy — certainly not as when compared with all of the goodies I would eat at special events in the past. I had a few homemade falafel balls, 1/2 a potato pancake and 1/2 a freshly made donut, and the rest of what I ate was baked salmon, low carb veggies and club soda.
Naturally, I expected my blood sugar to be elevated afterwards, but an hour later it was 11.3 mmol/L (204 mg/dl)!! That is the above the 10.0 mmol/L (180 mg/dl) blood sugar level cutoff where the body excretes the excess sugar in the urine (called glucosuria). I was clearly still very diabetic (i.e. not cured).
I had some Metformin in the house and took one tablet and also did 20 slow squats in order to coax my muscles to accepting the excess blood sugar. An hour later my blood glucose was 8.6 mmol/L (155 mg/dl); still very much above the so-called “ideal” of 7.8 mmol/L upper cut-off for someone with type 2 diabetes. An hour later my blood sugar was 6.8 mmol/L (123 mg/dl). Dejected, I went to bed.
I woke up 3 hours later to use the washroom (not surprising given my body was trying to get rid of so much excess sugar!!) and I decided to test my blood sugar one more time to see what it went down to. It was 4.1 mmol/L (74 mg/dl)) — which is usually what it is after a day-long fast. To be sure, I checked the result 3 times. Surprisingly, I was still producing small amounts of ketones 0.3 mmol. It was evident was that my muscle (as a bi-product of my significant weight loss (50 pounds) and encouraged by the squats) and my liver (also a bi-product of my significant weight loss and encouraged by the Metformin*) accepted the excessively high sugar load and the rest left via my urine. This is certainly a MUCH better response than I had to eating carbs 2 – 1/2 years ago, but by no means am I “cured”. I am still a person with type 2 diabetes, just in remission.
*the Metformin helped suppress the breakdown of fat from my fat cells (lipolysis) and the resulting release of glycerol, since I had all that sugar to use. I also helped promote glycogen storage.
Despite having had type 2 diabetes for 8 years prior to adopting a low carb lifestyle, I did have a first-phase insulin response to eating all those carbs, but it was clearly inadequate. I did have a second phase insulin response, but having been eating only low carb, my pancreas was not used to such a huge sugar load. It was ill-prepared. As a result, my blood sugar hit glucosuria levels (above 10 mmol/L), resulting in my body dumping excess sugar in my urine.
It’s hard to know what my first phase and second phase insulin response would have been had a eaten 100 or so grams of carbs for 3 sequential days before eating this huge carb load, in order to prepare my pancreas (i.e. this is what is encouraged for those eating low carb before having an oral glucose tolerance (OGTT) test).
It’s also hard to know how much of the improved insulin sensitivity was due to my significant weight loss and resistance exercise that I am doing and how much was due to the Metformin I took, but I have NO desire to repeat this experiment without the Metformin, in the interest of science! In fact, I am VERY content to go back to eating “on-plan” and letting my body recover from the excessively high carb load I gave it. The harsh reality is I am not cured. I still have type 2 diabetes. I am just in remission, provided I continue to eat a very low carb diet.
I’ve been in partial remission of type 2 diabetes for about 6 months now, but I have clearly not reversed (cured) it. For an explanation of the difference between partial-, complete- or prolonged-remission and reversal / cured, please click here). As discussed in that article, remission of type 2 diabetes can occur with weight loss of ≥ 15 kg (33 pounds) which either results in restoration of β-cell function by either (a) β-cells being reactivated or (b) by existing β-cells functioning better and this is what I’m experiencing. I am in partial remission (using Virta Health’s definition) as my HbA1C < 6.5% using only occasional Metformin, and my fasting blood glucose ≤ 5.5 mmol/l (100 mg/dl).
Diabetes reversal (i.e. being “cured”) is where a person no longer has the symptoms of type 2 diabetes (which has been documented to occur), but is clearly not my case! I am still very much diabetic. But I don’t have any symptoms, provided I continue to eat a very low carbohydrate diet.
Some final thoughts…
Critics of a very low carb / ketogenic diet say that it is “not sustainable”, but when the option for me of not eating this way is to have responses as above, eating real, whole food (instead of refined, prepared foods) is very sustainable! Have a look at some of my articles about what I eat, my posts on Instagram and my recipe tab, you’ll see that I am not suffering!
Those who have been following my “journey” from the beginning know that I had two girlfriends who worked in healthcare die (one of a heart attack and one of a stroke) before I faced my own health crisis in March 2017. I changed March 5th of that year and have not looked back. I do it for me. I do it for my young adult sons. I do it for Kim and Jane who didn’t get the opportunity to change their lifestyle before dying prematurely.
We’ll hear people who advise others to do something “as if their life depended on it” and for me, eating this way is just that. My life (via cardiovascular health) and my quality of life (having my vision, all my toes, etc.) depends on it. It’s all a matter of motivation and that is mine.
What’s yours?
Perhaps you want to lose weight for health reasons, or for aesthetic reasons or to eat less carbs to bring down high blood sugar or lower a risk that you know runs in your family. Whatever your reasons are, I can support you in accomplishing your goals.
More Info?
If you would like more information about the services I offer, please have a look under the Services tab or in the Shop for more information. If you have service-related questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
The American Diabetes Association (ADA) has just released its new Standards of Medical Care in Diabetes (2020) [1] which once again includes a low carbohydrate diet. The section on Medical Nutrition Therapy begins by referring to the ADA’s April 2019 Consensus Report[2] which emphasized that there is no ”one-size-fits-all” eating pattern for the prevention or management of diabetes (more in this article).
In the section on Medical Nutrition Therapy (MNT), the new Standards of Medical Care 2020 underscores that for many people with diabetes, the most challenging part about treatment is determining what to eat — and for this reason the ADA emphasizes that meal planning needs to be individualized.
The ADA also states that all people diagnosed with diabetes should be referred to an a Registered Dietitian (RD/RDN) who is “knowledgeable and skilled in providing diabetes-specific MNT at diagnosis and as needed throughout the life span”[1] and that research indicates that Medical Nutrition Therapy delivered by an RD/RDN is associated with decrease in HbA1C of between 0.3 and 2.0% for people with type 2 diabetes [3].
In the section on Eating Patterns, Macronutrient Distribution and Meal Planning, the new Standards of Medical Care in Diabetes re-iterated what the Consensus Report stated, that evidence suggests that;
“there is not an ideal percentage of calories from carbohydrate, protein, and fat for people with diabetes. Therefore, macronutrient distribution should be based on an individualized assessment of current eating patterns, preferences, and metabolic goals.”
As well, the new Standards of Medical Care re-iterates that a low carbohydrate eating pattern is an example of one that is both healthful and helpful in controlling blood glucose;
“The Mediterranean-style ([4-5], low-carbohydrate* [6-8] and vegetarian or plant-based [9-10] eating patterns are all examples of healthful eating patterns that have shown positive results in research, but individualized meal planning should focus on personal preferences, needs, and goals. “
*In the Consensus Report referred to in this section, a low carbohydrate eating pattern was defined as 26-45% of total calories from carbohydrate and a very low carbohydrate eating pattern (ketogenic) was defined as 20-50 g of non-fiber carbohydrate per day.
The new Standards of Medical Care encourages healthcare practitioners to not only consider a person’s metabolic goals, but also their personal preferences, including tradition, culture, religion, health beliefs, goals, and economic situation in helping them choose a suitable eating patterns.
It encourages each member of the healthcare team;
“to be knowledgeable about nutrition therapy principles for people with all types of diabetes and be supportive of their implementation.”
Given that a low carbohydrate diet is one of the eating patterns that the ADA considers both healthful and helpful in the management of diabetes, healthcare professionals ought to be prepared to be supportive of a person seeking to implement this approach.
The Standards of Medical Care states that until there is stronger evidence surrounding comparative benefits of different eating patterns in specific individuals, “healthcare providers should focus on the key factors that are common among the patterns:
1) emphasize non-starchy vegetables
2) minimize added sugars and refined grains
and
3) choose whole foods over highly processed foods to the extent possible”[2].
Similar to what was stated in the Consensus Report, the Standards of Medical Care reiterates that “research studies on some low-carbohydrate eating plans generally indicate challenges with long-term sustainability, it is important to reassess and individualize meal plan guidance regularly for those interested in this approach”. Given the wide range of “low carbohydrate” diets people may be following, it makes good sense to ensure a person is following one that is evidence-based and appropriate for them.
The Standards of Medical Care restates that at this time a low carbohydrate eating pattern is notrecommended for women who are pregnant or lactating, people with or at risk for disordered eating, or people who have renal disease, and should be used with caution in patients taking sodium—glucose cotransporter 2 inhibitors due to the potential risk of ketoacidosis [11-12]. (Note: This caution regarding those taking certain medication is covered in this previous article).
Carbohydrates
The section of the Standards of Medical Care in Diabetes on Carbohydrates re-emphasizes the benefits to blood sugar (glycemic) control of a low carbohydrate eating patterns that was previously outlined in the Consensus Report, namely;
“For people with type 2 diabetes or prediabetes, low-carbohydrate eating plans show potential to improve glycemia and lipid outcomes for up to 1 year [6, 8, 13, 14-17]
The new Standards re-iterates that “part of the challenge in interpreting low-carbohydrate research has been due to the wide range of definitions for a low-carbohydrate eating plan [8, 18]”.
Final Thoughts…
There is nothing really “new” in the section on Medical Nutrition Therapy in the new Standards of Medical Care as it pertains to the safety and efficacy of low carbohydrate eating patterns, or in their ability to help improve blood sugar control. This, in and by itself is very encouraging because it means that the ADA has considers a well-designed low carbohydrate diet to be both healthful and helpful in the management of diabetes for the second year in a row.
When will Diabetes Canada complete their review of the current literature, including that cited by the ADA in the Consensus Report and their new Standards of Medical Care in Diabetes 2020 and update their position on the use of low carbohydrate diets in those with diabetes in Canada?
More Info
If you would like more information about the services I provide and how I can design a Meal Plan for you based on your needs, please have a look under the Services tab, or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
American Diabetes Association, Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes—2020
American, Diabetes Care Jan 2020, 43 (Supplement 1) S48-S65; DOI: 10.2337/dc20-S005
EvertAB, DennisonM, GardnerCD, et al. Nutrition therapy for adults with diabetes or prediabetes: a consensus report. Diabetes Care2019;42:731—754
Franz MJ, MacLeod J, Evert A, et al. Academy of Nutrition and Dietetics nutrition practice guideline for type 1 and type 2 diabetes in adults: systematic review of evidence for medical nutrition therapy effectiveness and recommendations for integration into the nutrition care process. J Acad Nutr Diet 2017;117:1659—167
Esposito K, Maiorino MI, Ciotola M, et al. Effects of a Mediterranean-style diet on the need for antihyperglycemic drug therapy in patients with newly diagnosed type 2 diabetes: a randomized trial. Ann Intern Med 2009;151:306—314
Sainsbury E, Kizirian NV, Partridge SR, Gill T, Colagiuri S, Gibson AA. Effect of dietary carbohydrate restriction on glycemic control in adults with diabetes: a systematic review and meta-analysis. Diabetes Res Clin Pract 2018;139:239—252
van Zuuren EJ, Fedorowicz Z, Kuijpers T, Pijl H. Effects of low-carbohydrate- compared with low-fat-diet interventions on metabolic control in people with type 2 diabetes: a systematic review including GRADE assessments. Am J Clin Nutr 2018;108:300—331
Snorgaard O, Poulsen GM, Andersen HK, Astrup A. Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes. BMJ Open Diabetes Res Care 2017;5:e000354
Rinaldi S, Campbell EE, Fournier J, O’Connor C, Madill J. A comprehensive review of the literature supporting recommendations from the Canadian Diabetes Association for the use of a plant-based diet for management of
Pawlak R. Vegetarian diets in the prevention and management of diabetes and its complications. Diabetes Spectr 2017;30:82—88
U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA revises labels of SGLT2 inhibitors for diabetes to include warnings about too much acid in the blood and serious urinary tract infections. Accessed 1 November 2019. Available from http://www.fda.gov/Drugs/DrugSafety/ucm475463.htm
Blau JE, Tella SH, Taylor SI, Rother KI. Ketoacidosis associated with SGLT2 inhibitor treatment: analysis of FAERS data. Diabetes Metab Res Rev 2017;33:e2924
Saslow LR, Daubenmier JJ, Moskowitz JT, et al. Twelve-month outcomes of a randomized trial of a moderate-carbohydrate versus very low-carbohydrate diet in overweight adults with type 2 diabetes mellitus or prediabetes. Nutr Diabetes 2017;7:304
Hallberg SJ, McKenzie AL, Williams PT, et al. Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: an open-label, non-randomized, controlled study. Diabetes Ther 2018;9:583—612
van Wyk HJ, Davis RE, Davies JS. A critical review of low-carbohydrate diets in people with type 2 diabetes. Diabet Med 2016;33:148—157
Meng Y, Bai H, Wang S, Li Z, Wang Q, Chen L. Efficacy of low carbohydrate diet for type 2 diabetes mellitus management: a systematic review and meta-analysis of randomized controlled trials. Diabetes Res Clin Pract 2017;131:124—131
Tay J, Luscombe-Marsh ND, Thompson CH, et al. Comparison of low- and high-carbohydrate diets for type 2 diabetes management: a randomized trial. Am J Clin Nutr 2015;102:780—790
Thomas D, Elliott EJ. Low glycaemic index, or low glycaemic load, diets for diabetes mellitus. Cochrane Database Syst Rev 2009;1:CD006296
This souffle recipe is posted as a courtesy to those following a variety of low-carb and ketogenic diets (not necessarily Meal Plans designed by me). This recipe may or may not be appropriate for you.
Keto Spinach Souffle
When I was in my early teens, one of my favourite convenience foods was Stouffer’s® Spinach Souffle. I’m unsure whether it was discontinued or may still be available in eastern Canada, but it’s not in stores in Vancouver.
Stouffer’s® web page lists the ingredients in their Spinach Souffle as spinach, skim milk, eggs, water, soybean oil, modified tapioca starch, 2% or less bleached wheat flour, sugar, salt, and spice.
My keto version of Spinach Souffle uses spinach, whole eggs and egg whites, heavy cream, a touch of Parmesan, freshly ground salt and pepper and that’s it! There are no industrial seed oils, no flour and no sugar.
Here’s my recipe. It is delicious as a vegetarian main course along with a spring green salad, or as a side dish to your favourite main.
Enjoy!
Keto Spinach Souffle as a vegetarian main course
Ingredients
6 large eggs
4 egg whites
2 cups (500 ml) heavy whipping cream
1/2 cup (50 g) Parmesan cheese, grated
2 x 300 g frozen chopped spinach (total 3 cups), defrosted and squeezed dry
Instructions
Preheat convection oven with fan on to 400 °F (204 °C).
Grease the sides and the bottom of an oval Pyrex dish with butter (or use non-stick spray)
In a deep bowl, crack the eggs and beat well with a fork, then add the egg whites, and beat some more. Add the heavy whipping cream and mix well.
Squeeze the defrosted spinach well until it is as dry as possible, then add it to the bowl with the eggs, cream and Parmesan*. Season well with freshly ground salt and pepper.
When the oven is preheated, fill the Pyrex dish with the egg mixture and bake at 400 °F (204 °C) for one hour (or until nicely browned and well risen.
* for those sensitive to oxalates, blanching the spinach in boiling water and then shocking it in an ice bath before squeezing it dry will significantly lower the oxalate content. A 2005 study found that boiling high oxalate vegetables can reduce oxalates by as much as 87% (J. Agric. Food Chem.2005, 53, 8, 3027-3030, https://doi.org/10.1021/jf048128d)
Serve and enjoy!
from Cronometer
If you would like more information about the services I provide please have a look under the Services tab. If you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
Many people say they plan to lose weight, lower their blood sugar, pressure or cholesterol in the New Year, but the difference between a “wish” and a “resolution” is having a plan in place to actually do it.
Wish or Resolution?
A “wish” is really just a hope that something will occur — an “it would be nice” type of thought, whereas a “resolution” is a firm decision to do something and is associated with specific qualities that will make it a reality. A resolution is a SMART goal; one which is specific, measurable, achievable, realistic and timely.
A goal to lose weight or eat healthier isn’t specific — it’s just a wish. A resolution to stop eating foods with added sugar is specific, so is a goal to eat whole, real foods that are low in refined carbohydrate. These are specific.
A resolution isl measurable. It decides what success looks like. For someone to say they want to lose 25 pounds is very different than to say they plan to lose a pound a week so that in 6 months they’ve lost 25 pounds.
But is that goal achievable? If someone is significantly overweight, it is achievable to set a goal of losing 25 pounds in 6 months.
What if someone wants to incorporate long periods of intermittent fasting into their lifestyle, but also eat all of their meals with their family? This isn’t realistic — but they can choose to have shorter ‘eating windows’ (such as 18:6), intermittently fast each day and still eat dinner each night with their family. That’s entirely realistic.
For a goal to be timely(or time-bound) means that it will also be achieved in a specific amount of time. So, for example, the resolution to lose 25 pounds in 6 months, is time-bound.
So, while there are lots of people saying they’d like to lose weight, eat healthier, exercise more or have better blood sugar, blood pressure or cholesterol in the New Year, to be successful one needs a go about putting a SMART plan in place now in order to achieve it.
Without such a plan, January will arrive and a week into the New Year, 50% of people will have already given up on their goal [1] and by the end of the month, 83% will have quit [1]. Those are pretty discouraging statistics!
Why is that?
Because it takes ~66 days (more than 2 months) for a habit to become ingrained [2], so having professional support during that critical time is important!
I can help you get off to a good start in achieving your New Year’s resolution, but the best time to put a plan in place is now — before all the festivities begin.
Why not make this the year you actually achieve your health and weight-loss goals?
If you would like more information about the services I provide and how I can design a Meal Plan for you based on your needs, please have a look under the Services tab, or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Norcross, JC et al, Auld lang syne: success predictors, change processes, and self-reported outcomes of New Year’s resolvers and nonresolvers. J Clin Psychol. 2002 Apr;58(4):397-405
Lally, P., van Jaarsveld, C. H. M., Potts, H. W. W. and Wardle, J. (2010), How are habits formed: Modelling habit formation in the real world. Eur. J. Soc. Psychol., 40: 998—1009.
This recipe is posted as a courtesy to those following a variety of low-carb and ketogenic diets (not necessarily Meal Plans designed by me). This recipe may or may not be appropriate for you.
Blueberry-topped New York Style cheesecake is a classic and was easy enough to create by adapting my Keto Marble New York Cheesecake recipe (which is an 8″ one, and bakes in a counter-top convection oven). It can just as easily be made into a 10″ cheesecake by following the amount of cream cheese and egg and egg yolk in my New York Chocolate Cheesecake and baked either in a counter-top oven, if it is large enough or in a conventional oven.
Unless I am expecting more than a couple of people, I make the smaller one, because for me, “desserts” are a fare treat. A larger one would mean I would be enjoying it over several days, which may not be in my best interest, weight-wise.
Low Carb Blueberry Cheesecake
Low Carb Blueberry Cheesecake
Ingredients
Three 250 g (8 oz) pkgs cream cheese, room temperature
1/4 cup (60 ml) Truvia® (can use Swerve®, if preferred)
1/8 tsp salt
1/2 tsp real vanilla extract
3 large eggs, plus one egg yolk, room temperature
Blueberry Glaze
1 1/2 cups frozen blueberries
1 tbsp lemon juice,
1/4 cup low carb sweetener (I used Krisda Monk Fruit, granulated)
1.5 tsp tapioca starch, 2 tsp water
Instructions
Preheat the counter-top convection oven to 450 F. Make sure the fan on the oven is set to on’.
Prepare an 7 ” non-stick spring-form pan by lining with parchment paper and spraying well with a coconut oil spray.
In the bowl of a stand mixer using the flat paddle (or by hand) beat the packages of cream cheese one at a time until very well blended and add the eggs one at a time, continuing to blend. Don’t over mix once the eggs are added or the cheese cake may get a large crack as it cools.
Add the egg yolk, then the salt, Truvia® (or Swerve®) and some real vanilla, and complete the stirring by hand, using a spatula.
Have a pan that fits in the convection oven and that can be filled with water (for a water bath) and that can hold the springform pan. Pour the batter into the prepared springform pan and shake it gently to flatten the top.
Bake at 450 F for 12 minutes, then lower the heat to 200 F and make for another 35 minutes. Check during the last 5 minutes so as not to over-bake it.
While it is baking, prepare the blueberry glaze by putting the defrosted frozen blueberries, lemon juice and sweetener into a saucepan and heat over medium high heat while stirring. When it comes to a gentle boil, thicken with tabioca starch mixture and keep stirring until it is clear, shiny and thickened. Set aside until the cheese cake finishes baking.
When the cheesecake is done. remove it from the oven and top with blueberry glaze, then move it to a draft-free location to completely cool.
Transfer to the fridge to cool completely (best to cool overnight or two days ahead of time so the flavours fully develop).
Enjoy!
Based on 1/12 of the cheesecake, the macronutrient content is as follows;
The whole matter of ‘when we eat’ meals and ‘when we don’t eat’ was historically a non-issue; we ate when it was daylight and we had food available, and we didn’t eat when it was dark or had no food. With the creation of indoor lighting and electricity, “day” lasted as long as we keep the lights on and for most of us, food is available in our fridges around the clock. Before elaborating on the current science surrounding when to eat meals and to not eat, let’s look at a short history of the origins of eating 3 meals per day, and when the idea of ‘snacks’ became prominent.
Timing of Meals
According to food historian Ivan Day[1], during the Middle Ages, availability of daylight shaped meal times, as there was no electricity. People got up and began to work in the fields at first daylight and by mid-day they were hungry after working for 6 hours or so and lunch was the first and main meal of the day. As there was no artificial lighting, cooking large meals in the evening simply wasn’t possible, so dinner was really a smaller meal, such as bread and cheese.
Breakfast became popular during the mid-19th century when labourers needed an early meal to sustain them at work. It became widely popularized in the early 20th century when John Harvey Kellogg invented the first breakfast cereal. Dinner became the main meal of the day with the creation of artificial (gas) lighting, and by the early 1900s, people were eating 3 meals per day, with the last meal occurring after work. Gas lighting was expensive to run, so after dinner was eaten and cleaned up from, bedtime was shortly after.
Snacks
“Snacks” were frowned upon by the middle class during Victorian era because they did not require use of “proper” utensils (cutlery, plates), were seen as unhygienic and were associated with the lower class [2].
Snacks as we know them took root in the 1950s due to the manufacturing industry’s drive to sell new products in a growing economy after the end of WWII, along with an ability to create inexpensive disposable packaging and unique labelling to market these products. Sale of snack foods escalated in the late 1970s [2], and between 1977 and 2006, Americans were eating approximately 570 calories more per day, much of it as snacks rather than during meals [3].
Historic Dietary Treatment of Diabetes
Before the discovery of insulin, successful management of diabetes involved restricting carbohydrates eaten at meals.
In his text book titled “The Principles and Practice of Medicine” (1892), Dr. William Osler recommended a diet of 65% fat, 32% protein, and 3% carbohydrate, as well as abstaining from ”all fruits and garden stuff.” [4] — not dissimilar to some of the high-fat “keto” diets available today.
In the early 1900s, Bernard Naunyn encouraged a strict carbohydrate-free diet [5], with energy being provided as fat and protein.
In 1914, Dr. Frederick M. Allen treated people for several days with a period of fasting to clear the excess blood sugar via the urine, and then followed that with a diet that was mostly fat and protein, with a small amount of carbohydrates, mostly as vegetables â [6].
Dr. Elliot P. Joslin was the first doctor in the United States to specialize in treating diabetes, and in 1916 adopted the same low-carbohydrate approach as Fredrick Allen [7].
Medications as Treatment in Diabetes
Type 1 Diabetes
The discovery of insulin by Dr. Fredrick Banting and Dr. Charles Best in 1921 provided life-saving therapy for those with type 1 diabetes (which results from failure of the insulin-producing β-cells of the pancreas). The insulin was initially isolated from the pancreases of beef and pigs, but “human insulin” became possible in the 1980s due to recombinant DNA technology which enabled the development of both basal insulin, as well as rapid acting insulin. This was life-changing and life-saving to those with type 1 diabetes.
Type 2 Diabetes
Metformin initially became available as a first-line treatment for type 2 diabetes in the late 1990s, and enabled those with type 2 to better control their blood sugar levels along with dietary changes — but when people were unable, or unwilling to adequately limit carbohydrate intake, insulin was prescribed.
Insulin went from being a life-saving therapy for those with type 1 diabetes to also being a ‘treatment’ for people with type 2 diabetes who ate what they wanted at meals and snacks and “covered it with insulin“. The problem is that this type of “liberalization” of the diet creates a “vicious cycle” for those with type 2 diabetes, described as follows in a new study published ahead of print in September 2019, and to appear in the December 2019 journal, Diabetes Care[8];
“Dietary intervention is usually accompanied by sequential addition of several anti-hyperglycemic agents, including glucagon-like peptide 1 (GLP-1) analogs and sodium—glucose cotransporter 2 (SGLT2) inhibitors. Despite this medical treatment, many patients require insulin therapy, which is gradually augmented according to the glucose target-driven strategy. However, this progressive increase in insulin dose often leads to weight gain, which may increase insulin resistance, leading to a vicious cycle further increasing insulin doses, continued weight gain, decreased likelihood of achieving glycemic targets, a high risk for diabetes complications and increased insulin dose-dependent cardiovascular risk and mortality. It is, therefore, important to prevent the weight gain when insulin treatment is required.”
Of course, medications such as biguanides, sulfonylureas, SLP-1 analogues and SGLT2 inhibitors are very important tools for doctors to add in helping manage blood sugar levels, but too often they are used instead of / in the absence of carbohydrate reducing dietary changes and this results diabetes becomes “a chronic, progressive disease“. It need not be so if people are willing to reduce their carbohydrate intake and time when they do eat some carbohydrate-containing food, in accordance with when their body handles them best.
Dietary Recommendations – meals and snacks
Since 2009, people with type 2 diabetes have been advised to eat 3 meals per day plus several snacks per day â — with carbohydrates evenly distributed across the meals and snacks, in order to achieve the best weight management and blood sugar control [9-11]. They’ve been told to aim for between 45-60 grams of carbohydrate at each meal, and 15-20 grams of carbohydrate for each of 3 daily snacks (between breakfast and lunch, between lunch and dinner, and before bed). Surprisingly, the new study referred to above that will appear in the December 2019 issue of Diabetes Care states that there were no research studies to support these practices [8].
The 45-60 g of carbs for each of 3 meals per day and 15-20 g per snack distribution is still being recommended as goals to those with type 2 diabetes — resulting in between 190 -240 g of carbohydrate being eaten each day. That is a lot of carbohydrate for people who’s bodies can no longer handle that much. Presumably the snacks are to lower the risk of hypoglycemia (low blood sugar) that can result from the anti-hyperglycemic medications that have become necessary to prescribe because these people do not restrict carbohydrate and as a result have blood sugar levels that are too high.
Most concerning is that recent studies have found that snacks consumed later in the day have been associated with an increased risk of obesity and type 2 diabetes, with higher overall blood sugar and higher glycated hemoglobin (HbA1C) [12-13]. These are some of the “costs” of people being told to eat an afternoon and evening snack in order to avoid low blood sugar that can result from taking medication to lower blood glucose, and in an absence of being willing to reduce carbohydrate intake.
Would it not make far more sense to encourage people with type 2 diabetes to eat less carbs and eat less often — along with doctors de-prescribing anti-hyperglycemic medication, including insulin? That way, no snacks are needed to keep them from having low blood sugar and their average blood sugar levels can fall.
In fact, a soon-to-be-published pilot study [8] found that those with type 2 diabetes who ate the same calories each day as 3-meals per day, rather than as 6 meals per day [i.e. 3 meals and 3 snacks] reduced body weight, blood glucose, and insulin doses! Without even changing how many carbs they ate or how many calories they ate, in just 12 weeks, the subjects in the 3 meal per day group, lost on average 12 pounds (5.4 kg) more than those in the 6 meal per day group, had 1.2% lower HbA1C than the 6 meal per day group and their total daily insulin dose was reduced by 26 units ± 7 (with no reduction in the 6 meal per day group). On top of this, this study found that “there was a significant decrease in hunger and cravings only in the 3 meal per day group“. This makes sense of course, because they were able to lower their injected insulin, which drives hunger and fat storage, leading to weight gain. The mechanism was thought to be an up-regulation in the clock genes of those that ate 3 meals per day, which contributed to the improved glucose metabolism.
Note: it’s important to keep in mind that it is the eating of carbohydrate-containing food that triggers the release of insulin from our pancreas, so even in healthy people i.e. those who are not diabetic, eating the same amount of food as 3 meals per day with no snacks (versus 3 meals plus 3 snacks) will result in less insulin being released. Less insulin means less hunger and less fat storage — whether it is the natural insulin from our own pancreas or it is injected insulin. If our goal is weight management, eating the same amount of food as 3 meals, rather than as meals and snacks makes sense.
This study verified that when we eat and when we don’t eat matters a great deal because our body has evolved over hundreds of thousands of years to function in response to light and day cycles, called circadian rhythms.
When We Eat – especially which meals to eat carbs
Chronobiology is the study of the effect of time of day on living systems and is emerging as an important player in human health.
We now know that the body’s processes involved in the maintaining of blood sugar control such as β-cell function, glucose uptake by the muscles, and glucose production by the liver, are all under the control of circadian rhythms. The body’s “master clock” which controls these circadian rhythms is found in a part of the hypothalamus of our brain, called the suprachiasmatic nucleus (SCN) and is “set” by exposure to light.
Note: Historically, the only light that set the SCN was sunlight, but our increasing exposure to bright lights emanating from office- and store- lights, TVs, computers and smart phones has disrupted this once tightly regulated system.
Similar “peripheral clocks” are found in our body’s tissues, including muscle cells, liver cells, β-cells of our pancreas which produce and release insulin, and fat cells (adipose), and these are controlled by the “master clock” in our SCN, and by when we eat [14,15].
As it turns out, our circadian rhythms are optimized for us to eat during periods of light (daytime), and to fast and sleep in periods of dark (night time) [16,17] — so fasting after supper and overnight is consistent with our body’s built-in circadian rhythms.
In addition, blood sugar control is not the same at all times of the day, but fluctuates according to our body’s circadian rhythms. It has been shown in both healthy individuals and those with type 2 diabetes that identical foods eaten in the afternoon and evening cause much higher elevations in blood sugar, compared with the same foods eaten in the morning [18-20] . Based on this, it makes the most sense for any major carbohydrate sources (milk, fruit, root vegetables etc.) that are going to be eaten during the day to be consumed at breakfast, rather than evenly distributed across the whole day and evening.
When We Don’t Eat – intermittent fasting
It has been shown for those with type 2 diabetes that fasting until noon time actually results in much higher after-meal blood sugar levels (postprandial hyperglycemia), as well as an impaired insulin response after lunch and dinner [21], so while it is currently popular for people to chose their “eating windows” based on a wide range of popular protocols, it seems to me that choosing them in a way that is consistent with our circadian rhythms makes the most sense — especially if the goal is weight loss, appetite control and blood sugar regulation.
More Info
If you would like more information about having me design a Meal Plan for you that arranges your eating times and non-eating times around your schedule and in accordance with your natural circadian rhythms, please have a look under the Services tab or in the Shop. If you have service-related questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
BBD News Magazine, Winterman, Denise, Breakfast, lunch and dinner; Have we always eaten them? Nov 15 2012, https://www.bbc.com/news/magazine-20243692
Carroll, Abigail (30 August 2013). “How Snacking Became Respectable”. Wall Street Journal. August 30, 2013, https://www.wsj.com/articles/how-snacking-became-respectable-1377906874
Duffey KJ, Popkin BM, Energy Density, Portion Size, and Eating Occasions: Contributions to Increased Energy Intake in the United States, 1977—2006, June 28, 2011, https://doi.org/10.1371/journal.pmed.100105
Osler W. The Principles and Practice of Medicine. New York, D. Appleton and Company, 1892
WoodyattRT, Bernhard Naunyn. Diabetes 1952;1:240—241, pmid:1493683
JoslinEP, Treatment of Diabetes Mellitus. 2nd ed.Philadelphia, Lea & Febiger, 1917, p. 409
Jakubowicz D, Landau Z, Tsameret S et al, Reduction in Glycated Hemoglobin and Daily Insulin Dose Alongside Circadian Clock Upregulation in Patients With Type 2 Diabetes Consuming a Three-Meal Diet: A Randomized Clinical Trial, Diabetes Care 2019 Dec; 42(12): 2171-180.https://doi.org/10.2337/dc19-1142
Seagle HM, Strain GW, Makris A, Reeves RS; American Dietetic Association. Position of the American Dietetic Association: weight management. J Am Diet Assoc 2009;109:330—346
Beyond the Basics: Meal Planning for Healthy Eating, Diabetes Prevention and Management. Canadian Diabetes Association, 2014.
Arnold L,MannJI, Ball MJ. Metabolic effects of alterations in meal frequency in type 2 diabetes. Diabetes Care 1997;20:1651—1654
Mekary RA, Giovannucci E, Willett WC, van Dam RM, Hu FB. Eating patterns and type 2 diabetes risk in men: breakfast omission, eating frequency, and snacking. Am J Clin Nutr 2012;95:1182—1189
Gouda M, Matsukawa M, Iijima H. Associations between eating habits and glycemic control and obesity in Japanese workers with type 2 diabetes mellitus. Diabetes Metab Syndr Obes 2018;11:647—658
Dyar KA, Ciciliot S, Wright LE, et al. Muscle insulin sensitivity and glucose metabolism are controlled by the intrinsic muscle clock. Mol Metab 2013;3:29—41
Sadacca LA, Lamia KA, deLemos AS, Blum B, Weitz CJ. An intrinsic circadian clock of the pancreas is required for normal insulin release and glucose homeostasis in mice. Diabetologia 2011;54:120—124
Poggiogalle E, Jamshed H, Peterson CM. Circadian regulation of glucose, lipid, and energy metabolisminhumans. Metabolism2018;84:11—27
Saad A, Dalla Man C, Nandy DK, et al. Diurnal pattern to insulin secretion and insulin action in healthy individuals. Diabetes 2012;61:2691—2700
Bo S, Fadda M, Castiglione A, et al. Is the timing of caloric intake associated with variation in diet-induced thermogenesis and in the metabolic
pattern? A randomized cross-over study. Int J Obes 2015;39:1689—1695
Jakubowicz D, BarneaM, Wainstein J, Froy O. High caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity (Silver Spring) 2013; 21:2504—2512
Morgan LM, Shi JW, Hampton SM, Frost G. Effect of meal timing and glycaemic index on glucose control and insulin secretion in healthy volunteers. Br J Nutr 2012;108:1286—1291
Jakubowicz D, Wainstein J, Ahren B, Landau Z, Bar-Dayan Y, Froy O. Fasting until noon triggers increased postprandial hyperglycemia and impaired
insulin response after lunch and dinner in individuals with type 2 diabetes: a randomized clinical trial. Diabetes Care 2015;38:1820—1826
Many people think that eating a low carb or ketogenic diet necessitates eating meat — in the same way that many assume that one needs to eat lots of added fat, but neither are true. In a previous article, I addressed the misconception that eating a low carb or keto diet is all about eating lots of extra fat and in this article, I will address the false belief that one has to be a meat-eater to follow a low-carb or ketogenic diet.
Before launching into the article, it’s important to define some terms.
Vegetarian versus Vegan
There is a significant difference between vegetarians and vegans and these two terms seem to get mixed up frequently. Vegans eat no animal products, while vegetarians don’t eat the meat of animals but will eat products that come from animals, such as dairy and eggs.
There are different categories of vegetarians, including ovo-lacto (those who eat eggs and milk-based products), as well as those that only eat one or the other (ovo or lacto). Some classify pescatarians who eat wild fish and seafood as a form of vegetarianism because they don’t eat farmed animals for food but for the purpose of this article I will use the term “vegetarian” to mean ovo-lacto vegetarian, as this is the most common form.
Different Motivations, Same Needs
Religious or cultural vegetarians
People are vegetarian for different reasons; some for religious reasons, including some Hindus, Buddhists, Jains, Sikhs and Seventh Day Adventists. Some people don’t eat meat for cultural reasons. For example, some people from India may not be religious themselves but don’t eat meat because they were not raised eating it or because others in their social circle don’t eat meat. I refer to these type as being culturally vegetarian. Finally, some don’t eat meat for ethical reasons — believing it is morally wrong to kill an animal to eat it.
From my perspective as a Dietitian, it is important that people who want to eat a low carb or ketogenic diet for health reasons are able to do even if they are vegetarian.
While type 2 diabetes is on the rise in those of various ethnic backgrounds, people of South Asian descent (those who have their roots in India, Pakistan, Sri Lanka, Bangladesh and Nepal) are thought to be at higher risk, and many people from these regions eat a vegetarian diet for religious or cultural reasons. Given what we now know about the association between a diet high in carbohydrate and both hyperinsulemia and type 2 diabetes (documented in many previous posts), offering people the option of eating a low carb or ketogenic vegetarian diet, enables them to obtain the same health benefit as those that choose to eat meat. And why not?
While many omnivores consider vegetarianism an ‘inferior diet’ it need not be so. A well-designed vegetarian or omnivore diet enables people to access all the essential macronutrients (essential fats and amino acids) from real, whole foods. This article will explains ‘how’, below.
Ethical VEGETARIANS
Oftentimes I find that people that choose vegetarianism for ethical reasons don’t realize that one can purchase ethically-raised meat and poultry. There are butchers in my area that raise their animals out back, where they are humanely treated their entire lives and killed humanely. These are a far cry from the industrial feed-lots that often motivate ethical vegetarians, and for understandable reasons. One place that I shop at has the motto “know your farmer, know your meat“. As well, some of the most ethical meat-eaters I know are hunters that train at the range to make sure that the animal they harvest doesn’t suffer, and they use the whole animal for food; from snout to tail. In fact, one local hunting group I’ve heard of is run in association with a local First Nations band that teach hunters that already have their Federal hunting licence to select animals in accordance with centuries-old First Nations principals for animal stewardship. One does not have to become a vegetarian for ethical reasons, as there are other options.
Defining a Low Carb or Keto Diet
Whether one is a vegetarian or a meat-eater, defining what “low carb” or “keto” is necessary in order to determine how one can eat this way.
As mentioned in a prior article, what makes a diet ”low carb” or ”ketogenic” is how much carbohydrate it has, not how much fat it contains. In the same way, what makes a diet low carb or ketogenic has nothing to do with how much meat one eats, or whether one eats meat at all.
Feinman et al [2] defined three categories of reduced-carbohydrate diets as follows;
(a) very low carbohydrate ketogenic*: carbs limited to 20—50 g per day or < 10% of total energy intake.
(b) low carbohydrate: carbs limited to < 130 g per day or < 26% of total energy intake.
(c) moderate carbohydrate: carbs limited to 130—225 g per day or 26—45% of total energy intake.
As covered in detail in this previous article, from a dietary perspective only protein and fat are essential in the diet. For a nutrient to be ”essential”, it is required to be eaten because the body can’t manufacture it.
There are 2 essential fats; linoleic acid, an omega 6 fat and alpha-linolenic acid, an omega 3 fat, and there are 9 essential amino acids. Amino acids are are the building blocks from which proteins are made.
For omnivores, getting all the essential nutrients is fairly straight forward and simply requires eating a wide range of meat and animal products, along with nuts and seeds, but for those who are ovo-lacto vegetarians, one needs to be more intentional to ensure getting all the essential nutrients.
The 2 essential fatty acids (linoleic and alpha-linolenic acid) can be easily obtained from eggs, nuts and seeds, but ensuring adequate intake of all 9 of the essential amino acids (histidine, isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, and valine from low carb, vegetarian sources can be achieves as follows [3];
Vegetarians following a low carb or ketogenic diet can obtain histidine from dairy foods such as milk and cheese, as well as from nuts, seeds and eggs.
Isoleucine can be obtained from eggs and cheese, as well as from seaweed and soy protein, if people wish.
Rich sources of leucine include milk, cheese and egg, as well as from pumpkin or squash seeds. It can also be obtained from tofu and legumes eaten in daily maximum 1/2 cup quantities (as they are a significant source of carbohydrates).
Lysine can be found in some cheeses such as Parmesan, eggs and spirulina as well as from tofu, and if needed can be supplemented with whey protein isolate and isolated soy protein.
Foods high in methionine include dairy of different types, cheese, eggs, and nuts, as well as soy and legumes.
High phenylalanine foods include cheese, nuts and seeds, eggs and dairy, as well as from soybeans and legumes.
Foods rich in threonine include cheese, nuts and seeds, and if desired, in soy, and in legumes and lentils (in maximum daily 1/2 cup servings as they are significant sources of carbs)
Good sources of tryptophan include egg, milk products such as yogurt, nuts and seeds and soy products, if eaten.
High valine foods include nuts and seeds, mushrooms, and soybeans if eaten, as well as legumes.
Note (Nov 8, 2019 @ 10 am): shortly after publishing this article, the topic of whether vegetarians can obtain sufficient vitamin B12 and the long chain fatty acids, DHA and EPA was raised on social media. While this article is about a vegetarian diet providing all the essential macronutrients, I will add the following information for those who are interested:
Re: vitamin B12: 2 cups of yogurt per day provides 100% DV of B12 and so do 4 eggs (which many low carb omnivores eat in a day). Add to that 3 oz of Swiss cheese which provides 100% DV, or a cup of tofu (which provides more than 100%), getting enough vitamin B12 is not an issue, provided vegetarians are not restrained by a “low fat” paradigm.
Re: the long chain fatty acids DHA and EPA: There is no Dietary Reference Intake (DRI) for EPA or DHA, only for alpha-linolenic acid. In healthy young men, approximately 8% of dietary alpha linolenic acid is converted to EPA and ≤4% alpha-linolenic acid is converted to docosahexaenoic acid (DHA). [Burdge GC, Jones AE, Wootton SA. Eicosapentaenoic and docosapentaenoic acids are the principal products of α-linolenic acid metabolism in young men. Br J Nutr. 2002;88(4):355-364].
In healthy young women, approximately 21% of dietary alpha-linolenic acid is converted to EPA and 9% is converted to DHA. [Burdge GC, Wootton SA. Conversion of α-linolenic acid to eicosapentaenoic, docosapentaenoic and docosahexaenoic acids in young women. Br J Nutr. 2002;88(4):411-420. ].
The better elongation in young women is related to the effects of estrogen. [Burdge G. α-Linolenic acid metabolism in men and women: nutritional and biological implications. Curr Opin Clin Nutr Metab Care. 2004;7(2):137-144, Giltay EJ, Gooren LJ, Toorians AW, Katan MB, Zock PL. Docosahexaenoic acid concentrations are higher in women than in men because of estrogenic effects. Am J Clin Nutr. 2004;80(5):1167-1174.]
For vegetarians, eating seaweed including nori, spirulina and other types of edible seaweed provides a good source of pre-formed DHA & EPA in the diet. These also form the basis for vegetarian-sourced DHA and EPA supplements that can be purchased.
Low Carb and Ketogenic Diets are Truly Not “One-Sized-Fits-All”
There really isn’t a “one-sized-fits-all” low carb or ketogenic diet!
There are the high fat / moderate protein varieties popularized by Dr. Jason Fung and that are often associated with high consumption of bacon, heavy whipping cream, and fatty meat, and offset by periods of intermittent fasting.
There is the higher protein lower fat approach during weight loss, followed by a moderate protein higher fat diet during weight maintenance of Dr. Stephen Phinney MD, PhD and Dr. Jeff Volek RD, PhD.
You can read more about the above two approaches in this article.
There are the higher lean protein type, with more grams of protein than grams of fat (popularized most recently by Dr. Ted Naiman in his P:E Diet and referred to in the previous article). More than likely, there are different macronutrient combinations than the ones listed here that are popular with others.
I don’t believe that any of the above can serve as a “one-sized-fits-all” approach because everybody’s nutritional needs and health conditions are different.
Those who are omnivore can choose a meal pattern that includes meat, and for those that are vegetarian (for whatever reason) can still reap the health benefits from eating a well-designed low carbohydrate diet that does not include meat.
Final thoughts…
It is my observation that many people who follow a low carb or ketogenic lifestyle tend to be overly loyal to their particular dietary style, which inadvertently makes people who need to or choose to eat differently feel that the health and metabolic benefits of following a low carb diet is not available to them.
People that don’t eat meat for religious, cultural or ethical reasons need to know there are options available for them to have a well-designed meal plan that includes the animal derived products they do eat, rather than to be told how ‘inadequate’ their diet is compared to those who eat meat.
More Info
If you would like more information about the services that I provide and how I can help design a Meal Plan based on your needs, please have a look under the Services tab, or in the Shop.
If you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Resources
Gujral UP, Pradeepa R, Weber MB, Narayan KM, Mohan V. Type 2 diabetes in South Asians: similarities and differences with white Caucasian and other populations. Ann N Y Acad Sci. 2013;1281(1):51—63. doi:10.1111/j.1749-6632.2012.06838.x
Feinman RD, Pogozelski WK, Astrup A, Bernstein RK, Fine EJ,Westman EC, et al. Dietary Carbohydrate Restriction as the First Approach in Diabetes Management: critical review and evidence base. Nutrition. 2015;31(1):1—13.
This article is about which protein foods are best for weight loss on a low carb or ketogenic diet, and builds on the previous article, where I outlined that what makes a diet ”low carb” or ”ketogenic” is how much carbohydrate it has, not how much fat it contains.
I’m not sure where the idea came from that eating a low carb or ketogenic diet for weight loss should include piles of bacon, bulletproof coffee, fathead pizza and ‘fat bombs’. Perhaps it originated with advocates of eating such a diet which is offset by extended periods of fasting, or by the use of the very term “low carb high fat” / “LCHF“, itself. As explained in the previous article, a low carb diet is higher in fat and protein, because the amount of carbohydrate is reduced — and this is necessary for the the body to be provided with adequate amounts of essential fats and essential amino acids (that make up protein) in order to function properly and make any glucose it needs.
Note: if you haven’t yet read the previous article, I’d highly recommend clicking here and reading it first, as it will help considerably with understanding this one.
As mentioned in the preceding article, some “LCHF” diets that target higher protein may be as high as 50-60% fat — which is considered “high fat” compared to the 30% of calories as fat recommended by previous and current food guides. Other some variations of a low carb diet that target protein may have considerably less fat; depending which protein foods are chosen, and whether fat containing foods that are not rich sources of protein (such as avocado and olives) are also included. In either case, a low carb or ketogenic diet that targets protein will have significantly less than the 75% calories as fat of the high fat versions. The fat eaten on a low carb or ketogenic diet which targets protein will come from fatty fish such as salmon, tuna, mackerel and sardine, the fat that exists in the lean portions of chicken, pork and steak, in egg and cheese, as well as in nuts and seeds, avocado and olives. What is (pardon the pun) essential is for people to ensure is that they eat foods that contain the two essential fats (linoleic acid, alpha-linolenic acid) and the nine essential amino acids (the building blocks of protein), including histidine, isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, and valine that the body can’t manufacture.
Combined List of Essential Nutrient-Containing Foods
In the previous article, I outlined which foods of animal origin and vegetarian origin are the best sources of each of these essential nutrients and that list should be referred to when selecting specific foods containing these, but combining those into one list, the following taken as a whole are good sources of the essential nutrients for those following a low carb or ketogenic diet:
pork
beef
lamb
chicken
turkey
fish, including tuna
shellfish
cheese, including Parmesan
nuts, including walnuts
pumpkin seeds and flax
eggs
soy protein
whey protein isolate
seaweed
tofu
legumes and lentils
spirulina
For those seeking weight loss, it makes good sense to choose foods with the most amount of protein for the least amount of energy (calories). Up until recently, figuring this out would have required lots of calculations, but Dr. Ted Naiman, a board-certified family medicine physician who practices at the Virginia Mason Medical Center in Seattle, Washington has made this easy. Along with William Shewfelt, Dr. Naiman recently published an online book titled The P:E Diet – Leverage Your Biology to Achieve Optimal Health.
Protein to energy (P:E) Ratio
“P:E” is simply the Protein to Energy ratio of a food and Dr. Naiman who is well known on social media for his excellent infographics makes choosing foods with the most amount of protein for the least amount of energy (calories) easy.
from The P:E Diet – Leverage Your Biology to Achieve Optimal Health, available at http://thepediet.com/
Referring to Dr. Naiman’s P:E ratio enables the sorting of the foods available on a low carb or ketogenic diet and which contain the essential nutrients, into those with the highest protein to energy ratio:
whey protein isolate
egg white
fish, including tuna
prawns
chicken breast
other poultry, including chicken legs, turkey, etc.
plain non-fat Greek yogurt
ground beef
pork
steak
whole eggs
soy protein
tofu
processed meat such as bacon
cheese, including Parmesan
lentils
milk
peanuts
beans / legumes
nuts
Calculations will still need to be done for other meats such as lamb and goat, and other types of seafood, but this list provides a good means to select foods that have the highest protein to energy ratio.
Low Carb and Ketogenic Diets Include a Range of Fat Intake
In the previous article, I mentioned how a well-designed low carb or ketogenic diet may have in the range of 50-60% calories as fat, but selecting foods with a higher protein to energy ratio (such as egg white and non-fat Greek yogurt) will provide less fat and few calories (energy) than choosing whole egg and Greek yogurt that is 5% fat. Doing this consistently will result in a significantly lower amount of fat yet it is still a low carb or ketogenic diet because of the low amount of carbohydrate it contains.
Use of a higher P:E ratio makes sense for those who are seeking to build muscle mass or to follow a protein-sparing modified fast type of diet. For this, there is Dr. Naiman’s book (link in the References and above). For those seeking simple weight loss, eating whole egg and slightly higher fat yogurt may provide more satiety (feeling of fullness), albeit with higher caloric intake. Since each person’s reasons for wanting to follow a low carb or ketogenic meal pattern is different, which specific protein foods are best to choose in what quantities will vary, person to person. There is no one-sized-fits-all low carb or ketogenic diet.
Final Thoughts…
People following a low carb or ketogenic meal pattern for weight loss and preserving muscle mass should target protein foods with an optimal P:E ratio for their needs, which will likely fall somewhere between the highest P:E ratio (5.0) and those in the 1.0-1.5 range.
Regular inclusion of high fat foods with relatively low protein such as bacon, bulletproof coffee, fathead pizza and fat bombs’ is neither required nor ideal if weight loss is being sought.
More Info
If you would like more information about the services that I provide and how I can help design a Meal Plan based on your needs, please have a look under the Services tab, or in the Shop.
If you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Reference
Naiman T, Shewfelt W, The P:E Diet – Leverage Your Biology to Achieve Optimal Health, http://thepediet.com/
Many people assume that a “low carb” or ketogenic (“keto”) diet for weight management and blood sugar reduction requires them to eat a diet high fat — piles of bacon, bulletproof coffee, fathead pizza and ‘fat bombs’, but this is not true. Not only is eating that way not ideal for many people seeking weight loss — but some actually end up gaining weight doing so.
In fact, what makes a diet “low carb” or “ketogenic” is how much carbohydrate it has, not how much fat it contains.
Defining Low Carb and Keto Diets
Different people define “low carb” or “keto” level of carbohydrates in different ways, but Feinman et al [1] defined three categories of reduced-carbohydrate diets as follows;
(a) very low carbohydrate ketogenic*: carbs limited to 20—50 g per day or < 10% of total energy intake.
Note: What makes a keto diet ketogenic is that that low carbohydrate intake puts people into a state of ketosis, which is a normal physiological state that people go into after an overnight fast. It is where the body burns stored fat for energy, releasing ketones which can be used by the brain and other tissues.
(b) low carbohydrate: carbs limited to < 130 g per day or < 26% of total energy intake.
(c) moderate carbohydrate: carbs limited to 130—225 g per day or 26—45% of total energy intake.
In my clinical practice and on other articles on this web page, I define “low carb” and “ketogenic” as Feinman et al did; with a low carb diet being one that is < 130 g per day and a ketogenic diet as one that is 20—50 g per day.
Protein, Fat and Carbohydrate — are all essential?
Many people assume that people need to eat all three macronutrients; protein fat and carbohydrate but from a dietary point of view, only protein (as specific amino acids) and fat are considered “essential” in the diet. For a nutrient to be “essential”, it is required to be eaten in food because the body can’t manufacture it.
There are two fats that are considered “essential”; linoleic acid (an omega 6 fat) and alpha-linolenic acid (an omega 3 fat). We need to eat meat and eggs and/or nuts and seeds for the major dietary sources of linoleic acid, as well as nuts such as walnuts and seeds such as flax to get rich sources of alpha-linolenic acid, although many people obtain these from eating chicken, cheese and whole milk [2].
Amino acids are the building blocks of protein, and there are nine amino acids that are considered “essential”; histidine, isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, and valine.
Below are the best low carb foods for obtaining each of these[3] are listed below.
The best sources of histidine include pork, beef, lamb, chicken, turkey, fish, dairy such as milk and cheese, nuts, seeds, eggs.
Best sources of isoleucine are eggs, turkey, chicken, lamb, cheese and fish and for vegetarians, soy protein and seaweed.
Rich sources of leucine include chicken, beef, pork, tuna, milk, cheese, and egg and for vegetarians tofu, legumes and pumpkin or squash seeds.
The best sources of lysine include red meat such as beef and lamb, pork, poultry, some cheeses such as Parmesan, certain fish such a cod and sardine, egg and whey protein isolate, and for vegetarians there is tofu, isolated soy protein and spirulina.
Foods high in methionine include , beef, lamb, cheese, turkey, pork, fish, shellfish, eggs, dairy and nuts, and for vegetarians, soy and legumes.
High phenylalanine foods include cheese, nuts and seeds, beef, lamb, chicken, pork, fish, eggs and dairy, and for vegetarians soybeans and legumes.
Foods rich in threonine foods include lean cuts of beef, pork, chicken, liver, cheese, shellfish, nuts, seeds, and for vegetarians, soy, legumes and lentils.
While many people associate turkey as being high in tryptophan, there are other foods as well. Tryptophan is required for the body to make the neurotransmitter serotonin, so getting enough tryptophan is…pardon the pun, essential. Good sources of tryptophan include salmon, all kinds of poultry (including turkey), egg, milk, nuts and seeds and for vegetarians, soy products.
High valine foods include cheese, beef, lamb, chicken, pork, nuts and seeds, and fish, and for vegetarians, soybeans, legumes and mushrooms.
Carbohydrate is Not Essential in the Diet
The Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids [4] which sets the standard for macronutrient consumption in both the US and Canada states;
”The lower limit of dietary carbohydrate compatible with life apparently is zero, provided that adequate amounts of protein and fat are consumed.
The lower limit of dietary carbohydrate
In short, there is no essential need for dietary carbohydrate provided that ”adequate amounts of protein and fat are consumed”. The reason carbohydrate is not essential is because the body can make what it needs from dietary protein and fat!
The Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids (2005) goes on to explain the process;
”In the absence of dietary carbohydrate, de novo synthesis of glucose requires amino acids derived from the hydrolysis of endogenous or dietary protein or glycerol derived from fat. Therefore, the marginal amount of carbohydrate required in the diet in an energy-balanced state is conditional and dependent upon the remaining composition of the diet.”
What this means is that the body will synthesize the little bit of glucose needed by the brain and red blood cells, etc from the protein taken in through the diet —provided it is in adequate amounts, or from glycerol which is formed when fat is broken down.
I encourage people to target protein first, add low carb veggies and fruit (such as lime, lemon, and a few berries), then add a bit of fat to make things taste good and to provide a source of essential fatty acids. Protein and fat both provide satiety (not feeling hungry) but protein has significantly less calories than fat. If one is aiming for weight loss, adding lots of extra dietary fat (in addition to what comes naturally in protein foods) is counter-productive. That doesn’t mean avoid fat, either. Eat the egg with the yolk and marbling in steak is fine and so is using some fat for cooking food or putting on veggies, but for weight loss, it’s best to avoid extra fat that doesn’t come a good source of protein.
Final Thoughts…
What makes a diet low carb or ketogenic is how much carbohydrate it has, not how much fat it contains; with a low carbdiet being one that is < 130 g carbohydrate per day and a ketogenic diet as one that is 20—50 g carbohydrate per day. The amount of fat in the diet does not make it low carb or keto!
While a low carb diet is often called a “LCHF diet” i.e. “low carb high fat”, it is really only “high fat” relative to the recommended American or Canadian diet which is supposed to be < 30% fat. A low carb diet that targets protein may be as high ~50-55% fat or significantly lower if lower fat protein is chosen — but is no where near the 75% fat of a classic ketogenic diet (KD diet) used for those with epilepsy*, or some fat-based variations low carb diets. It is my experience that many people, especially peri-and post menopausal women do much better on the higher protein version. A Low carb or keto diet is not about eating lots of bacon, avocado, heavy whipping cream or ‘fat bombs’ and “bulletproof” coffee. It is about eating less carbs.
*Addendum (Nov 1, 2019 @ 2:35 pm) It was pointed out to me that the Charlie Foundation uses a Low Glycemic Index Treatment Diet for the management of epilepsy that is closer to 60% fat, which allows for less fat than a strict KD diet.
Yes, we need some essential fat in the form of linoleic acid and alpha-linolenic acid which can easily be obtained by eating meat and eggs, and for vegetarians to eat nuts including walnuts and seeds such as flax seed, but for the most part, eating the foods listed above that are rich in the nine essential amino acids will provide all the essential fat we need.
Update (Nov 3, 2019): The following article outlines which protein foods are best for weight loss on a low carb or ketogenic diet.
More Info
If you would like more information about the services that I provide, please have a look under the Services tab, or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Resources
Feinman RD, Pogozelski WK, Astrup A, Bernstein RK, Fine EJ,Westman EC, et al. Dietary Carbohydrate Restriction as the First Approach in Diabetes Management: critical review and evidence base. Nutrition. 2015;31(1):1—13.
National Cancer Institute, Food sources of alpha-linolenic acid (PFA 18:3), Epidemiology and Genomics Research Program, Table 6, https://epi.grants.cancer.gov/diet/foodsources/fatty_acids/table6.html
National Academies of Sciences, Engineering and Medicine, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids, 2005, https://www.nap.edu/catalog/10490/dietary-reference-intakes-for-energy-carbohydrate-fiber-fat-fatty-acids-cholesterol-protein-and-amino-acids
INTRO: This article documents the science that supplementing with Vitamin D can help protect us against the flu, recommendations for how much we should be supplementing, as well as excellent low carb dietary sources of this important fat-soluble vitamin.
The other day I shared an article[1] on social media from a local Canadian news outlet about a 37 year old man from Ontario who decided to forgo his annual flu shot last year and ended up in hospital with pneumonia for two months, after he contracted the flu virus from his daughter. The article indicated that data from Statistics Canada indicates that only 1/3 of Canadians above the age of 12 get the flu shot every year, yet according to deputy chief public health officer for the Public Health Agency of Canada, Dr. Howard Njoo, more than 12,000 Canadians end up hospitalized for flu-related complications each year, and between 3,000-4,000 people die as a result. Dr. Njoo was quoted as saying;
“it makes common sense that you should get your flu shot.”
There was much heated discussion on Facebook whether there is “proof” that the flu shot prevents people from getting the flu.
A well-known epidemiologist said that “unlike childhood vaccinations (ie, diphtheria, tetanus, pertussis, polio, measles, mumps, rubella, etc), there is no conclusive proof that flu shots reduce risk of either getting the flu or its complications. There are no large randomized trials, which is the standard for establishing a causal connection. So all we really have are observational studies, which are subject to a lot of confounding“. The epidemiologist noted that there was a meta-analysis of 44 years’ worth of studies that was published in Lancet Infectious Diseases in 2011 which found only “moderate efficacy” of the flu vaccine[2].
In response, a GP referenced a 2012 review of 15 meta-analyses related to the effectiveness of the flu vaccine for adults and the elderly which found they provided what was described as ‘satisfactory immunogenicity’, but that data on inactivated vaccines for children was scarce[3].
One of the other people that commented about the CTV article brought up studies that I was previously unaware of that indicate that Vitamin D supplementation may reduce the risk of getting the flu â — especially for those who are low in in this fat-soluble vitamin to begin with. Stats Can data from 2013 indicates that 1/3 of Canadians fall in this category [4]. It was this fact that motivated me to write this article.
Studies Showing that Vitamin D Attenuates the Flu
There are two large-scale meta-analyses — one from 2013 and the other from 2017 that indicate that Vitamin D supplementation can reduce the risk of getting an upper respiratory infection (URI) including influenza (“the flu”).
The first study by Bergman et al [5] analyzed data from 11 placebo controlled trials that involved more than 5,600 subjects and found that those taking a daily dose of Vitamin D had half the risk of developing an upper respiratory infection (URI), including influenza (‘the flu”). This held true even though many of the studies used very low dose of supplementation.
The second of the two large-scale meta-analysis by Martineau et al [6] analyzed the data from 25 randomized controlled trials and involved more than 11,300 subjects. This study found that Vitamin D supplementation reduced the risk of developing an upper respiratory infection (URI), including the flu and those who were the most deficient experienced the most benefit. Even those subjects with very low Vitamin D status had 1/3 the risk when supplementing with Vitamin D, compared to those who did not take any.
Both meta-analysis found that daily dosing with Vitamin D was more effective than taking larger (bolus) doses once a week, or once a month.
There are numerous studies which indicate that people with lower levels of Vitamin D are more likely to get the flu and a 2010 study with healthy adults found that people with lower levels of were twice as likely to get the flu than people with high levels of Vitamin D [7].
Supplementing with Vitamin D to Reduce Risk of Flu
Health Canada’s recommended daily intake (RDAs) for Vitamin D (updated in 2011) are 600 International Units (IUs) for everyone aged one year old to 70 years old and 800 IU for adults over 70 years of age. Health Canada’s safe upper limit (UL) is listed as 4,000 IU per day, however recent scientific publications indicate that there was an error in the calculations used to determine them.
Two researchers from the School of Public Health at the University of Alberta published a paper in October 2014 which indicates that the Institute of Medicine (IOM) that develops the Recommended Dietary Allowances (RDAs) used by both Canadians and Americans made a serious error in their calculations in determining the RDAs for Vitamin D [9] and that rather than 600 IUs being needed to prevent deficiency in 97.5% of individuals, the actual amount is estimated to be 8895 IU of Vitamin D per day — which is above the Health Canada’s tolerable upper intake of 4000 IU per day.
On top of that, researchers from the University of California at San Diego and Creighton University in Omaha, Nebraska published a letter in the same online journal in March 2015 which said that they have confirmed the Institute of Medicine’s miscalculation that was noted by the Canadian investigators [10].
A press release published in Science News on March 17, 201[11] indicated that;
“The recommended intake of vitamin D specified by the IOM is 600 IU/day through age 70 years, and 800 IU/day for older ages. Calculations by us and other researchers have shown that these doses are only about one-tenth those needed to cut incidence of diseases related to vitamin D deficiency.“
How much Vitamin D should we supplement?
The Vitamin D Council (a US-based group) recommends adults take 5,000 to 10,000 IU/day, depending on body weight and recommend people have their levels checked to make sure it is > 40 ng/ml (100 nmol/l) and to maintain serum levels at 50 ng/ml (125 nmol/L). Since Vitamin D toxicity manifests as high levels of calcium in the blood and urine, the Vitamin D Council recommends monitoring via blood tests that serum levels don’t exceed 150 ng/ml (374 mmol/L).
Since Health Canada’s current upper limit is 4,000 IUs per day (which may be based on an error in calculation, as noted above), a prudence dosage for supplementation for a healthy adult would not exceed 4,000 IUs per day.
Note: I also recommend people take 100 mcg of Vitamin K2 (menaquinone-4, or menaquinone-7) as Vitamin K2 plays a synergistic role with Vitamin D which regulates blood levels of calcium. Vitamin K prevents calcium from accumulating in soft tissues, such as the blood vessels (contributing to Coronary Artery Calcification)[12]. Put simply, Vitamin K helps ensure that calcium ends up in bone, not arteries.
NOTE: People taking Warfarin (Coumadin) or other anticoagulant medication should not supplement with Vitamin K2 except under the advice of the physician prescribing Warfarin.
If you are a healthy adult under 50 years old with no family risk of cancer* or osteoporosis, 1000 IU Vitamin D3 per day (plus 100 mcg of Vitamin K2) is probably sufficient. Be sure to choose the D3 form (not D2) as it is more efficient at raising serum levels. For adults under 50 with a family history of cancer or who are at risk for osteoporosis, a dosage of 2000 IU Vitamin D3 per day (plus 100 mcg of Vitamin K2) may be more appropriate.
*there are many studies indicating that supplementing Vitamin D levels for those in northern latitudes (such as Canada and the northern US) lowers the risk of certain types of cancer, especially breast, colon and prostate cancer.
I usually recommend that healthy adults over the age of 50 double the amounts above â — so 2,000 IUs Vitamin D3 per day (plus 100 mcg of Vitamin K2) and for those with a family history of cancer to take 3,000 IUs Vitamin D3 per day (plus 100 mcg of Vitamin K2).
Remember though that Vitamin D is a fat soluble vitamin, so be sure to have your serum levels checked periodically as your body is able to stores for long periods of time. The best indicator of Vitamin D status is a routine blood test called 25-hydroxy vitamin D.
Best Low Carb Sources of Vitamin D to Help Our Bodies Fight the Flu
Fish and Seafood
Below is a list of foods that are naturally high in Vitamin D and that can be included on a low carb or ketogenic diet. The best source of all comes from the sea in the form of fish and seafood.
Wild-caught salmon
Wild-caught salmon has on average almost 1000 IU of Vitamin D (988 IU) vitamin D per 3.5-ounce (100-gram) serving and some studies have found up to 1,300 IU per serving [13].
Herring
Fresh Atlantic herring provides 1,628 IU Vitamin D per 3.5-ounce (100-gram) serving [14]. That’s huge!
Halibut
Halibut is an exquisitely delicious white-fleshed fish that provides 600 IU Vitamin D per per 3.5-ounce (100-gram) serving [14].
Mackerel
Mackerel is simply delicious grilled on the BBQ and provides 360 IU Vitamin D per 3.5-ounce (100-gram) serving [14].
OYSTERS
Oysters contains 320 IU of Vitamin D in a 3.5-ounce (100-gram) serving [14].
Sardine
Sardine is an inexpensive and pretty good source of vitamin D — with one serving containing 272 IU of Vitamin D [14].
Canned Tuna
Canned tuna is an easy and inexpensive way to incorporate more Vitamin D into the diet and contains 236 IU of Vitamin D in a 3.5-ounce (100-gram) serving [14].
Non-fish Sources of Vitamin D
Fish and seafood are not the only sources of Vitamin D. Whole egg is a good source, with most of the Vitamin D found in the yolk.
Egg yolk
The average supermarket egg contains only 18—39 IU of vitamin D, but pastured eggs that roam outside and are exposed to sunlight produce eggs with 3 to 4 times that amount [15]!
Mushrooms
With the exception of fortified foods such as dairy, mushrooms are the only plant source of Vitamin D, however mushrooms only produce Vitamin D2, rather than Vitamin D3 which is not as effective at raising blood levels of Vitamin D. Even then, button mushrooms grown outside under sunlight contain as much as 2,300 IU per 3.5-ounce (100-gram) serving [16].
Final thoughts…
There is good evidence that adding Vitamin D3 supplementation to your daily routine may boost your ability to fight of upper respiratory infections, including the flu.
Supplementing your diet with Vitamin D and/or eating plenty of low carb foods rich in Vitamin D3 can help ensure adequate stores of this important nutrient.
More Info
If you would like more information about my services, please have a look under the Services tab or in the Shop and if you have any questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Osterholm MT, Kelley NS, Sommer A, et al. Efficacy and effectiveness of influenza vaccines: a systematic review and meta-analysis. Lancet Infect Dis 2011 (published online Oct 25)
Manzoli L, Ioannidis JP, Flacco ME, De Vito C, Villari P. Effectiveness and harms of seasonal and pandemic influenza vaccines in children, adults and elderly: a critical review and re-analysis of 15 meta-analyses. Hum Vaccin Immunother. 2012;8(7):851—862. doi:10.4161/hv.19917]
Bergman P, Lindh AU, Bjí¶rkhem-Bergman L et al, Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials, PLoS One. 2013 Jun 19;8(6):e65835.
Martineau AR, Jolliffe DA, Hooper RL, Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data, BMJ. 2017 Feb 15;356:i6583
Sabetta, J.R., DePetrillo, P., Cipriani, R.J., et al., Serum 25-hydroxyvitamin d and the incidence of acute viral respiratory tract infections in healthy adults. PLoS One, 2010. 5(6): p. e11088.
Veugelers PJ, Ekwaru JP. A statistical error in the estimation of the recommended dietary allowance for vitamin D. Nutrients. 2014;6(10):4472—4475. Published 2014 Oct 20. doi:10.3390/nu6104472
Heaney R, Garland C, Baggerly C, French C, Gorham E. Letter to Veugelers, P.J. and Ekwaru, J.P., A statistical error in the estimation of the recommended dietary allowance for vitamin D. Nutrients 2014, 6, 4472-4475; doi:10.3390/nu6104472. Nutrients. 2015;7(3):1688—1690. Published 2015 Mar 10. doi:10.3390/nu7031688
Theuwissen E, Smit E, Vermeer C, The role of vitamin K in soft-tissue calcification, Adv Nutr. 2012 Mar 1;3(2):166-73.
Schmid A, Walther B., Natural vitamin D content in animal products, Adv Nutr. 2013 Jul 1;4(4):453-62
USDA, Composition of Foods Raw, Processed, Prepared USDA National Nutrient Database for Standard Reference, Release 27
Kí¼hn J, Schutkowski A, Kluge H.,Free-range farming: a natural alternative to produce vitamin D-enriched eggs, Nutrition. 2014 Apr;30(4):481-4.
Simona RR, Borzelleca JF, DeLuca HF, Safety assessment of the post-harvest treatment of button mushrooms (Agaricus bisporus) using ultraviolet light, Food and Chemical Toxicology, Volume 56, June 2013, Pages 278-289
If you want to see me before your extended benefits reset at the end of December, now is the time to book your Complete Assessment Package. Most insurers will reimburse services into the following year, provided that they are paid for before the deadline, but if you want to start the New Year off with your new Meal Plan, remember that this takes a bit of time.
Whether we meet in person or remotely via Distance Consultation, the time needed is the same!
First we need to set an appointment for me to assess you — and this appointment usually takes between an hour and an hour and a half.
Then I need to schedule a time to design your Meal Plan — and I do them in the order that I assess people.
Finally, we need to set an appointment for me to teach you your Meal Plan and answer any questions you may have, so you are ready to implement it.
You can learn more about the Complete Assessment Package by clicking here or by looking under the Services tab or in the Shop.
Ready to get started?
Please download and complete the Intake and Service Option Form available for download here and then select the Complete Assessment Package.
Then, return the completed form to me at the email address written on the form, listing with the times you are available for an appointment.
If you reside in the US or elsewhere and are seeking nutrition education sessions, please use this formand select the Meal Planning Package. Keep in mind that services for those outside of Canada are for nutrition education purposes only, so if you have complex health issues or take multiple medications, please consult with a Registered Dietitian where you live.
If you would like more information, please send me a note using the Contact Me form, above.
Don’t miss the deadline. Most extended benefits plans reset on December 31st.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
The new study[1] that I mentioned in an article last week indicates that those with a genetic predisposition to having lower LDL cholesterol and systolic blood pressure have a lower lifetime risk of cardiovascular disease (CVD), but what the study doesn’t mention was that research published last year[2] found that people with the low LDL variant also having a genetic predisposition to lower levels of triglycerides. This begs the question as to whether it is really the lower LDL that lowers the lifetime risk of CVD, or the lower triglycerides or both.
*Note: special thanks to George Henderson (@puddleg) from Auckland, New Zealand for bringing this earlier study to my attention.
That is, it could very well be that perceived benefit of having a genetically lower LDL reported in this new study is actually due to the same people also having a genetic predisposition to having lower levels of triglycerides!
In a large-scale study published in 2018 [2], researchers analyzed data from several hundred thousand individuals. First they estimated associations from summary genetic data from more than 670, 000 people from 9 different European databases. Then they analyzed individual-level genetic data from >390 000 people and looked at the associations of naturally occurring genetic variation coding for lipoprotein lipase (LPL) inhibitors with cardiovascular and metabolic health outcomes. Researchers found that a subset of subjects with a genetic variant to lower LDL-cholesterol levels also had a genetic predisposition to lower triglyceride levelsand the group that had both had the lowest odds of coronary artery disease [2]. This 2018 study [2] raises the issue as to whether the results of the current study [1] referred to in last week’s article really indicates that genetically lower LDL levels along with lower systolic blood pressure are responsible for lower rates of lower cardiovascular disease, or whether the lower rates of CVD are due to these same people also having genetically lower levels of triglycerides, (or perhaps a combination of both).
The Risk of Higher Triglycerides
A 2016 study published in the Journal of Circulation [3] examined the health risks associated with high levels of triglycerides in those with CVD. Researchers analyzed data from a large-scale study conducted in Israel (Bezafibrate Infarction Prevention (BIP) trial) which followed > 15,300 people with heart disease for a period of 22 years. At the start of the study, participants had their cholesterol and triglyceride levels measured, as well as other health markers. Based on fasting triglyceride levels, subjects were divided into 5 groups, ranging from low triglyceride levels to extremely high triglyceride levels.
Note: Triglycerides below 150 mg/dL (1.70 mmol/L) are considered normal, whereas triglycerides over 200 mg/dL (2.5 mmol/L) are considered high.
After more than two decades of follow-up, researchers found that compared to subjects with low triglycerides, those with the highest triglyceride levels (> 500 mg/dL / 5.6 mmol/L) had almost a 70% greater risk of death over the 22 year period. In fact, even with subjects with triglycerides of 100 to 149 mg/dL (1.13 – 1.68 mmol/L) the elevated risk of death was detected over subjects with lower triglycerides levels (<100 mg/dl / 1.12 mmol/L).
Evidence is emerging that plasma triglycerides represent a causal risk factor for CVD and that genetic variants in a least 6 genes that modulate plasma triglyceride levels have been linked to CVD [4-12].
Using a research method called multivariable Mendelian randomization, researchers are able to group study subjects based on their genetic markers, so they are naturally randomized. Using this method, researchers are able to separate the effects on CVD associated with triglycerides from those associated with LDL [13]. It has been found that the effect of genetic variations involving triglyceride increases the risk of CVD independently of LDL concentration.
A 2016 review article [14] postulates that the risk factors surrounding increased plasma triglyceride concentration may involve the metabolism of lipoproteins that carry triglycerides in the blood, and that it could lie in a variant gene that encode for the enzyme lipoprotein lipase (which breaks down triglycerides), or for a gene that encodes for regulators of lipoprotein lipase [14].
Final Thoughts
It’s interesting to study whether those with a genetic predisposition to having lower LDL cholesterol have lower lifetime relative risk of cardiovascular events [1], but further study is needed to factor in the subset of subjects that also have a genetic predisposition to lower triglyceride levels, as well as a genetic variant to lower LDL.
More Info?
If you have been diagnosed as having “high cholesterol” and want to know how a low carbohydrate diet may help, you can learn more about the services I provide under the Services tab or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Ference BA, Bhatt DL, Catapano AL et al, Association of Genetic Variants Related to Combined Exposure to Lower Low-Density Lipoproteins and Lower Systolic Blood Pressure With Lifetime Risk of Cardiovascular Disease, JAMA. 2019 Sep 2. doi: 10.1001/jama.2019.14120. [Epub ahead of print]
Lotta LA, Stewart ID, Sharp SJ, et al, Association of Genetically Enhanced Lipoprotein Lipase—Mediated Lipolysis and Low-Density Lipoprotein
Cholesterol—Lowering Alleles With Risk of Coronary Disease
and Type 2 Diabetes, JAMA Cardiology, 2018;3(10):957-966. doi:10.1001/jamacardio.2018.2866
Klempfner R, Erez A, Ben-Zekry S et al, Elevated Triglyceride Level Is Independently Associated With Increased All-Cause Mortality in Patients With Established Coronary Heart Disease, Circulation: Cardiovascular Quality and Outcomes Vol 9(2), 2016, p 100-108, https://doi.org/10.1161/CIRCOUTCOMES.115.002104
Voight BF, Peloso GM, Orho-Melander M, et al. Plasma HDL cholesterol and risk of myocardial infarction: a Mendelian randomisation study.
Lancet. 2012;380:572—580. doi: 10.1016/S0140-6736(12)60312-2.
Triglyceride Coronary Disease Genetics Consortium and Emerging
Risk Factors Collaboration, Sarwar N, Sandhu MS, Ricketts SL, et al.
Triglyceride-mediated pathways and coronary disease: collaborative analysis of 101 studies. Lancet. 2010;375:1634—1639.
Jí¸rgensen AB, Frikke-Schmidt R, West AS, Grande P, Nordestgaard
BG, Tybjí¦rg-Hansen A. Genetically elevated non-fasting triglycerides
and calculated remnant cholesterol as causal risk factors for myocardial
infarction. Eur Heart J. 2013;34:1826—1833. doi: 10.1093/eurheartj/
ehs431.
Do R, Stitziel NO, Won HH, et al; NHLBI Exome Sequencing Project.
Exome sequencing identifies rare LDLR and APOA5 alleles conferring
risk for myocardial infarction. Nature. 2015;518:102—106. doi: 10.1038/
nature13917.
Pollin TI, Damcott CM, Shen H, Ott SH, Shelton J, Horenstein RB,
Post W, McLenithan JC, Bielak LF, Peyser PA, Mitchell BD, Miller M,
O’Connell JR, Shuldiner AR. A null mutation in human APOC3 confers
a favorable plasma lipid profile and apparent cardioprotection. Science.
2008;322:1702—1705. doi: 10.1126/science.1161524.
TG and HDL Working Group of the Exome Sequencing Project, National
Heart, Lung, and Blood Institute, Crosby J, Peloso GM, Auer PL, et al Loss-of-function mutations in APOC3, triglycerides, and coronary disease. N Engl J Med. 2014;371:22—31.
Jí¸rgensen AB, Frikke-Schmidt R, Nordestgaard BG, Tybjí¦rg-Hansen A.
Loss-of-function mutations in APOC3 and risk of ischemic vascular disease. N Engl J Med. 2014;371:32—41. doi: 10.1056/NEJMoa1308027.
Folsom AR, Peacock JM, Demerath E, Boerwinkle E. Variation in
ANGPTL4 and risk of coronary heart disease: the Atherosclerosis Risk
in Communities Study. Metabolism. 2008;57:1591—1596. doi: 10.1016/j.
metabol.2008.06.016.
Varbo A, Benn M, Tybjí¦rg-Hansen A, Jí¸rgensen AB, Frikke-Schmidt R,
Nordestgaard BG. Remnant cholesterol as a causal risk factor for ischemic heart disease. J Am Coll Cardiol. 2013;61:427—436. doi: 10.1016/j.
jacc.2012.08.1026
Do R, Willer CJ, Schmidt EM, et al. Common variants associated with
plasma triglycerides and risk for coronary artery disease. Nat Genet.
2013;45:1345—1352. doi: 10.1038/ng.2795.
Musunuru K, Kathiresan S, Surprises From Genetic Analyses of Lipid Risk
Factors for Atherosclerosis, Circulation Research; Compendium on Atherosclerosis, 2016;118:579-585. DOI: 10.1161/CIRCRESAHA.115.306398
This recipe is posted as a courtesy to those following a variety of low-carb and ketogenic diets (not necessarily Meal Plans designed by me). This recipe may or may not be appropriate for you.
Even though I developed a pretty good pancake recipe a year ago (posted here), I found myself wanting pancakes that were light and fluffy like my old flour-based ones. I also wanted to make some that didn’t have xanthan gum in them (as it caused one of my family members unpleasant GI issues).
I decided to play around with my original recipe but this time, I added just a touch of coconut flour to the almond flour, and just a bit more egg. These pancakes came out amazing — so good in fact, that I made chocolate chip pancakes with the same recipe, the next morning. This recipe is for both!
(Optional: 40 g — 85% dark chocolate, finely chopped)
5 large eggs
1 1/2 tsp real vanilla extract (I used homemade)
1/3 cup whole milk (I used goat’s milk because that’s what I have)
1/4 cup light olive oil
Method
In a medium sized bowl, put the almond and coconut flour, baking powder, , Swerve® and salt.
In a smaller bowl, beat the eggs, add the milk and real vanilla extract, add oil and mix well.
preheat cast iron pan to medium and while heating, mix the wet ingredients and fold into the dry ingredients.
If using, toss chocolate chunks into batter and mix well.
When the fry pan is hot, melt some of the butter and make 3 pancakes per pan (each 3″³ in diameter)
Cover pan for a minute or two to enable pancakes to rise well and to cook inside. They will start to look a little dry around the edges.
When the edges of the pancakes loose their wet look, lift off cover and gently flip each of them over and re-cover the pan until the second side finishes cooking. (I press the middle with a clean finger to see if they spring back)
Enjoy!
Macros (for 2 pancakes – without chocolate chips)
Carbs: 3 g (net) / 6 g total
Fat: 23 g
Protein: 9 g
If you would like to know how this recipe and some of my other recipes on this website can be included into a low-carb Meal Plan designed for you, I’d be glad to help.
You can find out information about the packages and stand alone sessions that I provide (both in-person-and via Distance Consultation) by clicking on the Services tab above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Share to Flipboard:
Yesterday, with some encouragement from others, I went to a hairdresser that specializes in cutting “curly hair”. In one sense, it was life-changing to have my hair cut to actually “be” curly, and in another it was another step in my “journey”, a Dietitian’s Journey. My “unruly” hair was not unlike being overweight and in poor health; all were barriers to looking and feeling the way I wanted, but not something I dealt with until recently.
I saw my hair’s texture as a barrier to having the smooth, silky hair I desired and that I saw in the media as being something to be valued. Growing up, naturally curly or wavy hair was seen as unruly; something that needed to combed or brushed and restrained in some way, in a clip or pin of some kind. Yet older women went for “perms” and these man-made curls were placed where they were desired, in the size that was desired and coloured to the chosen shade.
Growing up in the early 1970s, being overweight was solved with “girdles”; just like unruly hair was solved with combs and hair clips. For those that are unfamiliar with “girdles”, they are essentially torture devices that women squeezed into to arrange their fat in a more acceptable manner, and at least keep it from jiggling where it offended others and embarrassed the individual. Wearing a girdle wasn’t about health; but appearance.
Around this time the “health at every size” movement became popular, but it wasn’t until I was a Dietitian that it came to my awareness. The overweight women around me were not into acceptance, but denial and girdles were their solution.
In the 1990s, I was torn between the reality that being overweight or obese was rarely associated with positive health outcomes, yet at the same time knowing there was a need to be compassionate toward those who themselves were overweight or obese. At this point, I was slim and in good health, so my views were coldly ‘academic’. That said, I was always against “fat-shaming”, but didn’t feel the answer was to “embrace” being fat. I missed the point; it wasn’t about embracing being overweight or obese, but about focusing on health — health at every size.
Me and my 3 sons – White Pine Beach, September 10 2003
After having given birth to 3 children in a little over a year (yes, one set of twins and a singleton), I had little or no time to focus on “me”. My weight continued to creep up and along with it, my blood sugar and blood pressure. The photo on the left is what I looked like at this time 16 years ago. I knew my being overweight (obese, actually) was unhealthy, but despite my education, the idea of “eating less and moving more” seemed impossible.
The years passed and in May 2008, when I graduated with my Masters Degree in Human Nutrition, I was obese and pre-diabetic. I heeded my GP’s advice and followed the (then) Canadian Diabetes Association’s dietary recommendations to eat 60 g of carbohydrate at each meal, plus protein and carbohydrate at each of 3 snacks. I considered I was being so virtuous by eating “whole grain”, which was whole-wheat pasta, brown rice and multigrain brown bread with seeds. Despite this, within two years I was diagnosed as having type 2 diabetes and in hindsight, eating that many carbohydrates per day; carbohydrates that were really just less refined and not truly “whole, foods”, and eating that many times a day, made becoming diabetic inevitable. The only issue was how long would it take.
When I first saw an endocrinologist in 2014, she told me that if I continued to eat the way I was eating (same as above) I would be on insulin within 5 years. She encouraged me to eat a maximum of 100 g of carbs per day and mostly as unrefined vegetables, with only a small amount of fruit and unprocessed, whole grain. It took until my health had become a crisis two years later until I had little choice but to change my lifestyle. That was March 5, 2017 and the rest as they say, is history.
May 2008 (Masters Convocation) – May 2019
The photo on the left is what I looked like at my Master’s Convocation in May 2008 and the photo on the right is what I looked like this past May 2019. Yes, there’s a big difference — a 55 pound difference and even better, my type 2 diabetes is in remission and I no longer have high blood pressure.
In my health-recovery journey (which you can read in its entirety, here), I didn’t focus as much on weight, as I did on lowering my blood sugar and blood pressure. My focus from the beginning of my journey was on health as I attained a healthy body weight and waist circumference.
Surprisingly, my first experience with ‘fat-shaming’ was in January 2018; ten months into my health-recovery journey. I was told by someone quite well known in low-carb circles on social mediathat they “wouldn’t trust a fat Dietitian” and that ”once you get in shape then you can dish out advice“. I was hurt and offended, and my response at the time was to write an article I titled “Competent to Counsel“; where I addressed that what makes me competent or credible is not my own body weight, but my knowledge. I still feel that way now, even thought I’m slim. While it was offensive to be spoken to in this way, it made me acutely aware of the tremendous bias that overweight and obese people face; especially obese clinicians. I think it gave me more compassion towards those that struggle with these issues who have faced this type of disdain for years.
It has been 6 months since I achieved my health and weight loss goals, and both are stable. I’m still below the criteria for type 2 diabetes and have normal blood pressure.
I’m still not used to being ‘slim’. I still think I can’t fit in a space behind a chair, or beside a parked car when I have ample room. I try on clothes that I think are the right size, and they are too big — and then assume the brand must be ‘sized wrong’. I’ve been told it takes a while to adapt. That said, I am fully aware that as many as 80% of those who lose weight regain it within two years, so being in ‘maintenance mode’ does not mean I do nothing. I continue to monitor my weight weekly and waist circumference every few weeks. While less frequently than before, I continue to test my blood sugar at home and go for my HbA1C test every 3 months and now that I am off blood pressure medication, check my blood pressure frequently. While I am at a good weight and waist circumference and have recovered much of my health, I cannot afford to rest on these accomplishments. When I see my weight creeping up, I take inventory of what I am eating differently and same with changes in blood sugar or blood pressure.
Maintenance isn’t about doing nothing, it is about doing the same thing, over time.
Embracing my health is a bit like embracing my curls. I am no longer the obese Dietitian with type 2 diabetes and high blood pressure and I can share my story with others; to encourage them that I understand, have “been there” and also that I have the knowledge to help. But just like those who embraced their own curls before me and encouraged me to do so too, each person has their own journey. My role is to support people in theirs.
More Info?
If you would like to know about how I can help you, you can learn about the services I provide under the Services tab, or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above and I will reply as I am able.
To our good health!
Joy
NOTE: This post is classified under “A Dietitian’s Journey” and is my personal account of my own health and weight loss journey that began on March 5, 2017. Science Made Simple articles are referenced nutrition articles, and can be found here.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
A studypublished September 2, 2019 [1] reported that lower LDL cholesterol levels combined with lower systolic blood pressure are associated with lower lifetime risk of cardiovascular disease (CVD), however there are several factors that need to be kept in mind in considering the results of this study.
First of all, the study looked at data from people that had inherited a genetic marker for having LDL cholesterol that was on average 15 mg/dl (0.39 mmol.L) lower and NOT people that had lower LDL cholesterol due to diet, medication and/or lifestyle interventions. So, even though people with this genetic predisposition of having lower LDL cholesterol had a 26% lower relative risk in of having a serious cardiac event such as a heart attack, need for a stent or death from a heart attack, it says nothing about the amount of benefit that might be achieved by dietary and lifestyle changes or medication.
Secondly, the average triglyceride to HDL ratio of the population studied in the study was 2.5 mg/dl (0.065 mmol/L), which is far from ideal. As outlined in an earlier article about LDL cholesterol and cardiovascular disease, several studies [2,3,4] have found that triglyceride to HDL ratio is a good reflection of LDL particle size; with the small, dense sub-fraction of LDL being atherosclerotic, and the large, fluffy sub-fraction of LDL not being atherosclerotic [5]. In the US, triglyceride to HDL ratio values are expressed in mg/dl and the ratios are interpreted as follows [6];
TG:HDL-C < 2 is ideal
TG:HDL-C > 4 is too high
TG:HDL-C > 6 is much too high
In the present study, the triglyceride to HDL ratio was 2.5 mg/dl, which means that they already had a higher than optimal level of small, dense LDL, predisposing them to cardiovascular risk. By comparing people with a genetic predisposition to lower LDL cholesterol to the risk of a population that already has a less than ideal triglyceride to HDL ratio, it makes the benefit of low LDL seem larger.
Significance of this Study
Sure, it is interesting to study whether those with a genetic predisposition to having lower LDL cholesterol have lower lifetime relative risk of cardiovascular events, but it doesn’t tell us anything about any possible benefit to ordinary people (without this genetic marker) lowering their LDL cholesterol.
As well, by comparing the risk of those with a genetic predisposition to lower LDL cholesterol to a population that already had a higher than ideal level of small, dense LDL, it exaggerates the appearance of perceived benefit of lower LDL cholesterol.
Comparing Apples with Apples
The question is, of what predictive benefit is a study that uses a group of people with a genetic variant to lower LDL cholesterol compared with a reference group that already has higher than ideal triglyceride to HDL ratio?
What can we deduce about those that don’t eat a standard American diet, such as those that eat a low carb or ketogenic diet and have lower overall levels of triglycerides and higher levels of HDL?
Nothing.
We can’t deduce anything.
Which raises the common question; does a low-carbohydrate diet increase the risk of cardiovascular disease?
Looking at what we know; a 2017 study by Chui et al [7] demonstrated that in those eating a low carbohydrate diet, HDL cholesterol increased and while LDL cholesterol also increases, it tends to be the large buoyant LDL that increased, with no change in the atherosclerotic small, dense LDL [7].
As well, a 2012 meta-study analysis of 19 randomized control trials (RCTs) by Santos et al [8] reported thatin those eating a low carbohydrate diet, triglyceride levels dropped by 29.71 mg/dL (0.34 mmol/L) and a 2014 study by Bazzano [9] reported that a low carbohydrate diet had a greater decrease in 10-year cardiovascular heart disease (CHD) risk score based on the Framingham Risk Score, than those on the low fat diet.
Final Thoughts
When we read headlines that indicate that “low LDL lowers lifetime risk of cardiovascular disease” we need to look closer at who is being studied.
A study about those with a specific genetic variation tell us nothing about the general public without it. It also tells us nothing about whether lowering LDL cholesterol through drugs or diet has any of the same benefits as having this genetic variation.
We also need to ask ourselves about whether the group being used for comparison purposes has optimal markers, or are already sub-optimal and inflates the perceived benefit and what about what they are eating? Is it relevant to those of us that follow a low-carbohydrate lifestyle?
UPDATE (Sept 22, 2019): in a new follow-up article, another study from last year raises a question as to how much of the lower CVD in due to lower LDL and blood pressure or due to this same variant also having lower triglycerides. You can read the new article here.
More Info?
If you have been diagnosed as having “high cholesterol” and want to know how a low carbohydrate diet may help, you can learn more about the services I provide under the Services tab or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Ference BA, Bhatt DL, Catapano AL et al, Association of Genetic Variants Related to Combined Exposure to Lower Low-Density Lipoproteins and Lower Systolic Blood Pressure With Lifetime Risk of Cardiovascular Disease, JAMA. 2019 Sep 2. doi: 10.1001/jama.2019.14120. [Epub ahead of print]
Hanak V, Munoz J, Teague J, et al, Accuracy of the triglyceride to high-density lipoprotein cholesterol ratio for prediction of the low-density lipoprotein phenotype B, The American Journal of Cardiology, Volume 94, Issue 2, 2004, Pages 219-222, https://doi.org/10.1016/j.amjcard.2004.03.069
McLaughlin T, Reaven G, Abbasi F, et al. Is there a simple way to
identify insulin-resistant individuals at increased risk of cardiovascular
disease? Am J Cardiol. 2005;96(3):399Y404.
Vega GL, Barlow CE, Grundy SM et al, Triglyceride to High Density Lipoprotein Cholesterol Ratio is an Index of Heart Disease Mortality and of Incidence of Type 2 Diabetes Melletus in Men, Journal of Investigative Medicine & Volume 62, Number 2, February 2014
Lamarche, B., I. Lemieux, and J.P. Després, The small, dense LDL phenotype and the risk of coronary heart disease: epidemiology, patho-physiology and therapeutic aspects. Diabetes Metab, 1999. 25(3): p. 199-211.
Sigurdsson AF, The Triglyceride/HDL Cholesterol Ratio, updated January 12, 2019, https://www.docsopinion.com/2014/07/17/triglyceride-hdl-ratio/
Chiu S, Williams PT, Krauss RM. Effects of a very high saturated fat diet on LDL particles in adults with atherogenic dyslipidemia: A randomized controlled trial, PLoS One. 2017 Feb 6;12(2):e0170664. doi: 10.1371/journal.pone.0170664
Santos FL, Esteves SS, da Costa Pereira A, Systematic review and meta-analysis of clinical trials of the effects of low carbohydrate diets on cardiovascular risk factors. Obes Rev. 2012 Nov;13(11):1048-66. doi: 10.1111/j.1467-789X.2012.01021
Bazzano LA, Hu T, Reynolds K, et al. Effects of Low-Carbohydrate and Low-Fat Diets: A Randomized Trial, Ann Intern Med. 2014;161:309—318. doi: 10.7326/M14-0180
Yesterday, a client of mine who was on insulin 13 weeks ago and who went off of it with her Endocrinologist’s knowledge and oversight to follow a low carbohydrate diet had her regular two-month follow-up visit, where she saw both the Dietitian and the Endocrinologist. Their respective reactions to her progress really highlights how some clinicians can be transformed by seeing the clinical possibilities of what can be accomplished by someone following a well-designed low carbohydrate diet, whereas others remain pessimistic regardless of the clinical evidence.
This is the 4th article about this young woman’s incredible progress from injecting insulin to following an individually designed low carbohydrate diet. You can read about the first two weeks at the start of her journey here, about her achieving normalized blood glucose in 10 weeks here, and about here achieving target HbA1C in less than 12 weeks here.
NOTE: The different reactions that these clinicians had are in no way reflective of their respective professions; it could have easily been in reverse. It could have been entirely different healthcare professions. There are clinicians in every field who are willing to consider emerging evidence and respond by being open to the clinical possibilities, and there are others who are not.
When this young woman arrived for her appointment, she saw the Dietitian first, which was the same one that she saw the visit before, and who told her that she should be eating ‘60 g of carbohydrate per meal plus snacks’ (see Sept 6 update, here). At yesterday’s visit, the Dietitian only looked at her blood glucose numbers from the last two weeks and not the last 8 weeks since she was last seen. She said her ‘numbers look good’, and asked the name of the Dietitian she was seeing, and my client told her my name. She responded and said “I hope she told you that you can’t get your numbers under 7 with just Metformin“. My client pointed out that she recently got TWO fasting blood glucose of 4.7 mmol/L, and the Dietitian said she didn’t see that. My client pointed out the two dates where she did, to which the Dietitian said nothing, as she was only considering the numbers from the last two weeks. My client said to me that at this point, she “just shut down” and waited to see the Endocrinologist.
My client then saw her Endocrinologist who had a medical student with him. This is the same Endocrinologist that told her 8 weeks ago that it was unrealistic for her to think that she could lower her HbA1C to below 7 mmol/L following a low carbohydrate diet, and that she should go back on insulin (see more here). The endocrinologist said to her yesterday “these numbers are amazing! What are you doing?”. My client responded by saying she was following a low carbohydrate diet designed by me. He also asked her who her Dietitian was, and my client told her my name. He said “it would be great if you could get those fasting blood glucose numbers under 7 so keep doing what you’re doing”. He then added, that should my client get pregnant, that he “might need to talk to her about taking insulin, if she doesn’t continue to eat a low carbohydrate diet”. He added, “you are going down the right path. Keep doing what you’re doing!”.
The contrast between the reactions of these two clinicians is striking. As I said above in the disclaimer, it has nothing to do with their respective professions, but about their willingness as individual clinicians to be open to different clinical possibilities, in light of the evidence. Some are, and some aren’t.
As a Dietitian, I wonder how the advice to someone with type 2 diabetes to “eat 60 g of carbs per meals plus snacks” and “get fasting blood glucose under 7.0 mmol/L” can be reconciled without prescribing insulin. I don’t see that it can be. It is still expected that “Diabetes is a chronic, progressive disease” and it need not be.
By recognizing a low carbohydrate and very low carbohydrate (keto) diet as two of the options of Medical Nutrition Therapy in the treatment of diabetes (both type 1 and type 2), the American Diabetes Association (ADA) has opened the way for Diabetes to NOT be a chronic, progressive disease! (For more information about the policy changes at the ADA, you can read any one of several articles from April 2019 that are posted under the Science Made Simple tab above, including this one.)
As to the belief that “you can’t get your blood glucose under 7 with just Metformin”, people with type 2 diabetes routinely have fasting blood glucose well under 7.0 mmol/L (126 mg/dl) following a well-designed low carbohydrate diet — both with and without Metformin, and clinicians should be current with the literature to know this. In fact, in the April 2019 Consensus Report on Diabetes and Pre-Diabetes the ADA said;
“Reducing overall carbohydrate intake for individuals with diabetes has demonstrated the most evidence for improving glycemia and may be applied in a variety of eating patterns that meet individual needs and preferences.”
The ADA’s Guidelines do not apply in Canada, but as healthcare professionals, we need to know they exist.
We also need to know that at their annual National Conference, hundreds of Certified Diabetes Educators (CDEs) in the US were recently taught to use a low-carbohydrate diet and a very low carbohydrate (ketogenic) diet as Medical Nutrition Therapy with people with both type 1 and type 2 diabetes, as well as how to manage the many medications prescribed for people with diabetes (you can read about this in this post and this one). As clinicians we need to be aware that a low carbohydrate and a very low carbohydrate (keto) diet are both safe and effective for those with Diabetes, even if it is not public policy in Canada yet.
There are plenty of peer-reviewed studies demonstrating the safety and effectiveness of a well-designed low carb or ketogenic diet for weight loss, as well as for normalizing blood glucose and blood pressure. Many have been reviewed on this site (for more information, please click on the For Physicians & Allied Health Providers tab above).
As I’ve done in previous articles about this client’s progress, I asked her on our weekly call to write in her own words what her visit was like yesterday. This is what she wrote;
“I was excited for my Endocrinologist to see my lowered A1C number and decreasing blood glucose numbers. I went into the appointment knowing that I would see the Dietitian first to review my numbers. She mentioned that the numbers were better, but my fasting glucose was still not ideal. I discussed that they are definitely coming down, although I realize they are not where they should be, and I even got a few under 7 in the past month. This Dietitian was only interested in the past two weeks and mentioned that Joy would not be able to enable me get my fasting glucose under 7 with just Metformin. Seeing the Dietitian really shut me down to discussing anything further with her. I let her gather her information and wanted to move on to my Endo.
Seeing my Endo was a turnaround. He was so amazed with my results, especially with my A1C having come down so much, that he encouraged me to just keep going. I felt so proud and encouraged. He gave me the motivation I was looking for and now I am ready to continue down this path to show him (and that Dietitian!) that it can be done without insulin.”
She has every reason to be proud of her accomplishments! She has been very intentional; about what she eats, about testing her blood sugar and in tweaking the timing of her Meformin.
If you would like more information about my services, please have a look under the Services tab or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
There is much “push back” when it comes to the standard advice to “eat less and exercise more” as a means of losing weight, and for good reason. For one, metabolism will slow as a result of caloric restriction — making it that much more difficult to lose weight when deliberately cutting calories. Another reason is that it is exceedingly difficult for an obese person to exercise. For many, just getting around is a chore. It is for this reason that I focus on helping people be less hungry by eating a different mix of protein, fat and carbohydrate — because a natural byproduct of being less hungry, is eating less. Being active is possible once a person is losing weight and not feeling hungry all the time. Yes, they are still “eating less and moving more” — but as a result, not as the focus.
Addendum (Sept 10 2019) — Weight loss is not only about what we eat. It’s also about when we don’t eat; whether it’s having times between meals where we don’t eat, or not eating from the end of supper until the first meal of the following day (whenever that is). Thanks Dr. Andy Phung for the reminder!
A new study published yesterday (September 9, 2019) in the journal Nature Medicine[1] has found that “eating less and exercising more” may actually be good advice as we age — because it turns out that we have decreased fat turnover as we age. If we eat the same amount as we always have and don’t increase the amount we exercise, we will end up gaining approximately 20% over a 10-15 year period [3].
Until recently little was known about fatturnover [2] — which is the storage and removal of fat from adipocytes (fat cells). A 2011 study showed that during the average ten-year lifespan of human fat cells, the fat in them (triglycerides) turns over six times, in both men and women [2], and that when people are obese, the fat removal ratedecreases and the amount of fat as triglyceride stored each year increases [2]. What we didn’t know until now is what happened to fat turnover as we age. This follow-up study headed by the same lead researcher as the 2011 study explored this issue, as well as differences in fat turnover after people have bariatric surgery which helps explain why some people regain their weight after weight loss, where as others don’t.
Eating Less Matters as We Age
Fat turnover is a difference between the rate of fat uptake into fat cells and the fat removalrate. High fat storage but low fat removal is what results in the accumulation of fat and in obesity. The “bad news” of this new study is that fat accumulation due to decreased fat turnover is what happens as we age, leading to accumulation of fat. That is, even if we don’t eat more or exercise less than previously, we will store more fat — which can result in as much as a 20% increase in body weight over 13 years [3].
“Those who didn’t compensate for that (i.e. decrease fat turnover) by eating less calories gained weight by an average of 20 percent”[3].
Researchers from the University of Uppsala in Sweden and the University of Lyon in France studied the fat cells of 54 men and women over an average 13 year period [3] and regardless of whether the subjects gained weight or lost weight, they had a decreased fat turnover.
Since fat turnover is decreased as we age, to prevent weight gain we need to take in less calories than we used to, even if we are just as active.
Why We Regain Weight After Weight Loss
The study also looked at fat turnover in 41 women who underwent bariatric surgery. Results showed that only those who had a low lipid turnover rate before the surgery were able to increase their lipid turnover after surgery and maintain their weight loss 4-7 years after surgery [1]. Researchers think that if people had a high lipid turnover rate before surgery, there is less ‘room’ for them to increase their lipid turnover rate after surgery, which is why they regain the weight. This could explain why so many people who lose incredible amounts of weight following any one of a number of “diets” regain it (and then some) afterwards.
Exercise and Lipid Turnover
Previous studies have reported that fat turnover increases as we exercise [2], so based on this new study, the idea of ‘eating less and exercising more’ actually matters as we age. We can either decrease our intake as we age and/or be a little more active and avoid gaining weight — which is easy enough to do for those who are slim, if they know.
But what about those who are already overweight or obese and now find out they are more prone to storing fat now that they’re older, even though they eat the exact same way and haven’t changed their activity level?
I believe the solution is the same regardless of a person’s age — focusing on the person eating in such a way as to be less hungry, so that in the end they end up eating less. As they lose weight because they’re not hungry all the time, being more active is easier to implement. The difference between it being “doable” depends on what we focus on. As covered in a previous article, we understand why a person who eats foods that are a combination of fat and carbs together eat more, but my approach is to gradually adjust the amount of carbohydrate in the diet, so that people can eat more protein and healthy fat, and end up feeling less hungry. When they aren’t being driven by the reward system of their brain (see linked article) to want more and more foods with carbs and fat together, it is much easier for them to eat when they are actually hungry. As they do, their weight drops as a result.
In light of this new study, what is important is that as people age, there is a natural tendency to put on weight even if they eat the same and don’t change their activity level. This means older people need to modify the amount of calories they take in and/or expend more energy, the question is how.
If you would like more information about my services, please have a look under the Services tab or in the Shop and if you have any questions, please feel free to send me a note using the Contact Me form above, and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
Arner P, Bernard S, Appelsved K-Y et al. (2019). “Adipose lipid turnover and long-term changes in body weight.” Nature Medicine 25(9): 1385-1389.
Arner, P. et al. Dynamics of human adipose lipid turnover in health and metabolic disease. Nature478, 110—113 (2011).
Karolinska Institutet, New study shows why people gain weight as they get older, Published: 2019-09-09 18:35, https://news.ki.se/new-study-shows-why-people-gain-weight-as-they-get-older
A few weeks after requesting that her endocrinologist take her off insulin so that she could begin a low carbohydrate diet with his and her GP’s oversight (article here), this young woman was told she needed to get her HbA1C to ≤7.0%, which is the therapeutic target for adults with type 2 diabetes. She was told that it was unrealistic for her to think that she could do so following a low carbohydrate diet, and that she should go back on insulin. She replied that she wanted to continue to eat a low carbohydrate diet for a total of 12 weeks, and her endocrinologist replied that more than likely he would need to put her back on insulin then, because it was not realistic for her to accomplish those goals using diet, even with Metformin support.
*Metformin doesn’t lower blood sugar, but helps the body become more insulin sensitive and to keep it from manufacturing glucose from stored fat or protein which is what underlies high morning blood sugar.
Well, she achieved the “impossible”!
She had her blood tests yesterday and when she checked her results on-line last night she could not believe it!! Her results were below the 7.0% therapeutic target. . . and this was (1) despite me starting her on a moderate low carbohydrate diet for the first several weeks and only gradually lowering carbohydrate content in order to meet clinical outcomes*, and (2) despite her having two weeks of weddings in mid-July where she ate a little ‘off-track’, which caused her blood sugar levels to rise).
In spite of these, she did it!!
Note: weight loss was only ~5% of her original weight, so would not account for her significant improvement in HbA1C results.
Here are her results:
from injecting insulin to HbA1c within target
*I was asked on social media after the previous update on her progress why I didn’t start this young woman on a very low carbohydrate, ketogenic diet from the outset. This is what I replied; “Diabetes Canada has not (yet?) deemed a LC or very LC diet as safe and effective medical nutrition therapy. I start people at 130 g of carbs, then reduce carbs as necessary to achieve clinical outcomes as a prudent approach. Hence why I conclude the article w/ hope of future policy change.“
After this young woman picked up her blood test results last night, she sent me this short email which I have her permission to share here;
“JOY!!!
Such overwhelming feelings right now. We will talk tomorrow but I took my blood test today and have attached the results! Please tell me I am seeing the number I am seeing because it is hard to believe! Also, for the graph this week, I had to change the minimum limit from 5 to 4 to account for my TWO readings of 4.7!! “
As relayed in the second article about her progress (posted here), in 10 weeks this young woman went from a fasting blood glucose of 16.8 mmol/L (303 mg/dl) to 4.7 mmol/L (85 mg/dl). . . and this past week she had her second fasting blood glucose reading of 4.7 mmol/L! Twice in one week, she achieved normal fasting blood glucose numbers; the first time since being diagnosed as having type 2 diabetes in 2017.
As she said in the previous article, she is “invested” in her health and that investment translated to her own determinationandhard work to follow her Meal Plan, to speak to her endocrinologist about adding an extra dose of Metformin at bed-time, and to determine when was the best timing to take her before bedtime dose and her early morning dose, in order to prevent her blood sugar from spiking in the morning due to Dawn Phenomena. Yes, I helped but she did the work!
I asked her to write in her own words what it was like to get her blood test results last night, and this is what she wrote:
“I feel so happy and proud of myself. Patience and consistency has paid off.
Typically, if I were doing this on my own or changing how I was eating, I never stuck with it long enough to see changes. The number on the scale or one bad meal would take me further back than when I started. However, keeping track of my blood sugars and being accountable to someone have kept me going, and I feel like nothing can hold me back now.
I am so motivated to keep going and giving myself time to progress. I know I can do this!”
I am so proud of her hard work and accomplishments!
I look forward a day when Diabetes Canada updates its Clinical Practice Guidelines to enable clinicians to recommend a low carb or ketogenic diet as a therapeutic option for those with diabetes â — just like the American Diabetes Association (ADA) did last year.
For more information about the clinical changes at the ADA, you can read any one of several articles from April 2019 that are posted under the Science Made Simple tab above, including this one.
UPDATE (Sept 6, 2019): During our weekly call, this young woman told me that she is meeting her endocrinologist this week and is looking forward to his reaction to her accomplishments, as well as that of his diabetes nurses. She said during her last visit 8 weeks ago (4 weeks after coming off insulin and beginning a low carbohydrate diet) her doctor told her that she is ‘not eating rice and needs to be eating that’ and reminded her that the ‘insulin will cover that’. The diabetes nurse also told her ‘she should be eating 60 g of carbohydrate per meal plus snacks’ (which is still the recommendations for those with diabetes in Canada). She assured them that she is carefully monitoring her blood sugar multiple times per day and that they are coming down, and she feels great.
If you would like more information about my services, please have a look under the Services tab or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This recipe is posted as a courtesy to those following a variety of low-carb and ketogenic diets (not necessarily Meal Plans designed by me). This recipe may or may not be appropriate for you.
The latest recipe in the low carb / keto world are “chaffles” which are a mixture of whole egg and grated cheese cooked in a waffle iron. They are really just crispy, textured cheese omelettes, not waffles! This morning, I wanted REAL waffles, and of course they were to be low carb, so I invented them by taking my tried and true 30 year old waffle recipe and subbing out what I know “works”.
Real Low Carb / Keto Waffles – makes 18 waffles
Ingredients
2 eggs, beaten
1 – 3/4 cup full fat milk (I used goat, but cow milk is fine — or for even lower carbs, one can use heavy whipping cream diluted with cold, filtered water) 1/2 tsp real vanilla extract 1/2 cup butter, melted
Sift the almond flour into a large mixing bowl, then add the other dry ingredients.
Beat the eggs in a separate bowl then add the milk (or diluted heavy whipping cream).
Pour the melted butter into the milk and egg mixture.
This is a very important step. Let the batter rest for 10 – 15 minutes to let the nut flours absorb the moisture from the egg and milk. Rushing this step will result in waffles that are not the right texture.
When the waffle iron is hot, spray it well with coconut oil spray and add ~1/2 cup of batter to each section. Work quickly and shut the cover. When it stops steaming excessively, open it up and check that the waffles are golden, but not brown.
Remove them from waffle iron and place them on a wire rack to allow to cool a few minutes.
Serve and enjoy!
Macros (per waffle)
Fat 16.3 g
Carbs (net) 3.3g
Protein 7.9 g
Kcals 196 calories
If you would like to know how this recipe and some of my other recipes on this website can be included into a low-carb Meal Plan designed for you, I’d be glad to help.
You can find out information about the packages and stand alone sessions that I provide (both in-person-and via Distance Consultation) by clicking on the Services tab above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This recipe is posted as a courtesy to those following a variety of low-carb and ketogenic diets (not necessarily Meal Plans designed by me). This recipe may or may not be appropriate for you.
One of my young adult sons hasn’t had muffins since we both went low carb almost 2 – 1/2 years ago, and really felt like ones with chocolate chips in them. He thought I could start with the recipe for my Low Carb Dark Chocolate Raspberry Scones but after I thought for a moment of all the recipes I have accumulated over the years, I knew the perfect one to adapt! It had lots of egg and sour cream and real butter and was a perfect ‘start’ to transform to low carb! The original recipe that I’ve had since 1998 comes from a friend of a friend of mine from New Zealand, named Syrrh.
Low Carb Dark Chocolate Chip Blackberry Muffins
Ingredients
3 cups almond flour, sifted
1 scoop of unflavoured whey isolate protein powder
1/2 cup of Truvia® sweetener (or low carb sweetener of choice)
3 eggs, beaten
3 tsp baking powder
3 Tbsp. butter, melted
1 cup full fat sour cream
1/2 cup 80% dark chocolate, cut into small chunks
12 blackberries (or ripe raspberries)
Method
Preheat oven to 360° F and line a dozen muffin tins with paper baking cups, spray well with coconut oil baking spray.
Chop up the chocolate.
Melt the butter over a low heat.
Beat the eggs in a small bowl. Measure out the sour cream.
Mix all the dry ingredients together in a medium size bowl, then add the beaten egg and sour cream.
Fold everything together with a spatula until uniformly moistened.
Add the chocolate chips.
Fold in chocolate chips until evenly distributed.
Fill each of the 12 paper lined muffin tins with batter.
Poke a hole in the center of each with a clean finger and insert a blackberry.
No need to push them down too much.
Bake in preheated 360° F oven for 20 minutes, until slightly browned on the top.
Remove the muffins from the oven, and place on a wire cooling rack for a few minutes. Turn off the oven and allow it to cool a bit.
After about 10 minutes, remove each muffin and place it on another wire cooling rack that is set over a baking sheet, then place the baking sheet with the rack of muffins in the oven (which has been turned off) for about 10 minutes, to ensure the bottoms are fully set.
Remove from the oven after 10 minutes and serve the muffins with fresh butter.
Macros
macros calculated using Chronometer software
If you would like to know how you can include this recipe and some of my other recipes that are on this website into a low-carb Meal Plan designed for you, please let me know.
You can find out information about the packages and stand-alone sessions that I provide (both in-person-and via Distance Consultation) by clicking on the Services tab above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Ten weeks ago, with her endocrinologist’s knowledge, this young woman discontinued insulin to begin a low carb diet. She has been gradually achieving normalized blood sugar, but this morning she had her first totally normal fasting blood sugar level since being diagnosed as type 2 diabetic! How cool is that?
As relayed in the first part of this account (posted here), at this young woman’s insistence her doctor gave her 12 weeks to ‘try a low carb diet’ and then he would put her back on insulin. Needless to say, he was not optimistic that changing her diet would ‘work’.
When she saw him a few weeks after beginning a low carbohydrate diet, and after lowering her fasting blood blood sugar from 16.8 mmol/L (303 mg/dl) to approximately 7.5 mmol/l, he told her that that the only way she could get her blood sugar below 7.0 mmol/L was to begin injecting insulin again. She responded by saying that she was not even half-way through her 12-week “trial period” and that she wanted to continue. As a result of her on-going “dawn phenomenon” (and upon my recommendation) she asked her endocrinologist to add an extra dose of Metformin* at bed-time to prevent her liver from making so much glucose in the morning (via gluconeogensis) and while he agreed, he said that if her HbA1C was not below 7.0 mmol/L (126 mg/dl) the next time she has it checked, he was putting her back on insulin.
*Metformin does not lower blood sugar, but helps the body become more insulin sensitive and to keep it from manufacturing glucose from stored fat or protein which is what underlies high morning blood sugar.
This coming week she is having her 3 month blood work and she and I both realize that it is unlikely her HbA1C will be below 7.0 mmol/L because there was a two week period this summer where she had several friend’s weddings, and got off-plan a bit. While she was quite disciplined, a few things she ate that were low glycemic index complex carbs still caused her blood sugar to rise above the levels she had been achieving. She got right back on plan after the weddings, and has been doing absolutely amazing! I am so very proud of her!
Here is a graph of her blood work over the past 10 weeks, including the ‘blip’ in the middle from the weddings;
From injecting insulin to normalized blood sugar in 10 weeks
She is not “there” yet, but this week she began having much less variation in blood sugar and the graph continues to be shifted downward. She is doing so well.
She has begun delaying the first meal of the day to noon because she doesn’t feel hungry in the morning, and is making extra effort to try different timing for taking her late-night and early-morning Metformin, so as to maximize the reduction in fasting blood sugar from dawn-phenomena (gluconeogenesis). This morning, while we were on our weekly Skype call, she took her blood glucose. 4.7 mmol/L (85 mg/dl)! This was her first normal early morning glucose since being diagnosed as being Type 2 diabetic in 2017!! I asked her to hold the meter up to the screen and took a picture of it!
Note: I’ve edited out her name and made the numbers a bit more readable.
In just 10 weeks, this young woman has gone from a 2 hour post-meal glucose reading of 18.7 mmol/L (337 mg/dl) to between 6.5 mmol/L (117 mg/dl) and 7.9 mmol/L (142 mg/dl).
The normal “goal” for 2 hour post-prandial glucose for someone with type 2 diabetes is ≤ 7.8 mmol/L (141 mg/dl) and in just 10 weeks, she is already doing considerably better than that!
As I did in the first post about her progress, I asked her to write in her own words what it has been like and how she feels. This is what she wrote today;
“I have been working together with Joy for close to 3 months now and I am amazed at the progress being made. Monitoring my blood glucose levels consistently has given me more insight into how and when I should be eating and taking my medication. This is key to the progress that I have made. There have been highs and lows, with life and weddings getting in the way, but getting back on track from any deviation is crucial. Knowing that I was accountable to Joy and my blood glucose monitor motivated me to get back to those lower numbers.
With the guidance of Joy, I have adjusted the timing of my Metformin and made tweaks to my diet which will help lower my numbers and prevent spikes. I found that I was not hungry in the mornings and all I needed was my coffee, so I pushed my first meal to lunch and my second meal has been dinner. My cravings have been close to eliminated and I don’t feel the need to snack between meals.
The biggest issue has been my increased fasting glucose due to the dawn phenomenon. To avoid a nightly prescription of insulin (which I never want to take again), I have been invested in figuring out when the nighttime spike is occurring and how I can adjust the timing of my Metformin to minimize it. For the past couple of nights, I have been checking my blood glucose levels every 1-2 hours, and have narrowed down the time at which the spike occurs. This investigation has lead me to my lowest ever fasting glucose reading today of 4.7!!! This is a number I never thought I would see.I couldn’t believe it. I still can’t believe it. I keep checking to see if I read the number wrong but there it is every time!
This has been a slow and steady road, but being consistent and invested in my health is starting to pay off. It has all been worth it and I cannot wait to see what the next 3 months bring!.”
Note: This is what only one person has been able to achieve following a well-designed low carbohydrate diet the last 10 weeks, but these results are quite consistent with Virta Health‘s 10-week results from their outpatient study with 238 subjects published in October 2017 and outlined in this post.
Post-publication addendum (August 23, 2019): I was asked on social media yesterday why I didn’t start this young woman on a very low carbohydrate, ketogenic diet from the outset. This is what I replied; “Diabetes Canada has not (yet?) deemed a LC or very LC diet as safe and effective medical nutrition therapy. I start people at 130 g of carbs, then reduce carbs as necessary to achieve clinical outcomes as a prudent approach. Hence why I conclude the article w/ hope of future policy change.“
I partner with people’s GPs and Endocrinologists to enable them to oversee reduction and de-prescription of injected insulin (or other medications that may result in low blood sugar when following a low carbohydrate diet) while their patients follow a well-designed low carbohydrate diet to effectively manage their blood sugar. It is fantastic to see people such as this very determined young woman replicate what hundreds have done under the care of knowledgeable clinicians and as published in an ever increasing number of peer-reviewed studies.
It was so exciting to recently witness hundreds of CDEs in the United States being taught how to use a low-carbohydrate diet and a very low carbohydrate (ketogenic) diet as medical nutrition therapy with people with both type 1 and type 2 diabetes and how to manage the many medications prescribed for people with diabetes (you can read about these two presentation in this post and this one)!
I long for the day that Diabetes Canada releases an update to Clinical Practice Guidelines similar to what the American Diabetes Association (ADA) did last year, which enables clinicians to recommend a low carb or ketogenic diet as a therapeutic option for those with diabetes.
For more information about the clinical changes at the ADA, you can read any one of several articles from April 2019 that are posted under the Science Made Simple tab above, including this one.
If you would like more information about my services, please have a look under the Services tab or in the Shop. If you have questions, please feel free to send me a note using the Contact Me form above and I will reply as soon as I can.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
Two days ago I posted a photo on Instagram, Facebook and Twitter of fresh chicken that I had bought and had cut up into pieces for dinner. Real food is perfectly normal for a Dietitian to post about, right…but the photo was blurred out by Instagram because it contained what it deemed was “sensitive content” that some would find offensive or disturbing? Calling it what it is, this is censorship of real, whole food.
The photo I posted is above.
The caption under the photo indicated that this shouldn’t look foreign and that real chicken comes with a head, feet and bones (in contrast to chicken we buy in a supermarket that usually comes boneless or pre-cut, in Styrofoam trays, and covered in plastic wrap).
Presumably, someone found this photo offensive and reported it to Instagram. I was not notified that the photo had been censored and it looks the same from my end so I wouldn’t have known, but several people that follow me told me that my photo was deemed to contain “sensitive content” and was blurred out.
To anyone viewing the post now, it now looks like this:
This photo contains sensitive content which some people may find offensive or disturbing.
A physician who follows me on Instagram posted the following with regard to the censoring;
“I cannot believe a photo of food is blurred as “sensitive content”. It is absolutely mind boggling. But it’s totally fine to be constantly inundated with ads for crap that make us feel bad about ourselves, making us buy junk we don’t need.“
This physician is right!
There’s a huge difference between real food and the processed food-like substances (“crap”) that we are encouraged to buy and eat (you can read more about telling the difference between these in this previous article).
The two photos that I posted of chickenbefore and after being cut up has been censored on Instagram because in contains “sensitive content which some people may find offensive or disturbing“.
Do you know what I consider offensive and disturbing?
I find people having to have toes amputated because of uncontrolled diabetes offensive.
I find obese people trying desperately to lose weight, yet finding themselves unable to curb an insatiable craving for processed food that was deliberately created by its producers, disturbing.
I find the fact that many young children in Canada and the US (and likely in many other countries) think of chicken as something that comes boneless, deep fried in batter and packaged in small individual packages with various flavours of sweetened sauce to dip it in, disturbing.
I find pea protein isolate, industrial seed oil, methyl cellulose and a host of other processed ingredients masquerading in the meat counter, offensive. But please don’t misunderstand…
I have absolutely no problem with vegetarians and vegans having a wide variety of plant-based food available to eat as alternatives to animal-based foods, but it should not be marketed to consumers as “meat”, but ‘better’.
It may be “better” or “ultra” or “beyond” for those who choose a plant-based lifestyle, but an ultra-processed mixture of pea protein isolate, canola oil, refined coconut oil, cellulose from bamboo, methylcellulose, potato starch, maltodextrin, yeast extract, sunflower oil, vegetable glycerin, dried yeast, gum arabic along with seasoning and flavourings is not ‘better’ or preferable to whole, real food with a single ingredient, “beef”.
These are choices…
…and people have the right to choose what they want to eat, without condemnation and judgement.
There is no one-sized-fits-all-diet and individuals who choose to eat meat, fish or poultry should not be vilified or censored for doing so.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This past weekend, thousands of American Certified Diabetes Educators (CDE) gathered at the American Association of Diabetes Educators (AADEs) annual conference in Houston, Texas. Objectives of the conference were for CDEs to learn how to implement novel and innovative ways to advance chronic disease prevention and management, and one of those novel ways was through the use of a Low Carbohydrate Diet.
It is very exciting that CDEs are now learning how to implement the American Diabetes Association’s (ADA) new 2019 Standards of Medical Care in Diabetes that was released this past December and which includes use of a low carbohydrate diet (you can read more about thathere).
This conference provided education to enable CDEs to apply the content outlined in the ADA’s April 18, 2019 Consensus Report, which added the use of a very low carbohydrate (ketogenic) diet of 20-50 grams of carbs to the choice of meal patterns to manage both type 1 and type 2 diabetes. You can read more about the Consensus Report here.
As mentioned in the previous post, there were two Educational Sessions this past Saturday, August 11, 2019 about the use of a Low Carbohydrate Diet to manage and treat diabetes. The first session was titled Low Carbohydrate Diets; Fad or Evidence Based Course of Action and was given by Dr. Jim Painter, PhD, RD and Professor Emeritus from Eastern Illinois University, in Charleston, Illinois and this article covers that presentation in detail, including each of the slides and references used.
The second session was titled Person-Centered Implementation of Low Carbohydrate Eating Plans and was given as a joint-session by Dawn Noe, RDN, CDE and Diana Isaacs, PharmaD, CDE, both from Cleveland Clinic Diabetes Center. This second session is the subject of this article.
Copies of the slides and speaking notes for this presentation were sent to me by Dawn Noe, RDN, CDE. Many thanks to her and her colleague Diana Isaacs, PharmaD, CDE for sharing them with us!
The first part of the presentation was given by Registered Dietitian Nutritionist Dawn Noe and is covered in Part A and the second part was given by Doctor of Pharmacy Diana Isaacs and is covered in Part B.
Note: In a few places below, I have added my own clarifications that are clearly marked as *Note (bolded red asterisk *).
Person-Centered Implementation of Low Carbohydrate Eating Plans
Slide 1
The first slide was a disclosure of financial relation / financial conflict of interest, as well as a statement of non-endorsement of products.
Slide 2 – The second slide was a photo of each of the presenters, along with their credentials.
Part A: Nutritional Approach – Dawn Noe, RD, CDE
Slide 3 – list of learning objectives.
Key Points from the American Diabetes Association’s Consensus Report
Slide 4 – Summarized some key points from the American Diabetes Association’s (ADA) Consensus Report
(Evert AB et al. Diabetes Care 2019; 43: 731-754.)
Speaking Point Summary
There is no ‘ideal percentage of carbs’ shown in the literature, but despite this
many people with diabetes are told to eat ~60 grams of carbs at each meal, assuming 3 meals per day.
These numbers are essentially calculated to be 50% of the calories coming from carbohydrate on a 1500 calorie meal plan.
The 130 grams of carb per day recommended for adults without diabetes (which is determined in part by the brain’s requirement for glucose) can be fulfilled by the body’s metabolic processes with include glycogenolysis, gluconeogenesis, and/or ketogensis in the setting of very low dietary carbohydrate intake.
Note: This previous article outlines the ADA’s updated position that the brain’s need for glucose can be fulfilled by the body.
Slide 5 – The Evidence for Low Carb in Type 2 Diabetes and Type 1 Diabetes
Speaking Point Summary
Low carb and very low carb eating patterns are among the most studied eating patterns for type 2 diabetes (T2D).
Long-term outcomes of Virta Health’s 2-year data published in May 2019 were not included in the new ADA Consensus Report.
For those with type 1 diabetes (T1D), no trials met the inclusion criteria for the ADA’s Consensus Report, however one small study limited carbs to 47 grams per day, and another limited carbs to 75 grams per day with positive results relating less glycemic variability, and lower HbA1C respectively.
The ADA Consensus Report states that this evidence suggests that a very low carb eating pattern may have potential benefits for adults with type 1 diabetes, but clinical trials of sufficient size and duration are needed to confirm prior findings.
From 2019 Standards of Care
Providers should maintain consistent medical oversight and recognize that certain groups are not appropriate for low-carbohydrate eating plans, including pregnant or lactating women, children, people who have renal disease or disordered eating behavior.
Low carb and very low carb eating plans should be used with caution for those taking SGLT2 inhibitors due to potential risk of ketoacidosis.
There is inadequate research about dietary patterns for type 1 diabetes to support one eating plan over another at this time.
Slide 6 – Different Ways to Define “Low Carb”
Speaking Points Summary
In the ADA’s Consensus Report, Nutrition Therapy for Adultsincluded 2 meta-analysis where “low carb” was defined differently (≤ 45% calories, < 40% of calories) and 1 meta analysis where “ketogenic” was defined as 5-10% calories / ~20-50 grams carbohydrate per day.
In general, the presenters define “low carb” as being ~50 – 130 grams carbs per day, since < 50 grams of carbs could be a ketogenic for some people.
Feinman et al defined three categories of reduced-carbohydrate diets:
(a) very low carbohydrate ketogenic: carbs limited to 20—50 g per day or < 10% of total energy intake.
(b) low carbohydrate: carbs limited to < 130 g per day or < 26% of total energy intake.
(c) moderate carbohydrate: carbs limited to 130—225 g per day or 26—45% of total energy intake.
(Feinman RD, Pogozelski WK, Astrup A, Bernstein RK, Fine EJ,Westman EC, et al. Dietary Carbohydrate Restriction as the First Approach in Diabetes Management: critical review and evidence base. Nutrition. 2015;31(1):1—13.)
Slide 7 – Teaching Low Carb
Speaking Points Summary
Food Lists: customize to each patient / client. Some people prefer to stop buying / eating certain foods which automatically limits their carb choices, e.g. they don’t want to buy bread or keep it in the house
Carb Counting: could vary and be personalized depending on the client / patient’s post-prandial (after meal) glucose responses, e.g. up to ___ carbs per day versus set number of carbs at each meal
Food Label Reading: focusing on carbs and/or sugars in the ingredient list
Track Macros: use of an app such as MyFitnessPal or CarbManager, can be individualized to be gluten free, Mediterranean, etc.
Slide 8 – Teaching Low Carb (cont’d) – shows a handout used in practice to show lower carb options for traditional pasta.
Slide 9– Teaching Low Carb – making it easy
e.g. using leftover vegetables from dinner for breakfast, sample meal plans with carb amounts, resources with recipes and pictures, no—cook put together meal ideas.
Slide 10 – Clinical Pearls for Providing Support
real food when possible
option when convenience is needed
ways to make carb foods less carb-based; e.g. substituting plain yogurt with vanilla for sweetened vanilla yogurt
Slide 11 -Low Carb Empowered Eater
This slide gave an example of a person with diabetes who started eating lower carb on his own by using a Continuous Glucose Monitor (CGM).
i.e. eats the topping off a pizza to minimize glucose spike and is empowered to do so because he can see the results in real-time.
Slide 12 -Virta Health Type 2 Diabetes Trial was not included in the ADA’s Consensus Report because subjects self-selected which group they would be in, i.e. not randomized.
However, the 1-year data showed HbA1C declined 1.3% concurrently with elimination of non-metformin medications in the continuous care intervention group which is notable.
The 2-year data was published in 2019, just prior to the ADA Consensus Report but was not included.
Slide 13 – slide from Virta Health
Data from people who completed 2 years of the Virta Health clinical trial (intervention group versus usual care group)
This slide represents the actual percentage point reduction in prescription (Rx) costs, HbA1C and Body Weight of intervention group compared to the usual care group.
Slide 14 – What people think “keto” is, versus what keto actually is.
The idea here is that people think that all one eats on a ketogenic diet is meat, eggs, butter and lots of bacon, but there is a variety of foods one can eat, including vegetables, nuts, avocado (amongst other things).
Slide 15 – Well Formulated Ketogenic Meal Plans
A well formulated, ketogenic meal plans can be a great way for people to learn to eat whole, less-processed, and plant foods such as vegetables, nuts and olives and to learn about carbohydrates; a win-win for people with diabetes.
[*Note: this is not the only way to define a “ketogenic diet”, but the one the presenters use. Some clinicians use a higher protein/lower fat approach. What makes a diet ketogenic is the number of grams of carbs being ; 50 g per day or less, for men / 35 g of carbs per day or less, for women.]
adequate electrolyte supplementation: sodium; 2,000-5,000 mg per day, plus potassium, magnesium
can include sample plans, food lists, recipes, pictures, carb counting, tracking macros
Slide 17 – Ketogenic Meal Plans (cont’d)
Keto meal plans can be customized and individualized to the client’s / patient’s food preferences.
(e.g. gluten free, Mediterranean, etc.)
Slide 18 – Ketogenic Meal Plans – keeping it simple.
Many people benefit from basic simple food lists (eg. a “vegetable” list with types of vegetables, a place for them to list their 5 favourite types, along with some pictures).
These food lists can also be used to teach low carb eating.
Slide 19 – Examples of how to include options such as dessert, alcohol, etc. in very low carb eating plans.
use electrolyte drinks or bone broth to minimize symptoms of “keto flu”
the first week: fat / protein to satiety to address hunger
after the first week: either eat fat until satisfied and/or limit fat and total calories for weight management*
*Note: Some clinicians encourage people to eat lean protein until satiated, then add some fat for taste. Many clinicians do not limit total calories, but focus on increasing satiety instead, as the end result will be a decrease in overall calories (as a result rather than as an input).
Slide 21 – What is an Individualized Plan (slide credit: Shamera Robinson, RDN)
The following components should all be
considered when assessing, teaching and coaching with any nutrition intervention;
energy deficit*
dietary preferences
health literacy / numeracy
resources
food availability
cooking skills
disordered eating
sustainability
*Note: Many clinicians do not create an energy deficit (i.e. do not limit total calories) but focus on increasing satiety. Increasing satiety ends up resulting in an energy deficit as a result, which some clinicians prefer over restricting calories as an input.
Slide 22 – Transitioning to a Low Carb (from a Keto) Meal Plan
Some people will not want to do very low carb / keto diet forever and/or may benefit from taking planned breaks
this requires a period of transitioning from a ketogenic meal plan to other meal plan (e.g. low carb), depending on client / patient’s wishes/needs
transition should be customized to the individual
can be a mixture of carbohydrate food (e.g. 1/2 baked potato*, 1/2 pita bread*) along with low-carb alternatives (e.g. cauliflower “rice”, zucchini “zoodles”)
* Note: in this type of case, some clinicians would recommend low Glycemic Index / high fiber carbohydrates such as winter squash or peas, instead of potato or bread.
Slide 23 – Clinical Pearls for Providing Support
aim for real food when possible
convenience options could be protein shakes, pre-portioned cheese or nuts, ready-made mashed cauliflower, ready-made low-carb pizza or low carb wraps
emphasize protein, fiber, fat for satiety, electrolyte needs
keto dessert ideas
how to handle vacations, emotional / stress eating
consider incorporating “mindful eating” / “intuitive eating”; rating hunger levels to teach clients to listen to their bodies, eat when they are hungry and stop when full*, etc.
*Note: this approach may not be suitable for those with very high insulin levels that drive food cravings, or addiction to specific foods.
Part B: Pharmacology Approach – Diana Isaacs, PharmaD, CDE
Slide 24 – Medication Adjustment for Low Carb Eating
Slide 25 – ADA Consensus Report nutrition guidelines
adopting a very low carb eating plan can cause increased production of urine (diuresis) and a rapid reduction in blood glucose
consultation with a knowledgeable practitioner at the onset is necessary to prevent dehydration, reduce injected insulin and blood sugar lowering medications in order to prevent hypoglycemia (low blood sugar)
(Evert AB et al. Diabetes Care 2019; 43: 731-754.)
Slide 26 – Medication Adjustments for Type 2 Diabetes (T2D)
The first speaking point was to confirm that the patient is truly a type 2 diabetic
i.e. not LADA (Latent Autoimmune Diabetes of Adulthood) which is a form of type 1 diabetes that develops later into adulthood
Medication Adjustments for Type 2 Diabetes (T2D)
limit medications that cause hypoglycemia, such as insulin, sulfonylureas, meglitinides (more on that below)
other medication likely not needed / not preferred: alpha glucosidase inhibitors (prevent carb digestion), thiazolidinediones (TzD), also known as glitazones (more on that below)
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines)
Slide 27 – Medications to Stop on a Very Low Carbohydrate Diet
sulfonylurea, increase insulin release e.g. GlyburideⓇ
meglitinide (also called glinides), e.g. PrandinⓇ
bolus (meal time) insulin
combo insulins: 70/30, convert to basal only
alpha glucosidase inhibitors (acarbose), prevent carbohydrate absorption, e.g. GlucobayⓇ
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines), Murdoch C et al, British Journal of General Practice, July 2019)
Slide 28 – Medications to Use Caution on a Very Low Carbohydrate Diet
Sodium-glucose co-transporter protein 2 inhibitors SGLT-2 inhibitors (also called gliflozins), e.g. InvokanaⓇ, JardianceⓇ
basal insulin (initial 30-50% decrease)
insulin U500: cut dose in half
thiazolidinediones (TzD), also known as glitazones (risk of weight gain)
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines), Murdoch C et al, British Journal of General Practice, July 2019)
Slide 29 – Medications that are Okay to Use on a Very Low Carbohydrate Diet
MetforminⓇ
Glucagon-like peptide 1 inhibitors (GLP-1 agonists) e.g. VictozaⓇ, SaxendaⓇ
Dipeptidyl peptidase 4 inhibitors (DPP-4 inhibitors) e.g. JanuviaⓇ
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines, Murdoch C et al, British Journal of General Practice, July 2019)
Slide 30 – Medications Adjustments for Type 1 Diabetes on a Low Carbohydrate Diet
bolus insulin: may need to intensify carb ratio, ? bolus for protein
monitor ketones
avoid sodium-glucose co-transporter protein 2 inhibitors (SGLT-2 inhibitors), also called gliflozins, e.g. InvokanaⓇ, JardianceⓇ
caution with hybrid closed loop pumps
close follow-up required
(Eisworth M et al, Endocrinol Diabetes Metab Case Rep 2018, 2018:18-0002, Krebs JD et al, Asia Pacific Journal of Clinical Nutrt 2016 25:78-84, Nielsen JV et al Upsala Journal of Medical Sciences 2005; 110 267-273)
Slide 31 – Blood Pressure Medications
important to keep in mind the initial diuretic effect of a low carb or very low carb diet
consider cutting dosage in half or stopping diuretic (e.g. HCTZ or chlorthalidone)
monitor blood pressure
(Hussain TA et al, Nutrition 28 (2012) 1016-1021, Evert AB et al. Diabetes Care 2019; 43: 731-754.)
Slide 32 – Other Concerns
drink > 2 liters (64 oz /) water/day
to avoid muscle cramps, supplement magnesium 200-400 mg/day
watch for deficiency in vitamin K, sodium, chloride, vitamin B12, folate, calcium, vitamin D
(Clinical Guidelines for Therapeutic Carbohydrate Restriction, August 1, 2019, Standard of Care Clinical Guidelines, www.lowcarbusa.org/clinical-guidelines)
Note: Slide 33 and Slide 34 were part of a case study of a 52 year old woman with T2D along with several co-morbid conditions, and on multiple medications who planned to start a ketogenic diet the follow day. The case study reviewed the medications that should be stopped or the dosage changed, and what her new medication regimen would look like. They are not included here.
Many thanks once again to Dawn Noe, RDN, CDE and her colleague Diana Isaacs, PharmaD, CDE for sharing their slides and speaking points with us.
More Info?
If you have been diagnosed with pre-diabetic or as having type 2 diabetes and would like to adopt a low carb diet, I can help.
Please note that I am not a CDE and as a result do not provide clinical services to those with type 1 diabetes, or to those with type 2 diabetes who are currently on insulin or insulin-analogue.
For those with T2D who have only been recently prescribed insulin, I have experience working with people’s endocrinologists and GPs as they seek to transition over to a low carbohydrate / ketogenic diet to manage and treat their diabetes.
You can learn more about my services under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
This weekend, thousands of American Certified Diabetes Educators (CDE) gathered at the American Association of Diabetes Educators (AADEs) annual conference in Houston, Texas.
AADE 2019 Learning Objectives – Page 3 of Final Program
One of the Learning Objectives of the conference was for CDEs to learn how to implement novel and innovative ways to advance chronic disease prevention and management, and one of those novel ways was through the use of a Low Carbohydrate Diet.
CDEs are healthcare professionals from a variety of backgrounds who are specialized in diabetes prevention and management and include Registered Dietitians, Registered Nurses, Pharmacists, Physician Assistants and Nurse Practitioners.
This is very exciting news indeed!
It means that CDEs are now learning how to implement the American Diabetes Association’s (ADA) new 2019 Standards of Medical Care in Diabetes that was released this past December, and whichincludes use of a low carbohydrate diet(you can read more about thathere).
This conference provided education to enable CDEs to apply the content of the ADA’s April 18, 2019 Consensus Report which added the use of a very low carbohydrate (ketogenic) diet of 20-50 grams of carbs to the choice of meal patterns to manage both type 1 and type 2 diabetes. You can read more about the Consensus Reporthere.
Two Educational Sessions on Use of a Low Carbohydrate Diet
AADE 2019 Final Program – page 13 – two low carb educational sessions, Saturday August 10 2019
Saturday, August 11, 2019 there were two Educational Sessions at the AADE 2019 Annual Conference related to therapeutic use of a low carbohydrate diet.
The first session was titled Low Carbohydrate Diets; Fad or Evidence Based Course of Action and was given by Dr. Jim Painter, PhD, RD and Professor Emeritus from Eastern Illinois University, in Charleston, Illinois.
The second session was titled Person-Centered Implementation of Low Carbohydrate Eating Plans and was given by Diana Isaacs, PharmaD, CDE and Dawn Noe, RD, CDE both from Cleveland Clinic Diabetes Center. Link to this presentation, including the slides and speaking notes is at the bottom or this article.
This post is a summary of Dr. Jim Painter’s educational session at the AADE’s 2019 Annual Conference titled Low Carbohydrate Diets; Fad or Evidence Based Course of Action.
Note: Photos of the slides were posted on Twitter® on August 10, 2019 by Jake Kushner, MD (@JakeKushnerMD).
Low Carbohydrate Diets: Fad or Evidence Based Course of Action
Slide 1
Dr. Painter’s first slide demonstrates using National Health and Nutrition Examination Survey (NHANES) data (adapted from Ford 2015 Am J Clin Nutr) how carbohydrate content of the US diet increased dramatically after 1980 and continued high, while protein content (and fat content, not visible in this slide) remained stable.
“The increase in calories during the obesity epidemic was due largely to carbohydrate intake.“
Slide 2
Dr. Painter’s second slide pointed out that not only did carbohydrate consumption increase (dotted graph), the percentage of carbohydrate from fiber decreased (bar graph).
The point Dr. Painter made is that “carbohydrates that lack fiber are high glycemic index” carbs — and these highly refined carbs result in a higher increase in blood sugar than carbohydrates that contain fiber.
Slide 3
Dr. Painter then defined what a “low carbohydrate diet” is according to the American Diabetes Association and the Academy of Nutrition and Dietetics.
What is a low-carbohydrate diet?
The American Diabetes Association defines a low-carbohydrate diet as a diet that contains < 130 grams of carbohydrate per day (including 25-30 grams of fiber)
i.e. ~100-105 net grams of carbs
Note: Dr. Painter didn’t define a very low carbohydrate diet, which the American Diabetes Association defined in its new Consensus Report as 20-50 g carbs per day. You can read more about thathere.
The Academy of Nutrition and Dietetics defined low carbohydrate diets as ≤ 35% of energy from carbohydrates.
In the scientific literature, low-carbohydrate diets range from 20 grams of carbohydrate per day up to ~150 grams per day (~20-25% of energy).
Slide 4
Dr. Painter then explained how low carbohydrate diets seek to minimize insulin secretion in the pancreas via their very low glycemic response, and how the reduced insulin affects;
weight control
type 2 diabetes
coronary heart disease (CHD)
Slide 5
Dr. Painter explained how an initial concern with a low carbohydrate diet was with the higher fat aspect, particularly for weight loss, as fat provides 9 kcals / gram and carbs only provides 4 kcals/grams, however;
Fat slow gastric emptying and stimulates the secretion of cholecystokinin (CCK) and Peptide YY (PYY) — which are satiety hormones that result in people feeling full.
Dietary proteins, short chain fatty acids and free fatty acids increase GLP-1 (which is one of the incretin hormones). Glucagon-like Peptide-1 (GLP-1) acts on the brain to decrease appetite, increase satiety (feeling full) and decrease food intake. You can read more about that here.
Branched Chain Amino Acides (BCAA) found in protein reduces appetite.
Ketone bodies (produced in very low carbohydrate diets) such as beta-hydroxybuterate suppress appetite.
Slide 6
Dr. Painter then outlined the findings of a 2014 study titled Effects of low-carbohydrate and low-fat diets: a randomized trial (Baranna LA, Hu T, Reynalds K et al, Ann Intern Med. 2014 Sep 2;161(5):309-18. doi: 10.7326/M14-0180).
Participants in this study had a BMI of between 30-45 kg per meter squared (meaning they were obese to morbidly obese), but did not have any metabolic diseases such as diabetes or cardiovascular disease (CVD).
The low carb group had carbohydrate intake of < 40 grams/day and the low fat group was allowed 55% of energy from carbohydrate (which is with the Recommended Dietary Intake of 45-55%), but restricted calories from fat.
There were 59-60 participants in both the low carb or low fat group…
Slide 7
…and after a year, those in the low carb group had a greater decrease in weight, fat mass, ratio of total-high-density lipoprotein (HDL) cholesterol, triglyceride level, and greater increases in HDL cholesterol level than those on the low-fat diet.
Dr. Painter highlighted that at the end of 12 months; these were the results of the two groups;
Low-carbohydrate diet
5.3 kg weight loss
1.2 kg loss of fat mass
1.3 gain lean body mass
Low-fat diet
1.8 kg weight loss
0.3% gain in fat mass
0.4% loss in lean mass
Slide 8
Dr. Painter then went over the results from a 2006 study by Gannon MC and Nutall FQ, titled Control of Blood Glucose in Type 2 Diabetes Without Weight Loss by Modification of Diet Composition (Nutr Metab. (2006 Mar 23;3:16. doi: 10.1186/1743-7075-3-16) which found that even without weight loss, altering the diet composition to a low carb diet (carbs < 20% of energy) can enable people with type 2 diabetes to lower their blood sugar level without weight loss or diabetes medications, and achieve significantly better glycated hemoglobin (HbA1C) levels.
Slide 9
In this slide, Dr. Painter addressed a prevailing concern among many healthcare professionals that a low carbohydrate diet increase cardiovascular disease risk.
Does a Low-Carbohydrate Intake Increase Cardiovascular Disease Risk?
Dr. Painter outlined that a 2017 by Chui demonstrated that HDL cholesterol increases in a low carb diet and that while LDL cholesterol does increase, it tends to be the large buoyant LDL that increase, with no change in the athlersclerotic small, dense LDL.
He also outlined that a 2012 meta-study analysis of 19 randomized control trials (RCTs) by Santos et al reported a global decrease in triglyceride levels of 29.71 mg/dL (0.34 mmol/L) and that a 2014 study by Bazzano reported that a low carbohydrate diet had a greater decrease in 10-year cardiovascular heart disease (CHD) risk score based on the Framingham Risk Score, than those on the low fat diet.
Slide 10
Dr. Painter then elaborated on a study from 2008 by Forsythe CE et al titled Comparison of Low Fat and Low Carbohydrate Diets on Circulating Fatty Acid Composition and Markers of Inflammation that was published in the Journal Lipids (Lipids. 2008 Jan;43(1):65-77. Epub 2007 Nov 29).
In this study overweight men and women were put on either a low carb or low fat ~1500 kcal / day diet for 12 weeks. Results indicated that the low carb diet had a 3-fold higher dietary intake of saturated fatty acids (SFA) (36 grams/day versus 12 grams/day) yet the low carb group had a significantly greater reduction in their serum saturated fat levels.
That is, people in the low carb group they ate 3x the amount of saturated fat yet had a significantly greater reduction in their blood levels of saturated fat.
Slide 11
Dr. Painter then reviewed a 2004 study by Volek JS et al titled Dietary Carbohydrate Restriction Induces a Unique Metabolic State Positively Affecting Atherogenic Dyslipidemia, Fatty Acid Partitioning, and Metabolic Syndrome which indicated how a very low carbohydrate (VLCKD) compared to a low carbohydrate diet (LCD) significantly improved body mass, abdominal fat, triglycerides (TG), ApoB:ApoA1 ratio, small dense LDL, TG:HDL ratio, insulin levels, and HOMA-IR score.
Slide 12
Dr. Painter then looked at the “why” for using a low carbohydrate diet for type 2 Diabetes Mellitus (T2DM).
Dr. Painter outlined the results of a 2015 study titled Prevalence of and Trends in Diabetes Among Adults in the United States, 1988-2012 by Menke A et al (JAMA. 2015 Sep 8;314(10):1021-9. doi: 10.1001/jama.2015.10029) which indicated that;
“Recent data indicates 52% of the American population is either diabetic or prediabetic. The cost of diabetes (in the US) is estimated to be over $320 billion annually”.
Slide 13
Dr. Painter then cited a 2013 systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes (Ajala et al) titled Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes, Am J Clin Nutr. 2013 Mar;97(3):505-16. doi: 10.3945/ajcn.112.042457. Epub 2013 Jan 30.).
This paper looked at 20 randomized control trials (RCTs) across 3460 randomly assigned subjects and which found that a low-carbohydrate diet, low-GI diet, Mediterranean diet, and high-protein diet all led to a greater improvement in glycemic control and with the low-carbohydrate diet and Mediterranean diet leading to greater weight loss.
Dr. Painter indicated that each of these dietary philosophies show effectiveness of lower carbohydrate and lower GI diets for treating T2DM.
Slide 14
Dr. Painter then outlined the findings of a 2017 study by Snorgaard O et al titled Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes (BMJ Open Diabetes Research and Care 2017;5:e000354. doi: 10.1136/bmjdrc-2016-000354) where both the carbohydrate-restricted and low-fat diets were able to produce clinically meaningful HbA1C reductions of ≥ 0.5%, however the low carbohydrate diet produced a greater reduction of up to 0.19% over 6 months.
“Upon subgroup analysis, it was found that carbohydrate of < 26% of energy produces the greatest reduction whereas carbohydrate reduction of 26-45% of total energy produces no additional benefit over low-fat diets.”
Slide 15
In Dr. Painter’s next slide, he summarized the finding of a 2018 systematic review and meta-study paper by Sainsbury E et al with respect to medication use, titled Effect of Dietary Carbohydrate Restriction on Glycemic Control in Adults with Diabetes: A systematic review and meta-analysis (Diabetes Res Clin Pract. 2018 May;139:239-252. doi: 10.1016/j.diabres.2018.02.026. Epub 2018 Mar 6).
“There was a greater reduction in medication use for participants on carbohydrate-restricted diets compared with high carbohydrate diets at every time point.”
reduced the dosage of oral medication and/or insulin
or an elimination of medication
Sainsbury 2018
Slide 16
Dr. Painter then outlined some highlights of a 2015 review paper titled Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base by Feinman RD, et al; namely;
The benefits of carbohydrate restriction in diabetes are immediate and well- documented
Dietary carbohydrate restriction reliably reduces high blood glucose, does not require weight loss…and leads to the reduction or elimination of medication.
Slide 17
Dr. Painter next slide highlighted Table 2 from the consensus report of October 2018 by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) where they classified a low carbohydrate diet as Medical Nutrition Therapy (covered in this previous article). Table 2 outlines the full range of therapeutic options, including lifestyle management, medication and obesity management and lists a low carbohydrate diet as one of the available therapeutic diets.
Slide 18
Dr. Painter then went over the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes which was released on December 17, 2018 (covered in this previous article) and which outlined key recommendations regardless which of the different types of approved eating patterns people choose, namely;
“As for all individuals in developed countries, both children and adults with diabetes are encouraged to minimize intake of refined carbohydrate and added sugars and instead focus on carbohydrate from vegetables, legumes, fruit, dairy (milk and yogurt) and whole grains. The consumption of sugar-sweetened beverages (including fruit juices) and processed “low fat” or “non-fat” food products with high amounts of refined grains and added sugars is strongly discouraged.”
Slide 19
The next slide was a continuation from the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes, and Dr. Painter highlighted that;
“In addition, research indicates that low carbohydrate eating plans may result in improved glycemia and have the potential to reduce anti-hyperglycemic medications for individuals with type 2 diabetes.”
Slide 20
Dr. Painter next highlighted the necessity of medication adjustment soon after initiating a low carbohydrate diet in order to prevent hypoglycemia.
Box 1 from Adapting Diabetes Medication for Low Carbohydrate Management of Type 2 Diabetes: a practical guide by Murdoch C et al (2019), was presented and is as follows;
Summary guidance on adapting diabetes medication for low carbohydrate management of type 2 diabetes
Dr. Painter highlighted the following on his slide;
“Practice expertise suggests a 50% reduction of daily insulin dose at initiation of the low carbohydrate diet (LCD) is appropriate in most cases. In individuals whose HbA1C is markedly elevated, a smaller reduction of perhaps 30% may be appropriate, with further reductions over time…”
Slide 21
Dr. Painter’s next slide simply read;
“Be encouraged! Reversal of Type 2 Diabetes??”
…as if to challenge his listeners to consider that diabetes reversal using a low carbohydrate diet is possible.
Slide 22
Dr. Painter then reviewed the DiRECT randomized control trial by Lean et al, titled Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial (The Lancet, 391 (10120). pp. 541-551. ISSN 0140-6736).
In that study, the 300+ participants from almost 50 primary care sites in the UK were randomly assigned to either a weight management program (which was the intervention group) or to best-practice care by guidelines (which was the control group).
Slide 23
Dr. Painter outlined the results of the DiRECT trial, which found that at 12 months, 24% of the participants in the intervention group lost 15 kg or more, with no weight loss in the control group.
Diabetes remission varied with weight loss;
no remission in those who gained weight
7% achieved remission with under 5 kg of weight loss
34% achieved remission lost between 5—10 kg
57% achieved remission with 10—15 kg loss
86% achieved remission with weight loss of 15 kg or more
“Our findings show that, at 12 months almost half of participants achieved remission to a non-diabetic state and off anti-diabetic drugs. Remission of type 2 diabetes is a practical target for primary care“.
Slide 24
Dr. Painter then proceeded to addressed 3 common misperceptions about low carbohydrate diets, namely;
A low carbohydrate diet puts participants at risk of ketoacidosis…
Low carbohydrate diets ignore the principles of moderation and result in a nutrient-deficient diet…
The majority of weight loss comes from water and lean body mass…
Slide 25 – addressing the misperception that a low carbohydrate diet puts participants at risk of ketoacidosis…
Dr. Painter cited a 2013 study titled Long Term Successful Weight Loss with a Combination Biphasic Ketogenic Mediterranean diet and Mediterranean Diet Maintenance Protocol by Paoli A et al (Nutrients. 2013 Dec 18;5(12):5205-17. doi: 10.3390/nu5125205).
Using the data from that study, Dr. Painter demonstrated how the glucose range, insulin rang and ketone body range in a ketogenic diet is nothing like the ranges in Diabetic Ketoacidosis.
Slide 26 – addressing the misperception that low carbohydrate diets ignore the principles of moderation and result in a nutrient-deficient diet…
Dr. Painter cited the paper by Zinn C et al, titled Assessing the Nutrient Intake of a Low-Carbohydrate, High-Fat (LCHF) Diet: a hypothetical case study design and highlighted that despite macronutrient proportions not aligning with current national dietary guidelines, that when well-designed a low carbohydrate diet provides all of the essential micronutrients needed by the body.
Even at the lower end of the carbohydrate spectrum, you can still get all of the essential nutrients and energy your body needs by selecting from a broad array of nutrient-dense vegetables and fruit, e.g.:
raspberries
strawberries
blueberries
tomatoes
olives
avocados
plain greek yogurt
nuts/seeds
“Zinn et all demonstrated that a well-planned Low-Carbohydrate, High-Fat (LCHF) meal plan can be considered micronutrient replete.”
Slide 27 – addressing the misperception that the majority of weight loss comes from water and lean body mass…
Dr. Painter cited the 2014 study by Bazzano LA et al, titled Effects of Low-Carbohydrate and Low-Fat Diets: a randomized trial which found that of the ~60 subjects randomized to either the low-carbohydrate diet (<40 grams/day) or low-fat diet (<30% of daily energy intake from total fat [<7% saturated fat]) which found that at 12 months, participants on the low-carbohydrate diet lost 3.5 kg more weight and lost 1.5% more fat mass, than those in the low-fat diet group.
Slide 28
Dr. Painter concluded his talk by saying that he feels that most low carbohydrate diets are ‘harmful in practice’ because they are low in fiber, but that that can be addressed by;
Start with a foundation of 6-8 servings of non-starchy, fiber-rich vegetables (~ 15 grams net carbs per day)
Include additional calories from added fats. Nuts and seeds can provide additional fiber
Depending on weight loss and healthy goals, low glycemic carbohydrates found in whole grains and fruit can be used to provide additional fiber.
For those who want to make sure to meet current fiber consumption recommendations while eating a low carbohydrate diet, please have a look at the article I wrote titled Surprising Ways to Get Adequate Fiber Eating Low Carb High Fat (LCHF), located here.
Final Thoughts…
Just a few years ago, it was viewed as quite ‘radical’ for healthcare professionals to consider a well-designed low carbohydrate or very low carbohydrate (ketogenic) diet as therapeutic, but now organizations in Europe (such as the EASD), the UK and Australia — along with the American Diabetes Association (ADA) consider both meal patterns Medical Nutrition Therapy for management of diabetes and for treating overweight and obesity.
What an exciting time!
Here it is, less than a year after the ADA released their 2019 Standards of Medical Care in Diabetes and only 4 months after the ADA released its Consensus Report and this past weekend, thousands of American Certified Diabetes Educators (CDE) gathered at their annual conference znd ~500 learned how to implement a low carbohydrate or ketogenic diet to advance chronic disease prevention and management.
It is my sincere hope that it won’t be much longer before clinicians in Canada are provided with diabetes Standards of Care that support the use of a well-designed low carbohydrate and very low carbohydrate diet as therapeutic options.
More Info?
If you have been diagnosed as being pre-diabetic or as having type 2 diabetes and would like support to put the symptoms into remission by implementing a low carbohydrate or very low carbohydrate eating pattern, then I can help.
I also don’t believe in a ”one-sized-fits-all” approach and will work with you to design an individual Meal Plan that will meet your needs. You can learn more about my services under the Services tab or in the Shop and if you have questions, please feel free to send me a note using the Contact Me form above.
UPDATE (August 16 2019): You can find the second presentation from the American Certified Diabetes Educators conference here. This is where hundreds of CDEs learned about dietary and medication management of lowcarb and ketogenic diets from a Registered Dietitian and Dr. of Pharmacy with CDE certification.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.
References
American Association of Diabetes Educators, Annual Conference, Houston Texas, Friday August 9 – Monday August 12, 2019, https://www.aademeeting.org/
This recipe is posted as a courtesy to those following a variety of low-carb and ketogenic diets (not necessarily Meal Plans designed by me). This recipe may or may not be appropriate for you.
INTRODUCTION: Years ago, I used to make my own homemade yogurt using the pilot light in my gas oven to incubate it, but that was a long time ago. Unfortunately, my last few homes had electric stoves and not gas and purchasing yogurt just seemed more ‘practical’. Recently I switched from cow’s milk to goat’s milk to avoid A1 beta-casein that was negatively impacting my joints (you can read about A1 beta casein here), so I recently decided to start making my own Greek goat yogurt. My first reason to make my own was because the goat yogurt available on the market did not have the classic thick texture of “real” Greek yogurt, and the second reason was that making my own — even with premium milk such as goat milk or A2 beta-casein milk from heirloom cows still costs half of what it does in the store. Finally, making it myself, I can control what’s in it. Mine has no skim milk powder or gelatin; it’s just full-fat milk and yogurt culture.
Homemade Goat-milk Greek Yogurt
Oven Method
The first time I made yogurt recently, I incubated it in my electric oven by preheating it to 200° F (93°C), turning the heat off and allowing it to cool to 110° F (43° C). Then I turned the oven light bulb on to maintain the ambient temperature, and since ovens are so well insulated, it worked as well as it used to in my old gas oven years ago.
Crock-pot® and Inkbird® Method
When I posted my first results, someone online suggested I used an old Crock-pot® to incubate it, but when I had investigated that idea previously, the lowest setting on mine was too hot for the purpose. The “Lo” setting ranged between 140-145°F (60-63°C) which would kill the bacterial culture, so that’s why I used my old oven method.
This person suggested I purchase an Inkbird® plug and play temperature controller that could be set up between the Crock-pot® and the power supply, in order to maintain the temperature at a steady 110° F (43°C) for the duration of the incubation time. That sounded terrific so I ordered one online.
The cool thing is the Inkbird® temperature controller can also be used to turn the same old Crock-pot®into sous-vide; which I will definitely try at some point, too!
Below are step-by-step instructions for making both regular and Greek yogurt.
Homemade Yogurt – Crock-Pot® and Inkbird® controller method
Pour 3 liters of fresh goat milk (or other mammal milk) into a heavy bottom pot.
Heat the milk at a medium-low heat until the milk reaches 180° F (82 ° C), stirring occasionally. It takes a while, but don’t rush it by turning it up or it will scald on the bottom of the pot, losing some of the valuable thickening protein. Once it reaches temperature, turn the heat down just enough to maintain the temperature stable for 20 minutes.* * Heating the milk is essential even if the milk is pasteurized, as it transforms the proteins. Holding the milk at 180° F (82°C) for 20 minutes makes the difference between runny and full-bodied yogurt (even if you don’t strain it to make it Greek-style).
Pour the hot milk into the removable ceramic insert of the Crock-pot®, then cover it and let it cool until it reaches 110-115° F (43°- 46°C) . Since this can take several hours, I use a cold water bath to speed things up if I want to get it incubating sooner and stir it with a sterilized stainless steel whisk as it sits in the cold water, to make sure it cools uniformly so the thermometer reading is accurate.
Once the milk has cooled to just above 110°F (43°C), remove 1 cup of it (250 ml) to a bowl and add 1/2 cup (125 ml) of the starter you are using. I use a previous batch of my own yogurt, but start the first batch with some fresh commercial goat yogurt. Remember that each type of milk needs a different type of starter so be sure to buy one that is made from the same type of milk as you’re using. Stir the starter and cup of warmed milk back into the Crock-pot® and stir gently to distribute it evenly.
Put the insert into the base of the Crock-pot® and insert the plug of the Crock-pot® into the power receptacle of the Inkbird® thermometer controller, then plug the controller into the wall.
Set the temperature on the controller to 110° F (43°C) for 12 hours and then have it go off.
Insert the probe into the warm milk that has the starter added.
After 12 hours, remove the probe and unplug the Inkbird®.
At this point, you have plain yogurt which can be packaged up into containers and cooled in the refrigerator for 12 hours before eating.
For Greek Yogurt
Line a stainless steel colander or strainer with a clean piece of white cotton cloth and attach it firmly to the edges with clips.
Insert the strainer or colander into a large bowl that will catch the large amount of whey that will drain off. Keep in mind, about 35-40% of the finished yogurt is whey, which is what is being removed by draining.
amount of whey after 1 hour of draining
Pour in yogurt and while it is draining, cover the strainer.
Let the whey drain out in the fridge or in an oven that has been warmed and cooled to 110°F (43°C) and has the light bulb on. Remember, that while straining, the yogurt needs to be either in the fridge or at the same temperature it incubates at, to keep it out of the temperature “danger zone”.
Mine goes into a warmed, cooled oven because my fridge always has too much food in it to accommodate a large bowl!
Drain the yogurt until the mixture is the thickness you like. I drain mine for 12 hours so that it is very thick.
Package it up into sterilized containers with covers and let it chill 12 hours in the fridge before eating.
Enjoy as is, or with a sprinkle of hemp hearts and berries.
Macros – 3/4 cup / 175 ml of plain Greek Goat Yogurt
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.





 Prepare an 7 ” non-stick spring-form pan by lining with parchment paper and spraying well with a coconut oil spray.
Prepare an 7 ” non-stick spring-form pan by lining with parchment paper and spraying well with a coconut oil spray.

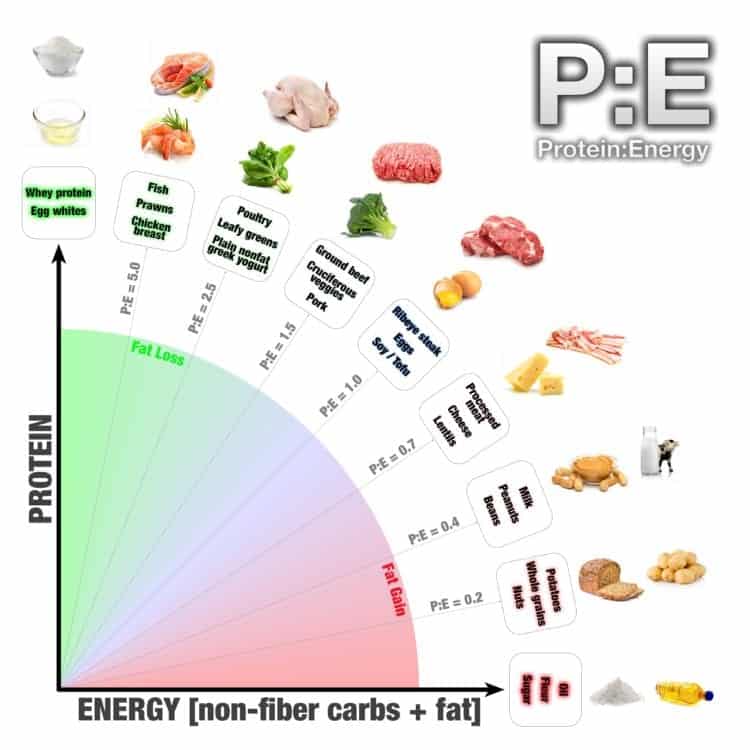







 For those that are unfamiliar with “girdles”, they are essentially torture devices that women squeezed into to arrange their fat in a more acceptable manner, and at least keep it from jiggling where it offended others and embarrassed the individual. Wearing a girdle wasn’t about health; but appearance.
For those that are unfamiliar with “girdles”, they are essentially torture devices that women squeezed into to arrange their fat in a more acceptable manner, and at least keep it from jiggling where it offended others and embarrassed the individual. Wearing a girdle wasn’t about health; but appearance.

 Embracing my health is a bit like embracing my curls. I am no longer the obese Dietitian with type 2 diabetes and high blood pressure and I can share my story with others; to encourage them that I understand, have “been there” and also that I have the knowledge to help. But just like those who embraced their own curls before me and encouraged me to do so too, each person has their own journey. My role is to support people in theirs.
Embracing my health is a bit like embracing my curls. I am no longer the obese Dietitian with type 2 diabetes and high blood pressure and I can share my story with others; to encourage them that I understand, have “been there” and also that I have the knowledge to help. But just like those who embraced their own curls before me and encouraged me to do so too, each person has their own journey. My role is to support people in theirs.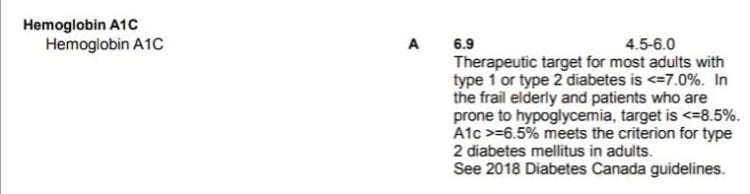





















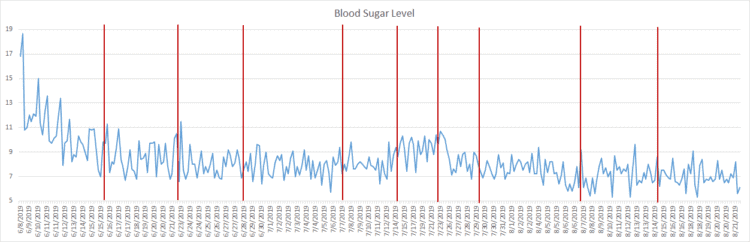
 The photo I posted is above.
The photo I posted is above.

 The first slide was a disclosure of financial relation / financial conflict of interest, as well as a statement of non-endorsement of products.
The first slide was a disclosure of financial relation / financial conflict of interest, as well as a statement of non-endorsement of products. Slide 2
Slide 2
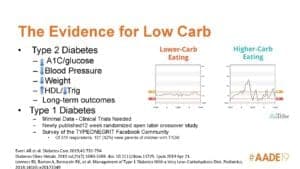
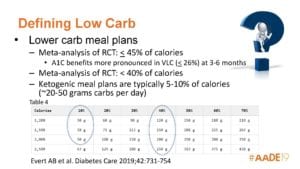 Slide 6 – Different Ways to Define “Low Carb”
Slide 6 – Different Ways to Define “Low Carb” Slide 7 – Teaching Low Carb
Slide 7 – Teaching Low Carb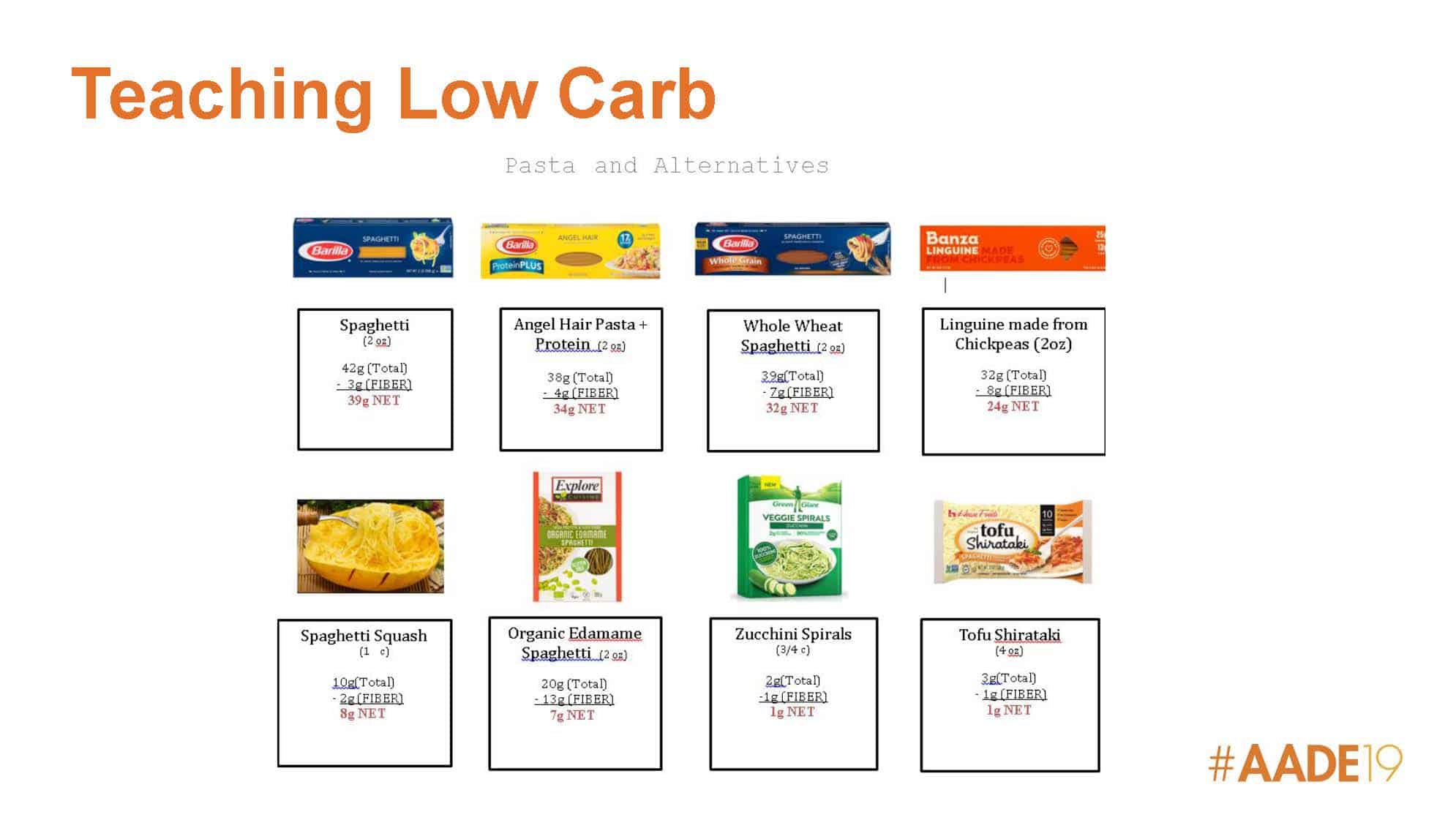

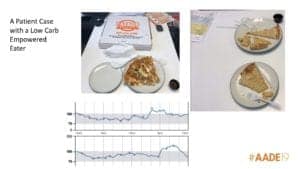
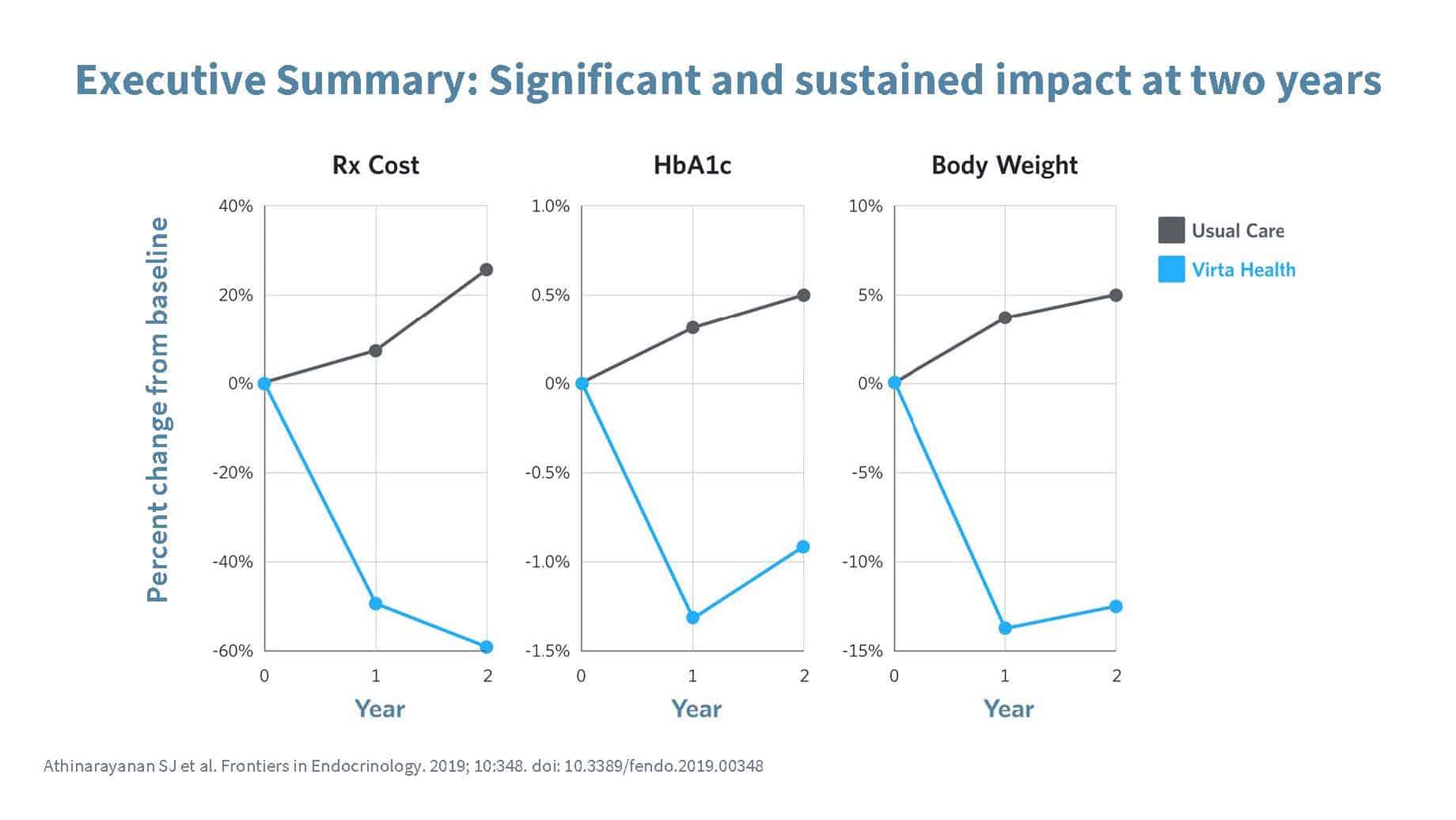
 The idea here is that people think that all one eats on a ketogenic diet is meat, eggs, butter and lots of bacon, but there is a variety of foods one can eat, including vegetables, nuts, avocado (amongst other things).
The idea here is that people think that all one eats on a ketogenic diet is meat, eggs, butter and lots of bacon, but there is a variety of foods one can eat, including vegetables, nuts, avocado (amongst other things). Well Formulated Ketogenic Meal Plans
Well Formulated Ketogenic Meal Plans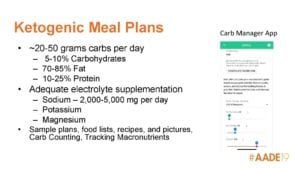
 Slide 17 – Ketogenic Meal Plans (cont’d)
Slide 17 – Ketogenic Meal Plans (cont’d)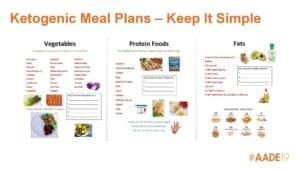

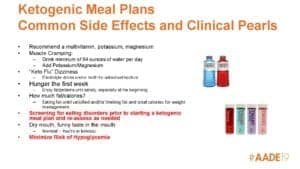
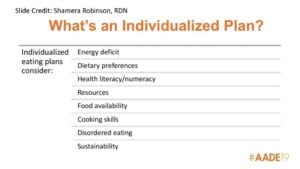
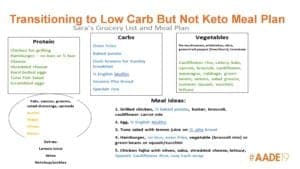
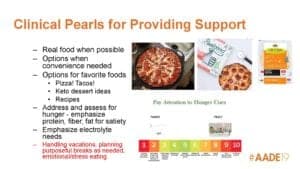

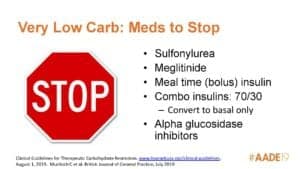
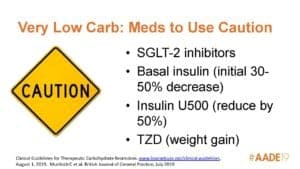 Slide 28 – Medications to Use Caution on a Very Low Carbohydrate Diet
Slide 28 – Medications to Use Caution on a Very Low Carbohydrate Diet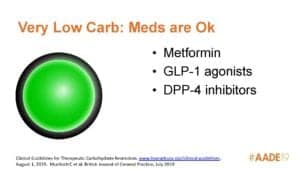 Slide 29 – Medications that are Okay to Use on a Very Low Carbohydrate Diet
Slide 29 – Medications that are Okay to Use on a Very Low Carbohydrate Diet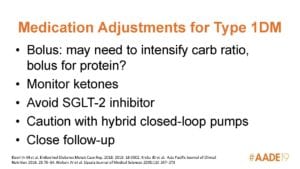
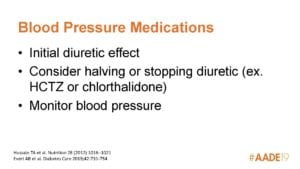
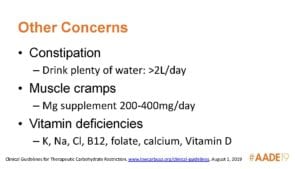
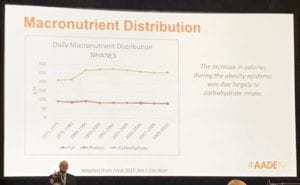
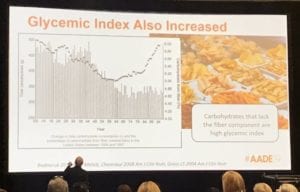 Dr. Painter’s second slide pointed out that not only did carbohydrate consumption increase (dotted graph), the percentage of carbohydrate from fiber decreased (bar graph).
Dr. Painter’s second slide pointed out that not only did carbohydrate consumption increase (dotted graph), the percentage of carbohydrate from fiber decreased (bar graph).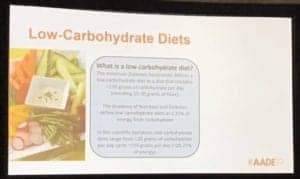
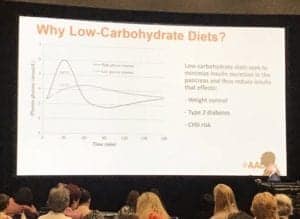 Dr. Painter then explained how low carbohydrate diets seek to minimize insulin secretion in the pancreas via their very low glycemic response, and how the reduced insulin affects;
Dr. Painter then explained how low carbohydrate diets seek to minimize insulin secretion in the pancreas via their very low glycemic response, and how the reduced insulin affects;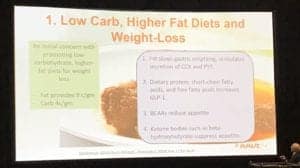 Dr. Painter explained how an initial concern with a low carbohydrate diet was with the higher fat aspect, particularly for weight loss, as fat provides 9 kcals / gram and carbs only provides 4 kcals/grams, however;
Dr. Painter explained how an initial concern with a low carbohydrate diet was with the higher fat aspect, particularly for weight loss, as fat provides 9 kcals / gram and carbs only provides 4 kcals/grams, however;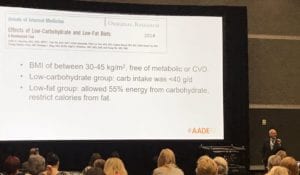 Dr. Painter then outlined the findings of a 2014 study titled Effects of low-carbohydrate and low-fat diets: a randomized trial (Baranna LA, Hu T, Reynalds K et al, Ann Intern Med. 2014 Sep 2;161(5):309-18. doi: 10.7326/M14-0180).
Dr. Painter then outlined the findings of a 2014 study titled Effects of low-carbohydrate and low-fat diets: a randomized trial (Baranna LA, Hu T, Reynalds K et al, Ann Intern Med. 2014 Sep 2;161(5):309-18. doi: 10.7326/M14-0180).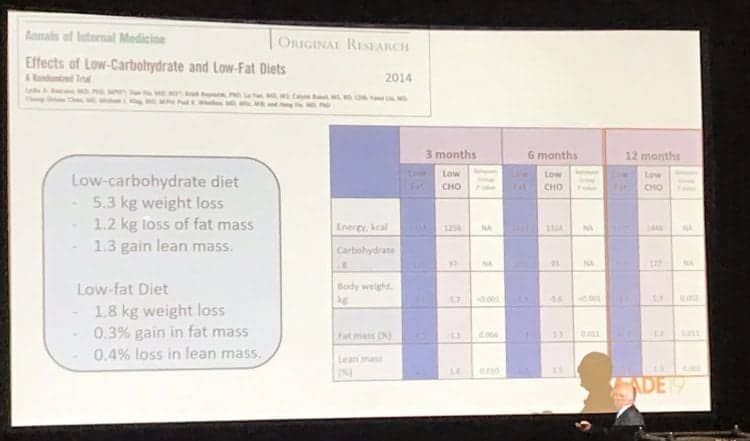
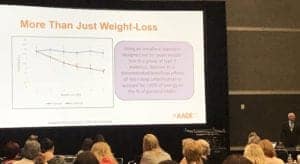 Dr. Painter then went over the results from a 2006 study by Gannon MC and Nutall FQ, titled Control of Blood Glucose in Type 2 Diabetes Without Weight Loss by Modification of Diet Composition (
Dr. Painter then went over the results from a 2006 study by Gannon MC and Nutall FQ, titled Control of Blood Glucose in Type 2 Diabetes Without Weight Loss by Modification of Diet Composition ( In this slide, Dr. Painter addressed a prevailing concern among many healthcare professionals that a low carbohydrate diet increase cardiovascular disease risk.
In this slide, Dr. Painter addressed a prevailing concern among many healthcare professionals that a low carbohydrate diet increase cardiovascular disease risk.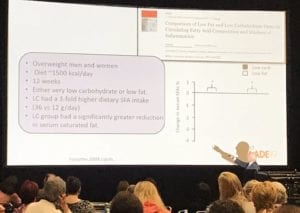 Dr. Painter then elaborated on a study from 2008 by Forsythe CE et al titled Comparison of Low Fat and Low Carbohydrate Diets on Circulating Fatty Acid Composition and Markers of Inflammation that was published in the Journal Lipids (
Dr. Painter then elaborated on a study from 2008 by Forsythe CE et al titled Comparison of Low Fat and Low Carbohydrate Diets on Circulating Fatty Acid Composition and Markers of Inflammation that was published in the Journal Lipids (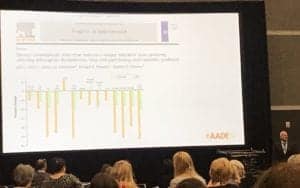 Dr. Painter then reviewed a 2004 study by Volek JS et al titled Dietary Carbohydrate Restriction Induces a Unique Metabolic State Positively Affecting Atherogenic Dyslipidemia, Fatty Acid Partitioning, and Metabolic Syndrome which indicated how a very low carbohydrate (VLCKD) compared to a low carbohydrate diet (LCD) significantly improved body mass, abdominal fat,
Dr. Painter then reviewed a 2004 study by Volek JS et al titled Dietary Carbohydrate Restriction Induces a Unique Metabolic State Positively Affecting Atherogenic Dyslipidemia, Fatty Acid Partitioning, and Metabolic Syndrome which indicated how a very low carbohydrate (VLCKD) compared to a low carbohydrate diet (LCD) significantly improved body mass, abdominal fat,  Dr. Painter then looked at the “why” for using a low carbohydrate diet for type 2 Diabetes Mellitus (T2DM).
Dr. Painter then looked at the “why” for using a low carbohydrate diet for type 2 Diabetes Mellitus (T2DM).
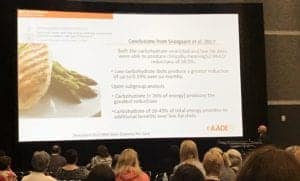
 In Dr. Painter’s next slide, he summarized the finding of a 2018 systematic review and meta-study paper by Sainsbury E et al with respect to medication use, titled Effect of Dietary Carbohydrate Restriction on Glycemic Control in Adults with Diabetes: A systematic review and meta-analysis (
In Dr. Painter’s next slide, he summarized the finding of a 2018 systematic review and meta-study paper by Sainsbury E et al with respect to medication use, titled Effect of Dietary Carbohydrate Restriction on Glycemic Control in Adults with Diabetes: A systematic review and meta-analysis ( Dr. Painter then outlined some highlights of a 2015 review paper titled Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base by Feinman RD, et al; namely;
Dr. Painter then outlined some highlights of a 2015 review paper titled Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base by Feinman RD, et al; namely; Dr. Painter next slide highlighted Table 2 from the consensus report of October 2018 by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) where they classified a low carbohydrate diet as Medical Nutrition Therapy (covered in
Dr. Painter next slide highlighted Table 2 from the consensus report of October 2018 by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) where they classified a low carbohydrate diet as Medical Nutrition Therapy (covered in 
 Dr. Painter then went over the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes which was released on December 17, 2018 (
Dr. Painter then went over the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes which was released on December 17, 2018 ( The next slide was a continuation from the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes, and Dr. Painter highlighted that;
The next slide was a continuation from the 2019 American Diabetes Association’s Lifestyle Management; Standards of Medical Care in Diabetes, and Dr. Painter highlighted that; Dr. Painter next highlighted the necessity of medication adjustment soon after initiating a low carbohydrate diet in order to prevent hypoglycemia.
Dr. Painter next highlighted the necessity of medication adjustment soon after initiating a low carbohydrate diet in order to prevent hypoglycemia.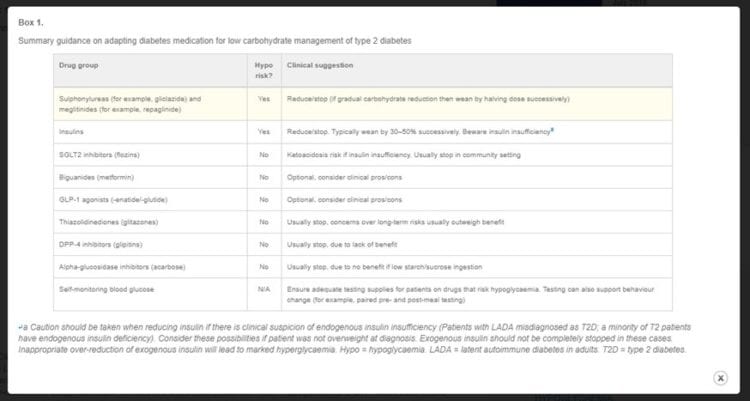
 Dr. Painter’s next slide simply read;
Dr. Painter’s next slide simply read; Dr. Painter then reviewed the DiRECT randomized control trial by Lean et al, titled Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial (The Lancet, 391 (10120). pp. 541-551. ISSN 0140-6736).
Dr. Painter then reviewed the DiRECT randomized control trial by Lean et al, titled Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial (The Lancet, 391 (10120). pp. 541-551. ISSN 0140-6736).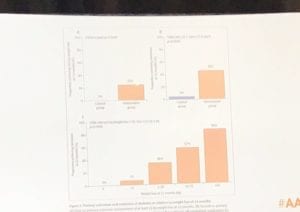 Dr. Painter outlined the results of the DiRECT trial, which found that at 12 months, 24% of the
Dr. Painter outlined the results of the DiRECT trial, which found that at 12 months, 24% of the  Dr. Painter then proceeded to addressed 3 common misperceptions about low carbohydrate diets, namely;
Dr. Painter then proceeded to addressed 3 common misperceptions about low carbohydrate diets, namely;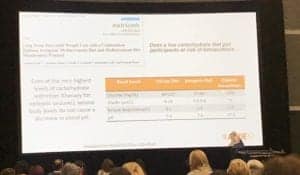 Dr. Painter cited a 2013 study titled Long Term Successful Weight Loss with a Combination Biphasic Ketogenic Mediterranean diet and Mediterranean Diet Maintenance Protocol by Paoli A et al (
Dr. Painter cited a 2013 study titled Long Term Successful Weight Loss with a Combination Biphasic Ketogenic Mediterranean diet and Mediterranean Diet Maintenance Protocol by Paoli A et al ( Dr. Painter cited the paper by Zinn C et al, titled Assessing the Nutrient Intake of a Low-Carbohydrate, High-Fat (LCHF) Diet: a hypothetical case study design and highlighted that despite macronutrient proportions not aligning with current national dietary guidelines, that when well-designed a low carbohydrate diet provides all of the essential micronutrients needed by the body.
Dr. Painter cited the paper by Zinn C et al, titled Assessing the Nutrient Intake of a Low-Carbohydrate, High-Fat (LCHF) Diet: a hypothetical case study design and highlighted that despite macronutrient proportions not aligning with current national dietary guidelines, that when well-designed a low carbohydrate diet provides all of the essential micronutrients needed by the body. Dr. Painter cited the 2014 study by Bazzano LA et al, titled Effects of Low-Carbohydrate and Low-Fat Diets: a randomized trial which found that of the ~60 subjects randomized to either the low-carbohydrate diet (<40 grams/day) or low-fat diet (<30% of daily energy intake from total fat [<7% saturated fat]) which found that at 12 months, participants on the low-carbohydrate diet lost 3.5 kg more weight and lost 1.5% more fat mass, than those in the low-fat diet group.
Dr. Painter cited the 2014 study by Bazzano LA et al, titled Effects of Low-Carbohydrate and Low-Fat Diets: a randomized trial which found that of the ~60 subjects randomized to either the low-carbohydrate diet (<40 grams/day) or low-fat diet (<30% of daily energy intake from total fat [<7% saturated fat]) which found that at 12 months, participants on the low-carbohydrate diet lost 3.5 kg more weight and lost 1.5% more fat mass, than those in the low-fat diet group. Dr. Painter concluded his talk by saying that he feels that most low carbohydrate diets are ‘harmful in practice’ because they are low in fiber, but that that can be addressed by;
Dr. Painter concluded his talk by saying that he feels that most low carbohydrate diets are ‘harmful in practice’ because they are low in fiber, but that that can be addressed by;








